

 PDF
PDF Citation
Citation Print
Print


Chronic pancreatic pain can be caused not only by malignancy, but also benign disease. Regardless of the cause, pancreatic pain is often difficult to manage even with strong analgesics and can be debilitating to many patients. Despite it being an invasive procedure, neurolytic celiac plexus block (NCPB) is reported to be an effective treatment option with a low complication rate for patients with non-malignant abdominal pain that is not controlled with analgesics [1-4].
Common complications of NCPB are hypotension, diarrhea and local pain at the injection site [5]. Among the uncommon complications, ejaculatory failure has been reported very rarely [6,7], and its significance is often overlooked due to short life expectancies in terminal cancer patients. We report a case of ejaculatory failure in a patient who received unilateral NCPB for the treatment of pain due to chronic pancreatitis.
CASE REPORT
A 45-year-old male patient was referred to our pain clinic during admission for abdominal pain control due to chronic pancreatitis. He had been diagnosed with diabetes mellitus type 2, liver cirrhosis and hepatocellular carcinoma due to chronic alcoholism 5 years ago and was being followed up without any viable tumor recurrence after having received transcatheter arterial chemoembolization. His daily medications were 2 mg of glimepiride for diabetes, 10 mg of zolpidem tartrate and 75 mg of trazodone for depression and anxiety, and 10 mg of alfuzosin for benign prostatic hyperplasia. He had made frequent visits to the emergency room complaining of severe abdominal pain, and was admitted to the department of internal medicine for pain control and conservative management.
The patient's chief complaint was continuous epigastric pain and severe postprandial pain of 7/10 on a visual analogue scale (VAS) score of 0 to 10, which was dominant on the left side. The pain itself was well controlled at a VAS of 2/10 with opioid analgesics, but the patient experienced severe constipation and sedation and requested a nerve block in an attempt to reduce his pain medication. He was taking 40 mg of oxycodone four times a day and 8 mg of hydromorphone daily. The patient's most recent abdomino-pelvic CT showed no evidence of tumor recurrence, and atrophic change of the pancreas. Otherwise, there were no anatomical distortions within the patient's abdominal cavity.
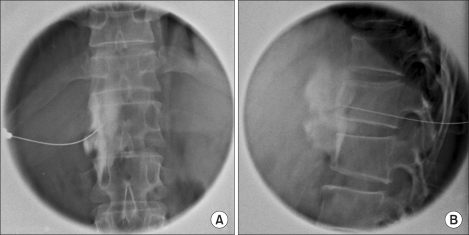
After obtaining a written consent form from the patient, we performed an elective left sided unilateral celiac plexus block under fluoroscopy guidance with the patient in the right lateral decubitus position. The patient's pain was clearly dominant on the left side, and because the source of his pain was a benign disease, a unilateral block was chosen in an attempt to reduce any possible complications. A skin wheal was raised with 1% lidocaine at a point 7 cm lateral to the L1 spinous process which corresponded to the inferior edge of the 12th rib, and a 15-cm 22-gauge needle was introduced at a 45 degree angle until it made bony contact with the L1 vertebral body. The needle's angle was adjusted as it was advanced by sliding off the anterolateral side of the vertebral body until it reached the anterior margin of the L1 vertebral body in the lateral view. A 10 ml plastic syringe filled with saline was then attached to the needle hub, and the needle was advanced slowly until loss of resistance was felt and pulsations of the aortic wall could be identified along the shaft of the needle. After the needle was aspirated and found to be negative for blood, a diagnostic block was done with 5 ml of 2% lidocaine mixed in 5 ml of iohexol (Omnipaque™, GE Healthcare Ireland, Carrigtohill, County Cork, Ireland) and adequate spread of dye was confirmed in the anterior-posterior and lateral view radiographs (Fig. 1). The patient was examined for any sensory or motor deficits for 20 minutes, and fluoroscopic evaluation was done to check for any delayed dye spread in unwanted regions such as across the midline of the vertebral bodies in the anterior view and posterior spread or along the psoas muscles in the lateral view. We checked for any numbness or dysesthesia in the T10-L2 dermatomes and weakness in quadriceps function as well as the patient's ability to wiggle his toes. When the patient's abdominal pain had resolved and no other side effects were observed, NCPB was done with 8 ml of 99% anhydrous alcohol (Dehydrated Alcohol Injection, Daihan, Ansan, Gyeonggido, Korea). The patient was followed up for 1 week until discharge from the hospital, and showed no motor or sensory deficits, hypotension or diarrhea. His pain medication was reduced to half of the pre-procedure dose, and the patient's pain was well controlled at a VAS score of 2/10. When the patient came to our out-patient clinic 1 month after discharge, his pain was still well controlled with reduced oral analgesics, but he reported that he had been unable to ejaculate since the procedure. He described his symptom as "a faucet turned off tight", and that he could not ejaculate during climax, which was a symptom that he had not experienced before the NCPB. We referred him to the department of urology and he is being followed-up under the impression of retrograde ejaculation but without any further evaluation. As of now, his ejaculation has not returned during the 3 months period after the procedure.
Go to : 
DISCUSSION
NCPB is a commonly performed procedure in patients with intractable pain due to malignancies involving the upper and mid abdomen [5]. Although its role in patients with benign abdominal pain has not been well established with controversies on whether it is truly effective for pain due to chronic pancreatitis, it is still recommended for patients who have exhausted all other treatment modalities [2].
One of the rare, but usually ignored complications of NCPB is sexual dysfunction [8]. Reports of ejaculatory failure after celiac plexus block are very rare. One case was reported by Leung et al. [6] in a study of 23 patients with chronic pancreatitis and 13 patients with pancreatic cancer. The patient had developed impotence and hyperesthesia of the lower limbs after a second block. Black and Dwyer [7] reported two cases of ejaculatory failure in a series of 100 patients who underwent celiac plexus block, and stated that it was a rare complaint due to the fact that most of the male patients selected were elderly. Whether the complication was resolved over time was not mentioned in either study.
The normal ejaculation process is composed of three phases: seminal emission, bladder neck closure and ejaculation [9]. These three phases are under sympathetic α-adrenergic control of neurons, the cell bodies of which are located in the lateral columns of T11-L2, and parasympathetic fibers of S2-4 [10]. The thoraco-lumbar spinal tract (T11-L2) appears to be responsible for the contraction of smooth muscles of the prostate, seminal vesicle, the vas deferens, and partial bladder neck closure [11]. If sympathetic tone is completely abolished, no seminal emission will occur; if sympathetic tone is partially disrupted, it will lead to retrograde ejaculation.
It is well known that there is a true risk of retrograde ejaculation after bilateral lumbar sympathetic blocks in male patients. Bilateral surgical sympathectomy is followed by disturbance of ejaculation in 13-54% of cases [12] but case reports are very rare with unilateral surgical lumbar sympathectomy or bilateral chemical sympathectomy. Baxter and O'Kafo [13] reported a case of ejaculatory failure following bilateral phenol sympathectomy performed at L2-4, which eventually resolved after 5 weeks. Ishizaki et al. [12] reported two cases of ejaculatory failure after chemical sympathectomy; a case of absent seminal emission after bilateral chemical sympathectomy of L2 and L3, and another case of retrograde ejaculation after unilateral chemical sympathectomy of L3. The former case did not resolve after 3 years of follow-up. However, the latter case was spontaneously changed to antegrade ejaculation after 2 years and 7 months.
The patient of this case underwent a unilateral NCPB with 8 ml of 99% anhydrous ethyl alcohol. A unilateral NCPB was performed in this patient for two reasons. First, the patient's pain was dominant on the left side, and second, unilateral NCPB may have benefit in reducing the complications of neurolysis in a patient with benign abdominal pain [14]. Despite this precaution, ejaculatory failure occurred in this patient and has not resolved after 3 months. Although he is being followed-up by an urologist, whether this patient's symptom is loss of seminal emission or retrograde ejaculation has not been determined. A post-masturbation urine specimen should be examined for sperm in order to accurately diagnose the type of disorder this patient is experiencing.
Ejaculatory failure after NCPB may be attributed to spread of neurolytic agents to an unwanted region. In the case reported by Leung et al. [6], the authors used 25 ml of alcohol on each side for a bilateral NCPB in a patient with chronic pancreatitis. However, only 8 ml of alcohol was used for unilateral NCPB in our case. Other explanations may be variations in the dimension of the paravertebral space leading to varying amount of neurolytic agent spread or abnormal sympathetic chain anatomy of the patient.
Diminished or retrograde ejaculation, as well as anejaculation may occur in up to a third of male patients with diabetes [15]. In our case, the patient had been diagnosed with DM type 2 and was on medication for 5 years with random blood glucose levels ranging from 120 to 240 mg/dl. The patient was also taking zolpidem tartrate and trazodone due to depression and anxiety and alfuzosin due to benign prostatic hyperplasia, but these medications are not known to cause ejaculatory disorders. Although the history of DM with poorly controlled blood glucose levels may be a contributing factor to the patient's ejaculatory disorder, the fact that the symptoms developed dramatically after NCPB heightens the probability of it being a complication of the procedure.
For patients with short life expectancy and low quality of life regardless of adequate pain control, sexual dysfunction may not have been an issue. On the other hand, for patients with non-malignant diseases in which pain is the main problem, quality of life may be significantly improved once their pain is well-controlled thus magnifying the presence of complications such as sexual dysfunction. In these patients, complication such as ejaculatory failure should be considered more important than in terminal cancer patients, and deserves more attention. Therefore, whenever a NCPB is considered for a sexually active male patient with a long life expectancy, the risk of ejaculatory failure should be considered seriously.
Go to :
 XML Download
XML Download