

 PDF
PDF Citation
Citation Print
Print


Methods to identify the epidural space in epidural puncture include loss of resistance technique to air or normal saline, hanging drop method [1], ultrasound-guided method [2-4], pressure-guided method [5], drip infusion method [6,7], Queckenstedt test method [8], and use of acoustic device [9], or nerve stimulator [10]. Among these, loss of resistance technique is used most frequently. In this report, epidural anesthesia failed while performing high level thoracic epidural anesthesia for arteriovenous bridge graft of the upper arm in a chronic renal failure patient even though loss of resistance technique, hanging drop method, and drip infusion method were all successful.
We report a case in which an epidurogram and cervical and thoracic computed tomography were performed to verify the location of the epidural catheter; the result showed that the catheter had failed to penetrate through the ligamentum flavum and had been positioned in the T2 lamina erecter spinae muscle.
CASE REPORT
The 67-year old, male patient (164 cm, 70 kg) with chronic renal failure was supposed to undergo arteriovenous bridge graft of the upper arm for hemodialysis under high level thoracic epidural anesthesia. Patient history revealed that he underwent coronary bypass graft six years ago and was taking antihypertensive agents and insulin for hypertension and diabetes. Blood tests performed after hemodialysis on the day before the operation showed hemoglobin 11.3 g/dl, hematocrit 36.3%, glucose 202 mg/dl, Na 136 mmol/L, K 5.2 mmol/L, Cl 97 mmol/L, BUN 43 mg/dl, and creatinine 4.5 mg/dl. Test results on the day of the operation showed that the platelet count and coagulation profile (prothrombin time, International Normalized Ratio, activated partial thromboplastin time, fibrinogen) were in the normal ranges.
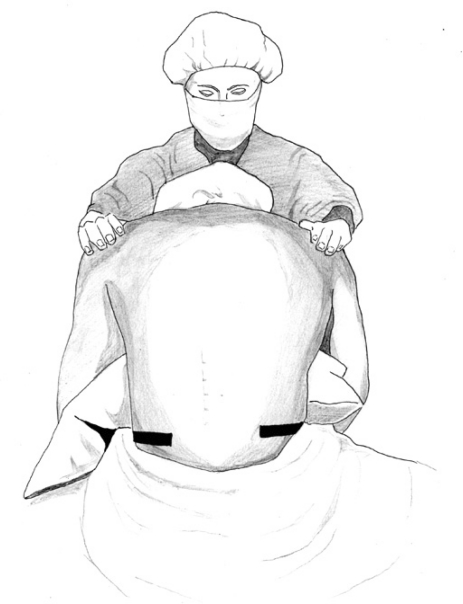
When the patient arrived at the operation room, blood pressure was 135/89 mmHg, and heart rate was 64 bpm. The high level thoracic epidural anesthesia was performed in the sitting position, and an assistant supported both shoulders of the patient so that the patient could lower his head to the maximum (Fig. 1). The first prominent spinous process of the cervical spine, which is the C6 spinous process, was identified [11]. Referring to that, local infiltration of 2% lidocaine 2 ml was performed in the middle line between the T1 and T2 spinous processes. Then, for the loss of resistance technique, a 5 ml glass syringe was connected to a 17-G Tuohy needle (ARROW®, Arrow International Inc., USA), and the needle was moved to the epidural space by the midline approach. When it moved into the 4.5 cm position from the skin, the plunge of the glass syringe was sucked inside, and the hanging drop method was performed at that position. As a result, the epidural space was positively identified, the loss of resistance technique to air was performed to verify that the loss of resistance was positive, and the drip infusion method showed that the normal saline was dropping at a rate of one drop per second or higher.
After that, an 18-G epidural catheter (ARROW®, Arrow International Inc., USA) was inserted through the Tuohy needle. The epidural catheter was inserted without particular resistance up to 3 cm inside the epidural space. After fixing the catheter, the patient's position was altered to the supine position, and 1% lidocaine 3 ml containing 1:200,000 epinephrine was injected through the catheter as the test dose. There was no change in blood pressure and heart rate at five minutes after the test injection. The sensory change on both upper arm medial sides was not accurately verified since the patient was unable to cooperate well. For epidural anesthesia, a mixture of 0.375% ropivacaine 15 ml and fentanyl 50 µg was injected through the epidural catheter. Pin-prick tests at 5, 10, 15 and 20 minutes after drug injection showed that pain had not been alleviated at all, and vital signs were not changed.
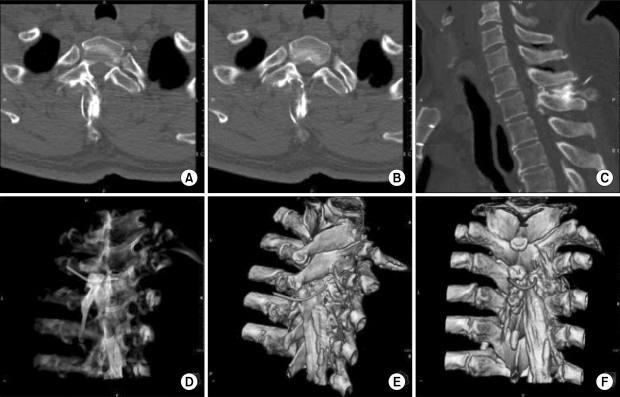
Judging that the epidural anesthesia failed, general anesthesia was performed under the agreement of the patient. To induce general anesthesia, 2% lidocaine 2 ml-propofol 2 mg/kg-atracurium 0.6 mg/kg was intravenously injected, and the anesthesia was maintained with O2-N2O-desflurane. The operation was carried out for 1.5 hours, and epidural anesthesia failure was reconfirmed when the patient complained of pain in the operated region in the recovery room. To find out the causes of the epidural anesthesia failure, iohexol 5 ml was injected through the epidural catheter and radiographic images were taken (Fig. 2). However, since the accurate position of the catheter was not found, cervical and thoracic computed tomography (CT) was performed after ensuring the patient that the hospital would cover the cost of the CT and receiving agreement from the patient and caregiver. CT findings revealed that the catheter had entered between T1 and T2 but failed to penetrate into the ligamentum flavum, proceeded along the T2 right lamina, and was eventually positioned within the erecter spinae muscle after converting the direction backwards (Fig. 3).
DISCUSSION
Anesthesiologists sometimes experience a situation where epidural anesthesia fails even when the loss of resistance and hanging drop methods have been successful and the catheter has been inserted without any particular difficulty [12].
Rissanen [13] and Sharrock [14] reported that pseudo loss of resistance or false positive loss of resistance may appear when the Tuohy needle is advanced to a region where a cavity has been formed due to degeneration of the interspinous ligament. Gupta et al. [15] reported pseudo positive loss of resistance due to subcutaneous emphysema generated after chest damage. Lirk et al. [16] reported that embryologically generated fissures from the lack of midline fusion of ligamentum flavum were found in the cervical spine region about 51-74% and thoracic vertebra region about 2-21%, respectively, and the mean area of fissures was 1.0 ± 0.3 mm. They also mentioned that the uncertain loss of resistance that takes place by such a fissure can probably cause dural puncture or spinal cord damage.
To solve this problem, Kil et al. [2] measured the depth of the epidural space by means of ultrasonic waves before operation children and infants aged seven or less, applied the drip infusion method for epidural puncture and reported that epidural puncture was successful by one-time trial in 179/180 patients (99.4%). Yamashita and Tsuji [17] applied the drip infusion method to identify the epidural space in 350 infants (300 in the spinal region and 50 in the thoracic vertebra region) under the age of nine and reported that it was accurately performed in 342 infants (97.7%).
However, in our case, although we performed the drip infusion method to avoid the problems of pseudo positive loss of resistance method listed previously, the Tuohy needle was unable to penetrate through the ligamentum flavum, the catheter deviated to the spinal lamina region at the entrance of the ligamentum flavum, and it proceeded into the near erecter spinae muscle, as revealed by cervical and thoracic CT. The methods used to verify accurate needle placement - hanging drop, loss of resistance, and drip infusion - were performed in the space just before the ligamentum flavum. Thus, the operator mistakenly considered this to be the epidural space and inserted the catheter, which led to the failure of the epidural anesthesia. The reason why the results from all three methods were found to be positive is unclear. As described previously, possible causes include the accompaniment of interspinous ligament degeneration or tissue breakdown by fluid overload due to chronic renal failure [18].
Clinically, epidural anesthesia sometimes fails even when the loss of resistance and hanging drop tests show positive results, and the catheter is inserted without any particular difficulty. Although C-arm guidance is employed from time to time, it is undeniably true that epidural anesthesia is most often performed without an imaging instrument. We identified the causes of epidural anesthesia failure using CT and recommend the use of C-arm guidance for epidural anesthesia, if possible, to reduce the frequency of pseudo positive cases of the loss of resistance.

 XML Download
XML Download