

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Curcumin is the main compound obtained from the rhizoma of Curcuma longa, also known as turmeric [1]. Curcumin displays a vibrant yellow color and thus is widely used as an additive in Indian food [2]. Curcuma longa has been used in Asian traditional medicine in the treatment of a variety of inflammatory disorders [3]. Furthermore, it has also been reported that curcumin exhibits antitumor, antioxidant, and antimicrobial activities [4]. It has been observed that curcumin is well tolerated after long-term use and at high doses [3,5]. However, adequately designed clinical studies specifically addressing curcumin safety are still lacking [6].
There is evidence that curcumin also appears to be an effective analgesic agent [7]. It has recently been reported that curcumin reduces pain and fatigue in patients undergoing laparoscopic cholecystectomy [8]. Animal studies have confirmed the efficacy of curcumin in pain relief. Systemic administration of curcumin induces significant antinociception in experimental models of neuropathic pain [9,10], acetic acid-induced visceral nociception [11], capsaicin-induced thermal hyperalgesia [12], and the formalin-induced orofacial pain test [13]. Several mechanisms of action have been proposed for the antinociceptive effects of curcumin, including suppression of brain nitrite and TNFα levels [9], activation of the descending monoamine system [10], blockade of TRPV1 activation [12], and desensitization of TRPA1 [14]. These hypotheses notwithstanding, however, the mechanism of antinociceptive action of curcumin has not yet been fully elucidated.
It has been reported that activation of ATP-sensitive potassium channels (KATP channels) antagonizes nociceptive responses evoked by noxious stimuli, dampening the hyperexcitability of the nociceptors [15]. There is evidence that the opening of KATP channels participates in the analgesic effect of the non-steroidal anti-inflammatory drugs ketorolac [16] and diclofenac [17, 18], but not in that of indomethacin [17]. There is also evidence that KATP channels play a role in the analgesic effect of a variety of agents such as morphine [19], clonidine [20] and 5-HT1 agonists [21], atrial natriuretic peptide (ANP) [17], and pregabalin [22]. Therefore, it appears that the opening of KATP channels is a common mechanism of antinociception.
There are several intracellular pathways that lead to the opening of KATP channels and to analgesia. Nitric oxide donors, such as sodium nitroprusside, activate the soluble form of guanylyl cyclase, resulting in the synthesis of cyclic GMP (cGMP), which in turn results in the opening of KATP channels and analgesia [23]. Ketorolac [16] and diclofenac [17] are able to produce antinociception by activation of the L-arginine-nitric oxide-cGMP-KATP channel pathway. On the other hand, ANP activates the particulate form of guanylyl cyclase [24], resulting in cGMP synthesis, which leads to KATP channel opening and antinociception [17]. There is also evidence that compounds that are able to directly open KATP channels, such as cromakalim [25] and pinacidil [17], result in pain relief. It is therefore possible that KATP channels are involved in the antinociceptive effect of curcumin. Hence, the purpose of this study was to examine whether KATP channel opening, and, in particular, the activation of the L-arginine-nitric oxide-cGMP-KATP channel pathway, is involved in curcumin-induced pain-relief.
Go to : 
MATERIALS AND METHODS
1. Animals
Female Wistar rats aged 8-9 weeks (weight range 200-220 g) from our own breeding facilities were used in this study [17,18]. The animals had free access to drinking water and were fasted for 18-20 hours before experiments. Efforts were made to minimize animal suffering and to reduce the number of animals used. Rats were used one time only. At the end of the experiments, the rats were sacrificed in a CO2 chamber. All experiments followed the Guidelines on Ethical Standards for Investigation of Experimental Pain in Animals [26] and the protocol was approved by the Institutional Animal Care and Use Committee (Center for Research and Advanced Studies of the National Polytechnic Institute, Mexico, DF).
2. Drugs
Curcumin, NG-nitro-L-arginine methyl ester (L-NAME), 1H-[1,2,4]oxadiazolo[4,3-a]quinoxaline-1-one (ODQ) and glibenclamide were purchased from Sigma Aldrich (St. Louis, MO, USA). Curcumin was suspended in carboxymethylcellulose (0.5% CMC). Glibenclamide and ODQ were dissolved in 20% dimethyl sulfoxide and L-NAME in isotonic saline.
3. Measurement of antinociceptive activity
Antinociception was assessed using the formalin test. Rats were placed in open Plexiglas observation chambers for 30 min. to allow them to accommodate to their surroundings; they were then removed for formalin administration. Fifty microliters of diluted formalin (1%) were injected subcutaneously into the dorsal surface of the right hind paw with a 30-gauge needle. Animals were then returned to the chambers and nociceptive behavior was observed immediately after formalin injection. Mirrors were placed behind each chamber to enable unhindered observation of the formalin-injected paw. Nociceptive behavior was quantified as the numbers of flinches of the injected paw during 1 min. periods every 5 min. for up to 60 min. after injection [25-28]. Flinching was readily identified and characterized as a rapid and brief withdrawal or flexing of the injected paw. Formalin-induced flinching behavior is biphasic [17,27-29]. The initial acute phase (0-10 min.) is followed by a relatively short quiescent period, which is then followed by a prolonged tonic response (15-60 min.). At the end of the experiment, the animals were sacrificed in a CO2 chamber.
4. Study design
Rats received vehicle or increasing oral doses of curcumin (3.1-100 mg/kg) by gavage 60 min. before formalin injection. In order to examine the participation of the NO-cGMP-KATP channel pathway in the antinociceptive effect of oral curcumin, rats were pretreated locally with L-NAME, an inhibitor of nitric oxide synthase, ODQ, an inhibitor of soluble guanylyl cyclase, or glibenclamide, a blocker of KATP channels [17,28,29]. Blockers dissolved in a volume of 50 µl were injected in the paw that was to be injured 10 min. before the insult, as described previously [17].
5. Data analysis and statistics
All results are presented as mean ± SEM. Curves were made by plotting the number of flinches against time. The area under the number of flinches against time curves (AUC) was calculated by the trapezoidal rule [17,28-30]. AUC was calculated for the two phases of the assay, and the percent of antinociception for each phase was calculated according to the following equation [30]:
Percent of antinociception = [(AUCvehicle - AUCpost compound)/AUCvehicle] × 100.
Analysis of variance followed by Tukey's test was used to compare the differences between treatments. Differences were considered statistically significant when P < 0.05.
Go to :
RESULTS
Local injection of 1% formalin produced a typical biphasic flinching behavior. The first phase was characterized by an immediate increase in flinching followed by a gradual decrease, to reach near-zero values after 10 min. A second flinching phase then occurred, being observed from 15 min. to 60 min. Oral curcumin administration did not have any significant effect on formalin-induced nociception during phase 1, but significantly reduced flinching during phase 2 (Fig. 1A). Therefore, only data from phase 2 were submitted for further analysis. Curcumin produced a dose-dependent reduction in the AUC of phase 2 (Fig. 1B). The effect of curcumin on the second phase of the formalin test can also be expressed as a dose-dependent increase in the percent of antinociception (Fig. 1C).
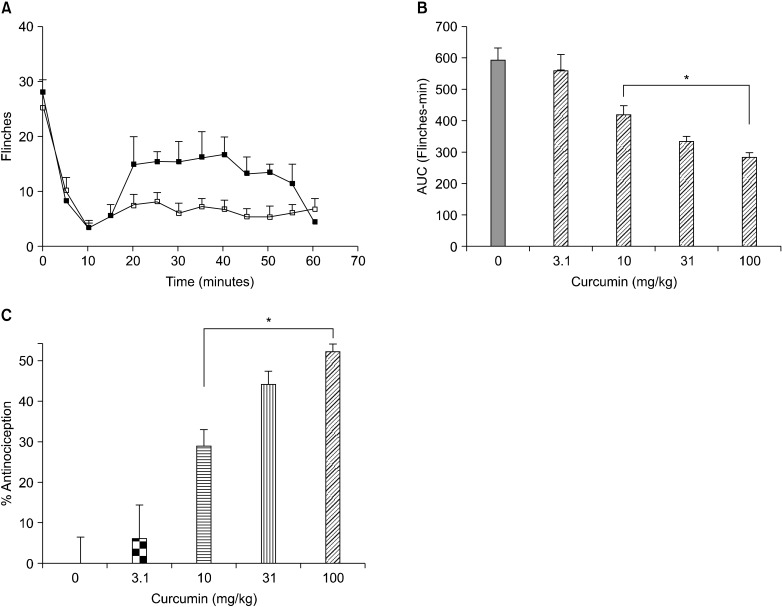 | Fig. 1(A) Flinching behavior observed after the intraplantar injection of 1% formalin in the right hind paw of Wistar rats in absence (black symbols) of in presence (open symbols) of 100 mg/kg oral curcumin. (B) Area under the number of flinches-against-time curve of the second phase of the formalin test observed in Wistar rats in presence of increasing doses of oral curcumin. (C) Percent of antinociception observed in the second phase of the formalin test in presence of increasing doses of oral curcumin. Data are presented as mean ± SEM of six animals. *Denotes a statistically significant difference (P < 0.05) with respect to the effect observed in absence of curcumin.
|
In an additional experimental series, it was observed that pretreatment with local injection of L-NAME or ODQ did not produce any significant change in oral curcumin-induced antinociception (Figs. 2A and 2B), while pretreatment with glibenclamide resulted in a dose-dependent reduction in the antinociceptive effect of 100 mg/kg oral curcumin (Fig. 2C).
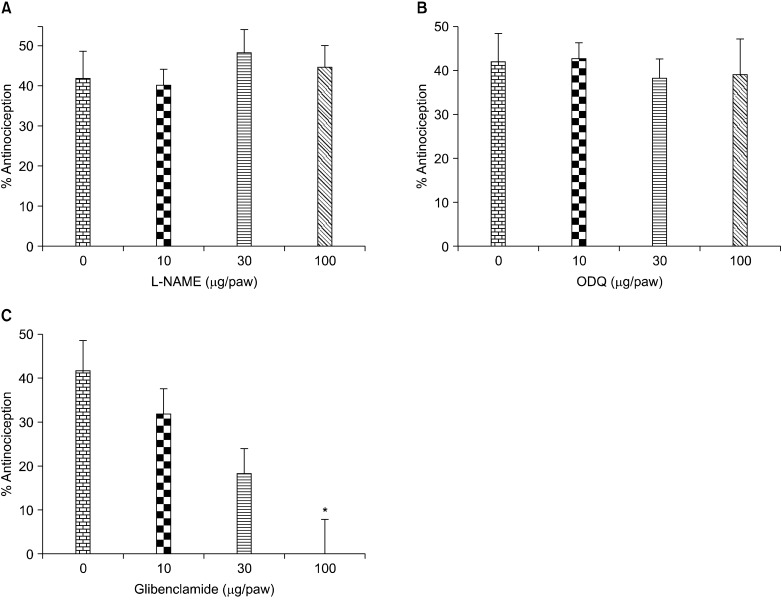 | Fig. 2Antinociceptive effect of 100 mg/kg oral curcumin in the second phase of the formalin test in Wistar rats submitted to local pretreatment with increasing doses of L-NAME (A), ODQ (B) and glibenclamide (C). Data are presented as mean ± SEM of six animals. *Denotes a statistically significant difference (P < 0.05) with respect to the effect observed in absence of glibenclamide.
|
Go to :
DISCUSSION
Curcumin, the main active ingredient of turmeric, exhibits several pharmacological actions [1-5]. It has been documented that curcumin exhibits a significant antinociceptive effect in a variety of experimental pain models [9-13]. Moreover, it has recently been reported that curcumin is effective in postsurgical pain [8] and therefore exhibits true potential as an analgesic agent in clinical practice [7]. Several mechanisms have been proposed to explain the antinociceptive effect of curcumin, including suppression of brain nitrite and TNFα levels [9], activation of the descending monoamine system [10], blockade of TRPV1 activation [12], and desensitization of TRPA1 [14]. However, the exact mechanism of action remains controversial [12]. Moreover, it is possible that the overall antinociceptive effect of curcumin involves multiple mechanisms of action, as is the case for several analgesic agents, such as diclofenac [31].
It is now well documented that the opening of KATP channels plays a role in the antinociceptive effect of a number of agents, including ketorolac [16], diclofenac [17,18], morphine [19], clonidine [20], 5-HT1 agonists [21], ANP [17], and pregabalin [22]. It is known that activation of KATP channels antagonizes nociceptive responses evoked by noxious stimuli, dampening the hyperexcitability of the nociceptors [15]. However, KATP channel opening is not a universal mechanism of antinociception. Several agents, such as indomethacin [17], acemetacin [32], and kappa opioid receptor agonists [33] induce a significant antinociceptive effect which does not involve the participation of KATP channels. In this study, we demonstrate that the activation of KATP channels is involved in the antinociceptive effect of curcumin.
KATP channels can be activated by several pathways. Compounds that directly open the channels, such as diazoxide [34], pinacidil [17], and cromakalim [33] produce a significant antinociceptive effect. KATP channel opening also occurs as a consequence of activation of Gi/o proteins, as is the case for µ- and δ-opioid agonists [33]. Moreover, an increase in intracellular cGMP also results in KATP channel opening and analgesia. This is observed after administration of dibutyryl-cGMP [34,35] or by activation of cGMP-generating pathways. ANP, which directly activates the particulate form of guanylyl cyclase, results in significant antinociception [17]. It is also well documented that activation of the L-arginine-nitric oxide-cGMP-KATP channel pathway results in antinociception. Administration of nitric oxide donors, such as sodium nitroprusside [23], induces a significant antinociceptive effect. KATP channel opening and antinociception is also induced by hydrogen sulfide [36].
Local administration of L-NAME, ODQ, or glibenclamide does not induce any significant alteration in formalin-induced nociception, suggesting that these compounds are devoid of any pro- or antinociceptive effects by themselves, although they can interfere with the antinociceptive action of several drugs [17,18,29]. In the present study, we observed that glibenclamide, but not L-NAME or ODQ, impairs the antinociceptive effect of oral curcumin. These results suggest that activation of KATP channels, but not by the L-arginine-nitric oxide-cGMP-KATP channel pathway, is involved in the antinociceptive effect of curcumin. Hence, curcumin may be directly stimulating KATP channels, activating Gi/o proteins, stimulating the particulate form of guanylyl cyclase, or acting through the hydrogen sulfide-KATP channel pathway. Further research is needed to fully elucidate this issue.
The local injection of glibenclamide in the same site as the formalin insult was able to significantly reduce the antinociceptive effect of oral curcumin. There is evidence that glibenclamide is able to block drug-induced antinociception after local and spinal administration [17,29], but also after systemic administration [18]. Hence, our results provide evidence that curcumin-induced antinociception involves the participation of KATP channels at the peripheral level, although additional systemic mechanisms of action may also be involved.
Recently, Han and coworkers reported that intrathecal administration of curcumin produces antinociception in the formalin test [37], demonstrating that this agent is also able to produce antinociception by central mechanisms. There is evidence that curcumin is able to pass through the blood-brain barrier [38]. Therefore, it is likely that the overall antinociceptive effect of curcumin after systemic administration involves both peripheral and central actions, as is the case for non-steroidal anti-inflammatory drugs and opioids [31]. Furthermore, for several agents, such as diclofenac [28] and lumiracoxib [29], we have shown that both the peripheral and central actions include the participation of KATP channels.
In summary, the present results confirm that curcumin is an effective antinociceptive agent. Our data provide evidence for the participation of peripheral mechanisms, including KATP channel opening, in addition to other mechanisms of action. The complete elucidation of the mechanisms of action of the antinociceptive effect of curcumin will certainly bolster its potential as an analgesic agent in clinical practice.
Go to :
 XML Download
XML Download