

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Postherpetic neuralgia (PHN) is defined as pain persisting for more than 1-6 months after the rash has healed [1-3]. Disseminated herpes zoster occurs primarily in immunocompromised patients including patients with chronic kidney disease (CKD) undergoing a regular schedule of hemo-dialysis [4,5].
Doses of anticonvulsants need to be adjusted in these patients according to the glomerular filtration rate and their scheduled dialysis [3,6]. However, it is difficult for them to adjust to the doses of neuropathic medications. If the neural blockade and pulsed radiofrequency ablation provide only short-term amelioration of pain [7], spinal cord stimulation (SCS) with a low level of evidence may be used only as a last resort.
SCS is well known to be effective in some patients with failed back surgery syndrome, peripheral vascular disorders, and complex regional pain syndrome [8-11]. However, it is rare to find the studies with good results in patients with PHN.
The aim of study was to evaluate the efficacy of spinal cord stimulation in the treatment of PHN in patients with chronic kidney disease.
MATERIALS AND METHODS
This retrospective study was done at a pain clinic of Pusan National University Hospital in Korea. The recruitment period was from January 2003 to December 2007. The protocol was approved by the Policy of the Ethical Committee at Pusan National University Hospital Institutional Review Board. The patients eligible were informed about the procedure of the study and agreed to participate in this study and gave their written consent.
The PHN patients with CKD who needed hemo-dialysis who received insufficient relief from pain with a visual analogue scale score of over 8 for at least 6 months regardless of neuropathic medications were eligible for percutaneous SCS test trial. A permanent SCS implant was implanted after patients had experienced at least 50% reduction in the pain score. The follow-up period was at least 2 years after permanent SCS implantation. The successful cases of permanent SCS implantation were defined as the patients who had experienced at least 50% reduction in pain score continuously with tolerable neuropathic medications till the end of study.
The efficacy of the permanent SCS implant was evaluated using the pain score and daily doses of neuropathic medications at the final visit day for the successful cases of the permanent SCS implants. The complications related to SCS were also recorded.
RESULTS
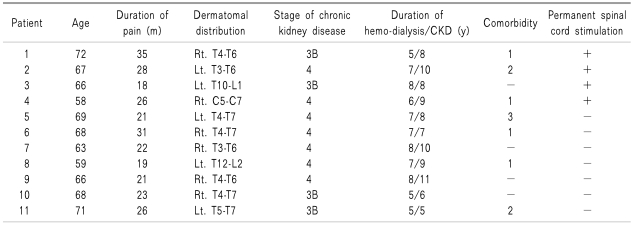
All postherpetic neuralgia pain patients with chronic renal failure who had received trial spinal cord stimulation were male. Mean age was 66.1 ± 4.5 years old. Mean duration of pain was 24.5 ± 5.2 months. Dermatomal distributions of pain were 1 cervical, 8 thoracic, and 2 thoracolumbar areas. Mean duration after diagnosis of chronic renal failure was 8.3 ± 1.8 years. Mean duration of hemo-dialysis was 6.6 ± 1.2 years. Their stages of renal failure were from 3B to 4. Four patients had comorbid diabetes mellitus. All patients had received hemo-dialysis 3 times a week regularly (Table 1).
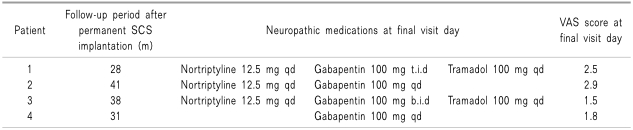
Eleven patients received the SCS test trial during the study period. Four patients had the permanent SCS implanted successfully with their pain being tolerable with a VAS score of less than 3 along with small doses of neuropathic medication at the final visit. Mean follow-up period was 34.5 months (range, 28 to 41 months) (Table 2). There were no complications related to the SCS implant including lead migration, infection, or bleeding.
DISCUSSION
Although it was a small number of PHN patients with CKD, 4 of the 11 patients showed considerable relief of pain and experienced mild pain intensity of less than VAS 3 with tolerable neuropathic medications.
It seemed that factors including age, dermatomal distribution and duration of pain, duration of hemo-dialysis and CKD, stages of CKD, and comorbidity between the success or failure group of permanent SCS did not show any differences in the effectiveness of SCS in this study. Randomized clinical studies showed the efficacy of antiviral agents in the prevention of PHN and the use of anticonvulsants, antidepressants, opioids, and lidocaine patch in the treatment of PHN (level A evidence). The role of epidural local anesthetic and steroid injections in preventing PHN has not been completely established (level B evidence). Intrathecal steroid injections and topical capsaicin may be effective in PHN (level B evidence). A non-randomized controlled study supports the usefulness of spinal cord stimulation [3,12]. SCS is considered to be of poor value in treating PHN because of deafferentation and scarring of the dorsal horn and dorsal root ganglion. A retrospective study for SCS for pain control of 30 peripheral neuropathies revealed that causalgic and diabetic neuropathic pain seem to respond relatively well, whereas postherpetic pain and intercostal neuralgia syndromes seem to respond less favorably to the long-term beneficial effects of SCS [13].
However, Harke et al. [14] insisted that SCS treatment of PHN may offer a worthwhile option in the treatment of pharmacological nonresponders with anatomically intact neural pathways, provided the patients accept such an invasive approach. In cases of unbearable herpes zoster pain, this approach may have supportive benefit as well. Iseki et al. [15] reported that excellent outcomes were achieved with SCS for 7 to 10 days on 2 patients who developed PHN within 2 to 3 months of the onset of the condition. They believed that limited-duration SCS for subacute PHN is a useful treatment approach that may prevent pain from progressing to chronic PHN. The other positive result of SCS in the treatment of PHN was introduced by Meglio et al. in 1989. Although positive in only 6 of the 10 patients, the effectiveness of SCS was remarkably stable over time. They therefore recommend a percutaneous test trial of SCS in every case of PHN resistant to medical treatment [16]. The efficacy of peripheral subcutaneous stimulation for the treatment of intractable PHN was recently introduced [17,18]. However, because the main pathognomonic lesion is known to be the dorsal horn, it is better to believe its role to be in partial control of the origin of the pain. The basic pain mechanism of PHN is known to originate from both the central and peripheral nervous systems. The central mechanism is a disinhibition of the large afferent (Aβ) fibers, central reorganization, and central sensitization. The peripheral mechanism is ectopic discharge, increased sympathetic activity and catecholamines on the sensitized and damaged primary afferents, and continuous inflammatory response of the sensory nerve or nervi nervorum [19].
The great limitation of this study was the small number of patients. A well-designed comparative prospective multi-center studies are needed. The other limitation is the control ability of the SCS instrument because of old age. Only the patients know characteristics and intensity of the pain; however, they will not or cannot manipulate the mode of the SCS. It is difficult to use the SCS even with the best mode of control. Therefore, SCS in the elderly may be underestimated. It is also difficult to perform SCS trial test for pain in the subacute stage of PHN due to insurance coverage.
SCS was helpful in managing with tolerable pain levels in some PHN patients with CKD along with tolerable neuropathic medications for over 2 years.
 XML Download
XML Download