

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Fibromyalgia is a disease with characteristic chronic diffuse pain caused by a decrease in the pain threshold [1]. However, there are many cases where diagnosis is difficult due to unclear causes of the disease and symptoms other than pain, such as fatigue, sleep disturbance, etc., which are common in fibromyalgia along with pain in the overall body and specific tender points [2,3].
Up to now, the classification criteria suggested by the American College of Rheumatology (ACR) in 1990 had been used in the diagnosis of fibromyalgia. According to these criteria, there has to be left, right, top, bottom of body and axial skeletal chronic whole body pain for at least 3 months, and 11 or more tender points from the 18 tender points to be diagnosed as fibromyalgia [4]. However, the tender point test is measuring the pain felt when an equal pressure of 4 kg is applied accurately to a tender point each time, so the test can be inconsistent. There are also cases where 11 or more tender points are not fulfilled so there are limitations in objectivity and usefulness as diagnostic criteria [3,5]. In addition, extra-pain symptoms are a major symptom of fibromyalgia [6], but there is no mention of extra-pain symptoms in the 1990 ACR classification criteria. Currently, the Fibromyalgia Impact Questionnaire (FIQ) and pain VAS (visual analogue scale) is additionally performed in diagnosis and there is follow-up observation for the assessment of extra-pain symptoms, but detailed agreement or treatment guidelines are insufficient.
To supplement the above-mentioned problems of the existing classification criteria, ACR suggested new preliminary classification criteria. The 2010 ACR preliminary classification criteria diagnoses fibromyalgia as the sum of widespread pain index (WPI) and total symptom severity (SS) being more than a certain score, continuing symptoms for more than 3 months, and all three criteria without disease related to symptoms being satisfied. These criteria do not include a tender point test, and the patient is to indicate the location and severity of the pain as well as the extra-pain symptoms. In addition, the WPI and SS have numerical values so objective diagnosis and follow-up observations are possible [7].
However, the preliminary classification criteria presented were not intended for Korean patients so there is need to evaluate whether clinical application to actual Korean patients is suitable. The aim of this study was to examine whether the fibromyalgia preliminary classification criteria suggested by the ACR in 2010 was useful in effectively diagnosing FM compared to the 1990 classification criteria. In addition, the study examined whether other assessment indicators such as FIQ or pain VAS, which had been used until now without detailed agreement, could be replaced by WPI and SS.
Go to : 
MATERIALS AND METHODS
1. Subject
The study was conducted on 98 patients diagnosed with fibromyalgia and had been under treatment for six months from June to November 2010 who gave consent to the study. This study was performed after passing the IRB review of Konkuk University (KUH1010208).
2. Method
1) Selection criteria
Patient selection criteria were patients who had diffuse whole body pain for 3 months or more together with 11 or more tender points according to the 1990 ACR classification criteria during the research period, or patients who did not satisfy the 11 tender points but were suspected of fibromyalgia in clinical examination and had a FIQ of 40 or more. Patients with other diseases related to pain such as thyroid disease, osteoarthritis, or rheumatoid arthritis were excluded from the study.
2) Questionnaire and diagnosis method
A diagnosis according to the 1990 ACR fibromyalgia classification criteria was given when the pain period was 3 months or more and there were 11 tender points among the 18 tender points. A diagnosis according to the 2010 ACR preliminary classification criteria was given when the three suggested diagnosis criteria were all satisfied. The first diagnosis criteria in the 2010 ACR preliminary classification criteria is the sum of the WPI which represents a subjective number from the 19 whole body pain areas and the SS which represents the degree and type of extra-pain symptoms (Table 1, 2). From these, the SS consists of SS-1, which numerically represents the degree of pain, and the SS-2, which numerically represents the number of various extra-pain symptoms. The sum of the WPI and SS were again categorized into WPI ≥ 7 and SS ≥ 5, or WPI 3-6 and SS ≥ 9. When patients corresponded to any of the two criteria, they satisfied the first diagnosis criteria. The second criteria of the 2010 ACR preliminary classification criteria was suffering from the disease for 3 months or more, and the third criteria was when there were no other incidents or diseases related to the symptoms. A final diagnosis with the 2010 ACR preliminary classification criteria was given when the patient corresponded to all three criteria above. The medical team applied 4 kg of pressure on the 18 tender points according to the 1990 ACR classification criteria on the selected patients for the study and recorded the results. The patients were also asked to answer the 2010 ACR preliminary classification criteria survey and FIQ questionnaire. The collected data were categorized into sex, age, FIQ, pain VAS, 1990 ACR classification criteria, and the 2010 ACR preliminary classification criteria for statistical analysis. Pain VAS was expressed as "0" when there was no pain, and "10 mm" when the pain was the most severe pain imaginable.
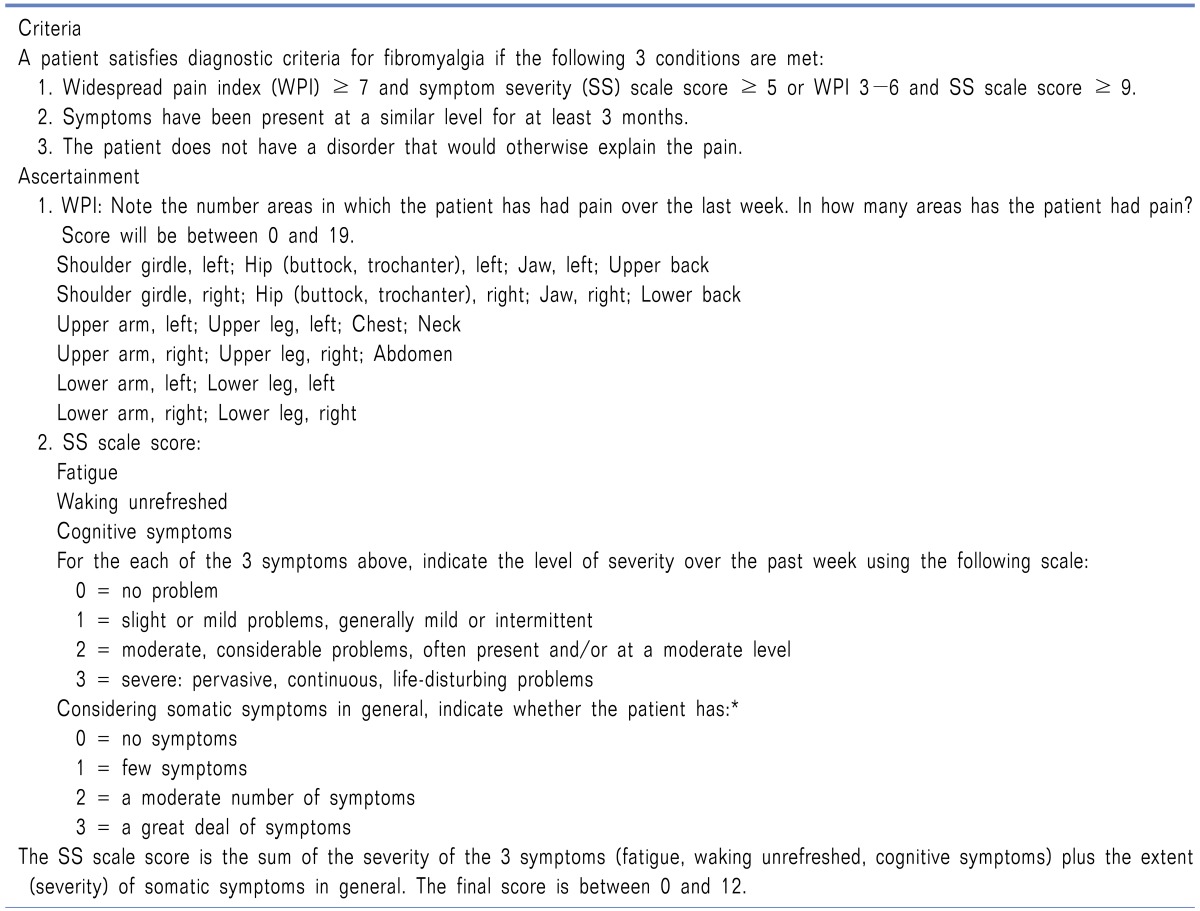
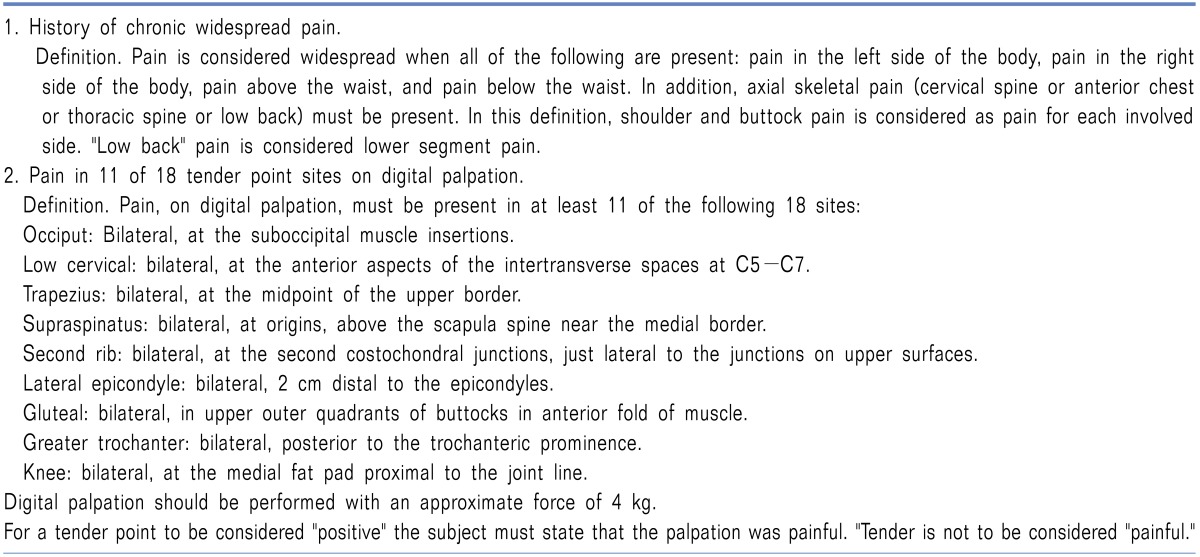
Table 2
The 2010 American College of Rheumatology Diagnostic Criteria
*Somatic symptoms that may be considered include muscle pain, irritable bowel syndrome, fatigue/tiredness, thinking or remembering problems, muscle weakness, headache, pain/cramps in the abdomen, numbness/tingling, dizziness, insomnia, depression, constipation, pain in the upper abdomen, nausea, nervousness, chest pain, blurred vision, fever, diarrhea, dry mouth, itching, wheezing, Raynaud's phenomenon, hives/welts, ringing in ears, vomiting, heartburn, oral ulcers, loss of/change in taste, seizures, dry eyes, shortness of breath, loss of appetite, rash, sun sensitivity, hearing difficulties, easy bruising, hair loss, frequent urination, painful urination, and bladder spasms. Adapted from reference [19].
![]()
3. Statistical analysis
SPSS 17.0 was used for statistical analysis. Frequency analysis, cross tabulation, and independent sample t-test were performed to compare the 1990 ACR classification criteria and the 2010 ACR preliminary classification criteria. Pearson correlation analysis was performed to determine if there were correlations between the diagnosis criteria categories.
Go to :
RESULTS
1. Clinical characteristics
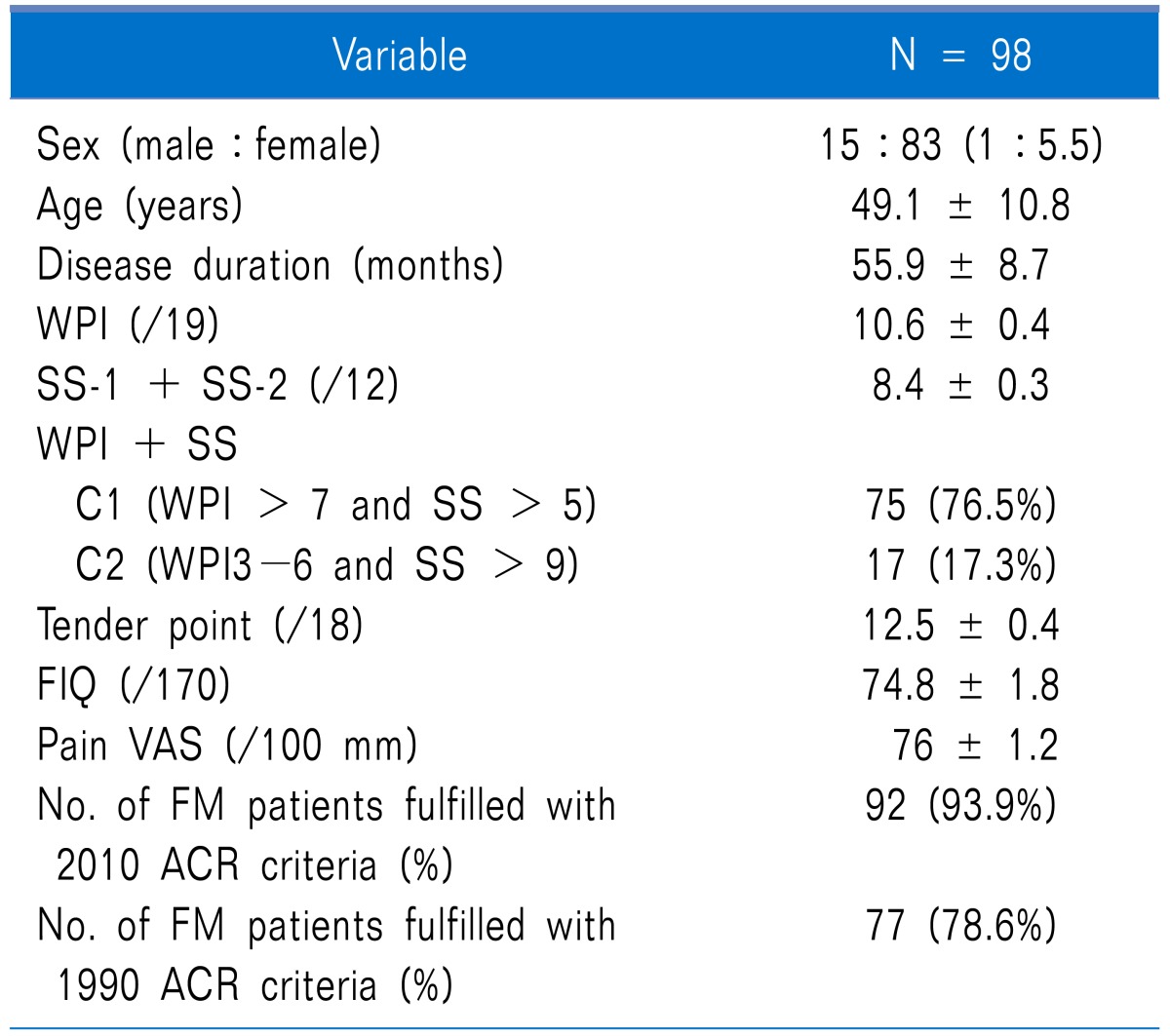
There were 15 males and 83 females in the study population so there were more female patients. Mean age was 49.1 ± 1.0 (24-76) so the patients were mostly middle age, and the mean disease period was slightly long at 55.9 ± 8.7 months. The mean number of tender points was 12.5 ± 0.4. The mean WPI was 10.6 ± 0.4 (total, 19), and the mean sum of the SS was 8.4 ± 0.3 (total score, 12). The mean FIQ was 74.8 ± 1.8 and the mean Pain VAS was 76 ± 1.2 mm (Table 3).
2. Frequency analysis of the two diagnosis criteria
There were 77 patients (78.5%) who satisfied the 1990 ACR fibromyalgia classification criteria and 92 patients (93.8%) who satisfied the 2010 ACR preliminary classification criteria, so there were more patients who satisfied the 2010 criteria. From these, the number of patients who satisfied both criteria was 71 (72.4%). From the patients who did not satisfy the 1990 criteria, 21 patients (21.5%) were diagnosed with fibromyalgia according to the 2010 ACR preliminary classification criteria (Table 4).

3. Patient analysis according to the 1990 ACR classification criteria
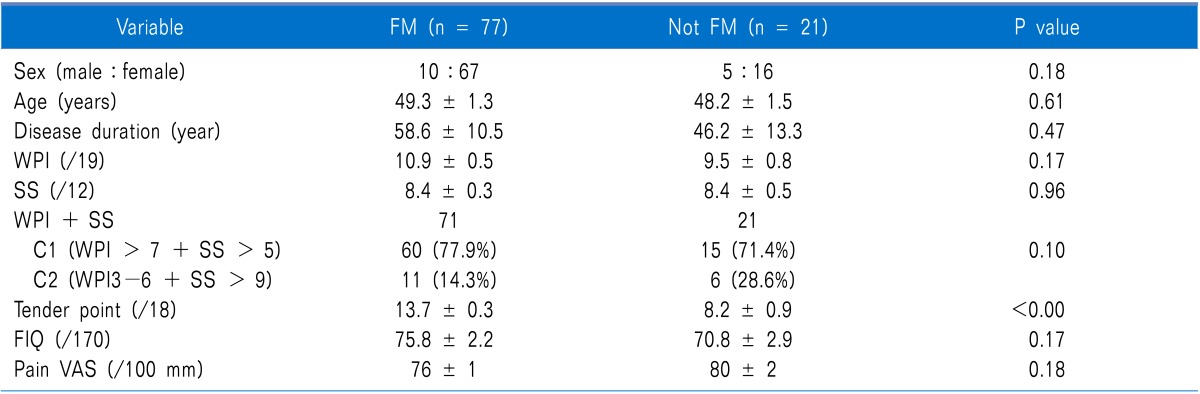
Among the patients who satisfied the 2010 ACR fibromyalgia preliminary classification criteria, 71 met the 1990 ACR classification while 21 did not. This means that there was a higher number of patients who satisfied the 1990 criteria than those who satisfied the 2010 criteria. The mean FIQ of the patients who satisfied the 1990 ACR classification criteria was 75.8 (± 0.5), which was 1.4 points higher than those who satisfied the 2010 ACR classification criteria. The FIQ, pain VAS, WPI in the patients who satisfied the 1990 ACR classification criteria were high, but when compared to those who did not satisfy the classification criteria, the difference in values failed to reach statistical significance. However, the tender points were significantly different between the patients who satisfied the 1990 ACR classification criteria and those who did not (Table 5).
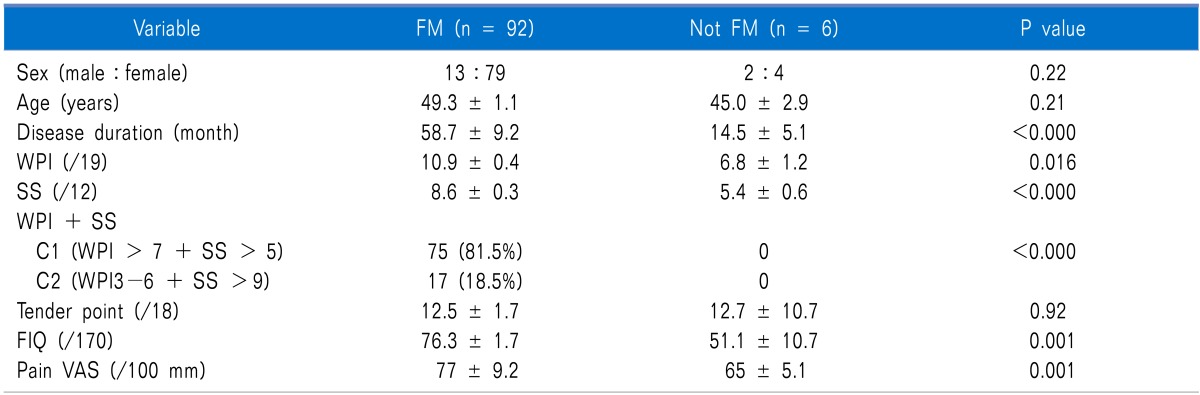
4. Patient analysis according to 2010 ACR preliminary classification criteria
The male to female ratio of patients diagnosed with fibromyalgia according to the 2010 ACR preliminary classification criteria was 1:6.1, and the mean age was 49.3 ± 1.1, so there was no difference in the basic demographics of the patients who satisfied the 1990 classification criteria. The mean disease duration of the patients who satisfied the 2010 ACR preliminary classification criteria was 58.7 months (± 9.2), which was 44 months longer than the patients who did not (P < 0.001). The mean WPI was 10.9 (± 0.4), and this value is 4.1 points higher than the mean WPI in the patients who did not satisfy the criteria (P = 0.016). The mean SS was 8.6 (± 0.3), which was also 3.2 points higher (P < 0.000). As for the sum of the WPI and SS which was the first criteria of the 2010 ACR preliminary classification criteria, 81.5% of the patients were classified as WPI > 7 + SS > 5, which was more than the 63% of the patients who were classified as WPI3-6 + SS > 9 (P < 0.000). The mean number of tender points of patients who satisfied the 2010 ACR preliminary classification criteria was 12.5 ± 1.7, and there was no significant difference between those who did and those who did not satisfy the criteria. However the mean FIQ of patients who satisfied the 2010 ACR preliminary classification criteria was 76.3 (± 1.7), which was 24 points higher (P = 0.001) and the pain VAS was 77 (± 9.2) mm, which was 12 mm higher than in the patients who did not satisfy the criteria (P = 0.001). The mean WPI of patients who satisfied the 2010 ACR preliminary classification criteria was 10.9 (± 0.4), which was also 4.1 points higher than in the patients who did not satisfy the criteria (P = 0.016) (Table 6).
5. Correlation between each classification criteria
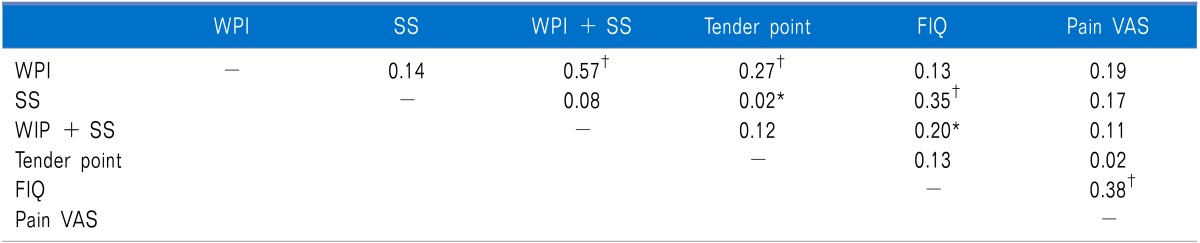
Upon investigating the correlations between the different categories of the 2010 ACR preliminary classification criteria, we found that the number of tender points had a positive relationship with the WPI (r = 0.27, P < 0.001), and FIQ with SS (r = 0.35, P < 0.001). While pain VAS showed a weak correlation with other categories in the 2010 ACR preliminary classification criteria, the FIQ showed a significant positive correlation (r = 0.38, P < 0.001) (Table 7).
Go to :
DISCUSSION
The prevalence of chronic whole body pain in Korea is about 14%, so it is slightly higher than the prevalence in other countries known to be generally at about 10% [8]. Fibromyalgia is known as a common cause for chronic diffuse whole body pain; it is more common in females than males, and it increases with age so the risk at the age of 80 or higher is reported to be 10.9 times higher [9,10]. When the prevalence of fibromyalgia in other countries was examined, England was at 11% [11], Germany at 14% [12], and the USA was reported at 11% in 1995 [9]. However, the prevalence of fibromyalgia in Korea is reported to be about 2.2% in a research conducted in 2 rural areas of Gyeongsangbuk-do, so it is extremely low compared to foreign countries [4]. The elderly population is rapidly increasing in Korea, and in elderly patients, fibromyalgia appears in combination with other diseases, so in many cases, it is diagnosed only as myalgia [13]. It is presumed that the prevalence rate of actual fibromyalgia in Korea is higher than reported. The preliminary classification criteria presented by the ACR in 2010 can be an alternative for this diagnostic situation in Korea. In our study, patients diagnosed with fibromyalgia according to the 2010 preliminary classification criteria was 93.9% of the patients, which was more than the 78.6% diagnosed according to the classification criteria of 1990. In addition, 21.4% of the patients who had been excluded from the diagnosis according to the 1990 classification criteria were diagnosed with fibromyalgia by the 2010 preliminary classification criteria. On the other hand, patients who had not satisfied the 2010 preliminary classification criteria but was diagnosed with fibromyalgia by the 1990 classification criteria were only 6.1% of all the patients (P = 0.003). This result can be interpreted as 21.4% of the patients who had been excluded from 1990 classification criteria were newly diagnosed with fibromyalgia according to the 2010 preliminary classification criteria. The additional 21.4% of patients is believed to be because of the extra-pain symptoms that had been overlooked in the 1990 classification criteria and was included in the 2010 preliminary classification criteria as the SS category. The FIQ had been used as an additional assessment regarding extra-pain symptoms clinically, and in the correlation test in this study, the FIQ and SS had a significant correlation (r = 0.35, P < 0.01). Extra-pain symptoms of fibromyalgia were not included in the 1990 ACR classification criteria despite it being a major symptom of this disease, so a large number of patients had not been diagnosed. Therefore, the application of the 2010 preliminary classification criteria, which includes the extra-pain symptoms in the diagnosis, can diagnose many more patients with fibromyalgia who had not been diagnosed before.
The 1990 ACR fibromyalgia classification criteria defines it as when there is left, right, top, below whole body pain for 3 months or more and 11 or more tender points among 18 [5]. However, this classification criteria has several problems in diagnosing fibromyalgia. First, the number of tender points cannot be an objective assessment of whole body pain. Tender points can be mistaken for trigger points for myofascial pain syndrome or pain from other disease such as osteoarthritis, and generally, females are more sensitive to pain than males so they show a tendency to respond to more tender points [5]. Therefore, when the number of tender points is used as the main diagnostic information for fibromyalgia, there is a chance to mistake another disease for fibromyalgia. In addition, the difference in tender points between sexes is ignored so there can be problems in deducing the objectiveness of the diagnosis. Second, since the tender point test is the main information for the diagnosis, the major mechanism of fibromyalgia can be mistaken as a muscle disorder rather than a neurological disorder [14]. Third, the number of tender points, 11 or more, might not be an accurate range limit in confirming the diagnosis. There have been many patients who were actually clinically diagnosed with fibromyalgia with the number of tender points being lower than 11, and some specialists diagnose fibromyalgia with "fibromyalgia inclination diagnosis" which does not fixate on the number of tender points [15]. Fourth, it is difficult for the examiner to assess each of the 19 tender points with an equal pressure of 4 kg/cm2 using the index finger, and objectivity is also difficult to obtain. In some clinics, a pressure gauge is used instead of a finger but this method is also difficult to implement in busy Korean clinics. Fifth, as fibromyalgia is diagnosed only with a duration period of whole body pain and the number of tender points, it is devoid of assessing any extra-pain symptoms, which is characteristic of this disease. The tender point test is not included in the 2010 preliminary classification criteria. Therefore, if this preliminary classification criterion is applied in Korea, it is expected that it will save time and effort for the examiner in the busy reality of Korea clinics with many outpatients, and can also overcome the limitations of the tender points mentioned above.
In our study, the number of tender points had a significant correlation with the WPI of the 2010 preliminary classification criteria (r = 0.27, P < 0.01). The WPI is a numerical expression of subjective pain as the patient records the subjective pain area themselves, and there is relatively good correlation between the WPI expressed subjectively by the patients and tender point examination assessed objectively by the examiner. These research results mean that the tender point test can be substituted with the WPI in the 2010 ACR preliminary classification criteria also in Korea.
The main characteristic of fibromyalgia is whole body pain, but most patients also are accompanied with extra-pain symptoms such as severe fatigue, sleep disturbance, weakness, depression, anxiety, headache, irritable bowel syndrome, abnormal menstruation, and urinary incontinence [16-18]. When patients with chronic polymyalgia pain complain of such extra-pain symptoms, fibromyalgia can be the most convincing diagnosis than other overlapping pain syndromes [19]. Currently, FIQ developed by Burckhardt and pain VAS are additionally used in the diagnosis and treatment effect assessment of fibromyalgia for these extra-pain symptoms [20]. However, FIQ is used without detailed agreement, and was developed for female fibromyalgia patients so there could be sexual bias [21,22]. For example, many categories can be assessed differently according to sex or life pattern such as "Can you do the dishes or the laundry?" or "Can you go shopping?" In addition, FIQ consists of ambiguous expressions so there has been criticism that there is a lack of understanding regarding functional disorders [23,24]. The SS in the 2010 preliminary classification criteria divides and numerically represents the degree and type of extra-pain symptoms into SS-1 and -2. In this study, the FIQ showed significant correlation with sum of WPI and SS as well as SS (r = 0.35, P < 0.01; r = 0.20, P < 0.05). Similar results were obtained from the analysis of the first patient diagnoses, and these results can be used as a basis for suggesting the possibility of the SS substituting the FIQ in the diagnosis of fibromyalgia patients in Korea.
Fibromyalgia can accompany other diseases. Common diseases that accompany fibromyalgia are rheumatic diseases such as Sogren syndrome, systemic lupus erythematosus, and infectious disease such as tuberculosis, and endocrine disease such as hyperparathyroidism [25]. According to one study, it has been reported that 29% of rheumatoid arthritis patients and 33% of osteoarthritis patients have accompanying fibromyalgia. However, there is nearly nothing known yet on the mechanism for fibromyalgia developing in the presence with other diseases, and there has been debate whether it is suitable to diagnose whole body pain, which accompanies other diseases, as fibromyalgia even though it may satisfy the 1990 fibromyalgia classification criteria [26]. The third criterion of the 2010 ACR preliminary classification criteria is the absence of any other incidents or diseases that may be related to the symptoms. The purpose of this criterion is to exclude cases in which many patients who satisfied the 1990 classification criteria had other diseases and they did not notify the medical team, and in cases in which other diseases were combined and the patients received an ambiguous diagnosis and treatment. According to the 2010 ACR preliminary classification criteria, ambiguous whole body pain combined with other diseases can no longer be diagnosed as fibromyalgia.
Fibromyalgia includes individual psychobehavioral characteristics. This characteristic appears as extra-pain symptoms with individual variation, and this variety is a factor that makes it difficult to research and develop treatment for fibromyalgia [27]. In one study, the various individual psychobehavioral characteristics were combined in an effort to separate and understand them in several groups [28]. The 2010 ACR preliminary classification criteria can be seen to include such individual psychobehavioral characteristics into the diagnostic criteria. The second criterion, SS, in the 2010 ACR preliminary classification criteria numerically represents the degree of relevant symptoms from 41 various physical symptoms along with the individual degree of 3 major extra-pain symptoms of fatigue, waking un-refreshed, and cognitive symptoms. This composition not only deals with the extra-pain symptoms of fatigue, sleep disturbance, and cognitive symptoms, but also deals with the various psychobehavioral characteristics that can appear according to individual variation by suggesting 41 somatic symptoms. In addition, by suggesting flexible and various symptoms that are not standardized and by inducing patients to numerically express the severity, it allows the patients to effectively complain of their symptoms in a short time and with no effort. According to our research results, the 2010 ACR preliminary classification criteria with the SS showed no mean difference between patients who satisfied the 1990 ACR classification criteria and those who did not (8.4 ± 0.3 vs 8.4 ± 0.5, P = 0.96); however, there was significant difference in the mean values of patients who satisfied the 2010 preliminary classification criteria and those who did not (8.6 ± 0.3 vs 5.4 ± 0.6, P < 0.001). Therefore, it is expected that the SS can be used as a useful assessment criteria that can reflect various individual psychobehavioral characteristics in domestic fibromyalgia patients.
According to a recent research result, the sensitivity of the 2010 ACR preliminary classification criteria reached 82% and specificity reached 91% [29]. This is high compared to the specificity of the 1990 ACR classification criteria, which was 81.1%. The 2010 ACR preliminary classification criteria are simpler and easier to diagnose fibromyalgia compared to the 1990 ACR classification criteria, and do not lack in sensitivity and specificity.
The limitations of this study is that it was not conducted on only first diagnosis patients, so patients who already had improved symptoms at the time of diagnosis were included. Due to this problem, it could be that there was no significant difference in WPI or SS in the analysis according to the 1990 classification criteria. If a comparative study is conducted on first diagnosis patients with initial symptoms who have not started treatment, it is expected that the WPI or SS would show significant differences in the analysis according to the 1990 classification criteria. Therefore, it is believed that there is a need for a comparative analysis regarding the 1990 classification criteria and the 2010 preliminary classification criteria conducted on only first diagnosis patients. The second limitation of this study is that a relatively small number of patients were examined over a short period. If the research is conducted on more patients over a longer period, a more significant P value may be obtained. The third limitation is that it is an analysis study of only one aspect without follow-up investigation according to the course of treatment. The 2010 ACR preliminary classification criteria can numerically express various criteria so it is composed to be useful in observing the course of treatment as well as for the diagnosis. However, our study only focused on the diagnosis and compared the two criteria of 1990 and 2010, so there was no review on whether the 2010 ACR preliminary classification criteria can be utilized in the follow-up observation of domestic patients. However, to introduce and use the 2010 ACR preliminary classification criteria in our country, it is believed that research regarding its usefulness in follow-up observation as well as in diagnosis is necessary. Therefore, there is a need for a useful analysis of the 2010 ACR preliminary classification criteria as a new diagnosis criteria through a long term, large-scale prospective study conducted on first diagnosis patients for it to be introduced in Korea.
This study applied the fibromyalgia preliminary classification criteria newly suggested by the ACR in 2010 to domestic patients, for a comparison with the existing 1990 classification criteria, to examine whether the 2010 ACR preliminary classification criteria is useful as a new diagnosis criteria. The analysis results showed that the 2010 ACR preliminary classification criteria provided a basis to diagnosis 21.4% of the patients who had not satisfied the 1990 classification criteria. In addition, the tender point test was unnecessary so time and effort was saved, and the SS, which includes the concept of extra-pain symptoms, had a significant correlation with the FIQ so a basis for its substitution was also provided. The 2010 ACR preliminary classification criteria numerically represented extra-pain symptoms as well as pain so a more objective assessment is possible. However, the various suggested extra-pain symptoms need to be confirmed in that they are relevant to domestic patients; therefore, a large scale prospective study is necessary.
It is expected that the 2010 ACR preliminary classification criteria will include more patients in the fibromyalgia diagnosis than the 1990 classification criteria. However, the 2010 preliminary classification criteria has a completely different composition to the existing classification criteria, so using both diagnosis criteria in diagnosing fibromyalgia until more accurate research regarding each category of the preliminary classification criteria is done will be necessary to heighten the specificity of the diagnosis from a complementary aspect.
Go to :
 XML Download
XML Download