

 PDF
PDF Citation
Citation Print
Print


Invasive treatment of chronic pain emanating from joints is often difficult because of the complex anatomy of nerve supply. In most joints, the innervation is derived from several segmental levels, with multiple peripheral nerve branches entering the joint capsule [1]. Radiofrequency treatment has been used empirically for the management of different chronic pain syndromes, based on the assumption that thermocoagulation of the nerve fibers will interrupt pain conduction [2]. This report describes three cases in which patients experienced little or moderate satisfaction with pulsed radiofrequency lesioning of the glenohumeral joint.
All 3 patients were referred from the physical medicine or orthopedics departments to our pain clinic. None had experienced trauma to the shoulder or undergone surgery, and all 3 were taking oral opioid medication. They suffered from pain throughout the day, particularly aggravated at night and by movement. The pain was moderately responsive to oral analgesics, but all 3 patients had severe restrictions on activities of daily living. Despite physical therapy, they experienced little improvement in range of motion.
CASE 1
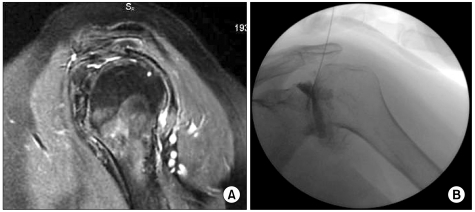
A 70-year-old woman was referred from physical medicine to our pain clinic with the diagnosis of general osteoarthritis and osteoporosis. She had undergone 4 sessions of physical therapy with oral analgesics during a 5-year period because of painful glenohumeral osteoarthritis. MRI showed a full thickness rupture of the supra- and partial ruptures of the infraspinatus and subcapsular ligaments. She had no history of shoulder surgeries or trauma. Pain was present at night and aggravated by movement. The patient's VAS score was 6 out of 10 on the NRS-11 scale, and her Oxford Shoulder Score was 24. Intraarticular pulsed mode RF under fluoroscopy was applied with a 10 cm neurotherm needle for 4 minutes to the glenohumeral joint. 3 weeks later, on the patient's control visit, the VAS score was 3 and the Oxford Shoulder Score was 32 (Fig. 1).
Go to : 
CASE 2
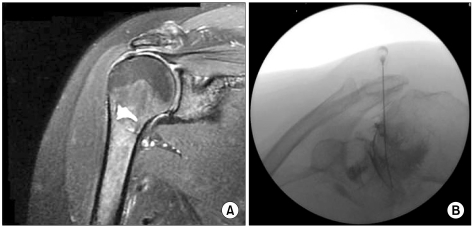
A 76-year-old woman was referred to our pain clinic from orthopedics with the diagnosis of shoulder impingement syndrome with general osteoarthritis and osteoporosis. The patient had no history of trauma or surgery to the shoulder. She suffered from pain throughout the day, aggravated especially at night and by movement, and had severe restrictions on activities of daily living. Despite physical therapy and oral analgesics, her VAS score averaged 7 out of 10 on the NRS-11 scale, and she experienced no improvement in arm movements. Use of her arm was limited in all planes. MRG showed severe degeneration, remodelling and osteophytes in the glenohumeral joint. Oxford Shoulder Score was 16. Intraarticular pulsed mode RF with fluoroscopy was applied with a 10 cm neurotherm needle for 4 minutes to the glenohumeral joint. 3 weeks later, on the patient's control visit, the VAS score was 4 and the Oxford Shoulder Score was 25 (Fig. 2).
Go to :
CASE 3
An 80-year-old woman was referred from orthopedics with the diagnosis of inoperable osteoarthrosis in the shoulder joint. She had no history of trauma or surgery. Her pain was experienced at rest and with movement, and showed little response to oral analgesics. A shoulder X-ray showed severe degeneration and osteoarthrosis in the glenohumeral joint. No rupture was seen in the ligaments around the joint. Her VAS score was 8 out of 10 on the NRS-11 scale. Oxford Shoulder Score was 21. Intraarticular pulsed mode RF under fluoroscopy was applied with a 10 cm neurotherm needle for 4 minutes to the glenohumeral joint. 3 weeks later, on the patient's control visit, her VAS score was 6 and her Oxford Shoulder Score was 21 (Fig. 3).

All 3 patients were seen in clinic for their 2nd control visit in the 8th week following treatment. For all 3, symptoms like pain and range of motion limitation with VAS and OSS scores were the same as before treatment. We conclude that pulsed mode RF can be used as an alternative and palliative treatment with both analgesic and physiotherapeutic procedures, but that it may not be a sufficient therapy itself for chronic shoulder pain patients. More cases are necessary to assess this treatment.
Go to :
 XML Download
XML Download