

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Early cancer diagnosis and various therapeutic options have extended the life expectancy of cancer patients. Unfortunately, however pain management for patients with malignant disease has not been effective, which decreased the quality of life of cancer patients. Approximately, 20-50% of all cancer patients suffer pain and 75-90% of terminal cancer patients experience severe pain [1]. The most difficult type of cancer pain is bone cancer pain, which occurs primarily in bone or secondarily by metastasis from distant organs to bones [2-4]. The characteristics of bone cancer pain are constant, increased with time and exacerbated after movement or weight-bearing on the affected limb [5-7]. The most commonly used analgesics for cancer pain control are non-steroidal anti-inflammatory drugs (NSAIDs) and opiates [8]. However, despite the widespread use of both drugs, their analgesic effect is often limited and they sometimes cause side effects [9,10]. Therefore, the effective and safe analgesics for cancer pain management are needed.
The root of Pannax ginseng C.A. Meyer, or ginseng, has been used as an herbal medicine [11]. Therefore, it has been used for a long time to relieve some types of pain such as toothaches, abdominal pain and neuralgia in traditional folk medicine. The major active constituents of ginseng are ginsenosides [12]. It has been reported that ginsenosides inhibited postoperative pain and inflammatory pain at the spinal level of rats [13-15]. Therefore, we hypothesized that spinal ginsenosides may reduce cancer pain.
The aim of this study was to evaluate the efficacy of an intrathecal ginsenosides in a murine bone cancer pain model.
Go to : 
MATERIALS AND METHODS
All procedures were performed following the approval by the Institutional Animal Care and Use Committee of Chonnam National University. The experiments were done on adult male C3H/HeJ mice, weighing 20-25 g. These strains were selected for their histocompatibility with the NCTC 2472 tumor line [American Type Culture Collection (ATCC), Rockville, MD, USA]. The mice were housed in a vivarium, maintained at 22 ± 0.5℃ with a 12-h light/dark cycle and were allowed to access food and water.
Tumor cells were incubated and cultured in NCTC 135 medium (Sigma-Aldrich Co., St. Louis, MO, USA) with 10% horse serum (ATCC) at 37℃ in a 5% CO2 in air atmosphere, and passed two to three times weekly. Tumor cells inoculated into the femur of the mice under intraperitoneal ketamine (100 mg/kg) anesthesia according to a previously described method [16]. When the mice did not respond to a paw pinch, the right thigh of the mice was shaved and disinfected with povidone-iodine. A 1 cm skin incision was made along the lateral femur and a 25 gauge needle was inserted into the medullary cavity of the distal femur. Tumor cells were injected using a hand-driven, gear-operated injector connected to the 25-gauge needle with polyethylene-10 tube. Twenty µl of minimal essential medium (MEM) alone (sham; n = 3) or MEM containing 2.5 × 105 tumor cells (n = 6) were injected slowly. The injection site was sealed with dental amalgam, and the skin was closed with 6-0 silk sutures. Radiographics and the determination of the withdrawal threshold in tumor cells-injected femur were done at 7, 14, 21 days after tumor cells inoculation to assess the bone tumor and bone cancer pain development.
Ginsenosides were used in this study and provided by the Korea Ginseng and Tobacco Research Institute (Daejon, Korea) and dissolved in dimethylsulfoxide (DMSO). Ginsenosides were intrathecally administered according to the procedure of Hylden and Wilcox [17] using a 25 µl Hamilton syringe with a 30-gauge needle. The needle was inserted between L5 and L6 and the injection volume was 5 µl. The intrathecal placement of a needle was confirmed by observation of a tail flick of the mice.
The development of bone cancer pain was evaluated by measuring the mechanical sensitivity of the tumor cells-injected femur. The withdrawal threshold in response to mechanical stimulation was measured with von Frey filaments (Stoelting, Wood Dale, IL, USA). One of von Frey filaments (0.4-3.6 g) was applied to the tumor cells-injected femur for 4 s while the filament was bent. Sharp withdrawal or flinching of paw was regarded as a positive response. If no response was noted at a pressure of 3.6 g, mice were assigned to this cutoff value. The 50% paw withdrawal threshold was determined according to a previous method of Dixon [18].
Fourteen days after tumor cells inoculation, the behavioral study was commenced. The mice were placed individually in plastic cages with a plastic mesh floor (4 × 5 × 5 cm) and allowed to adapt for 20-30 min before the experiments. Intrathecal ginsenosides (150, 500, 1,000 µg, n = 19) were administered and the withdrawal threshold was measured at 15, 30, 60, 90, and 120 min after delivery of ginsenosides. Intrathecal DMSO was used as a control (n = 3). The withdrawal threshold measured before tumor cells injection was regarded as the baseline threshold. Each mouse was tested only once. The investigator was blind to the experimental conditions in all cases.
To examine the abnormal behaviors of ginsenosides, additional naive rats (n = 5) were given intrathecal ginsenosides (1,000 µg), and examined at 15, 30, 60, 90, and 120 min after administration. The righting and placing-stepping reflexes were checked for evaluation of motor function. The first was tested by placing the mice prone on the table, which normal mice immediately take a posture to an upright position. The latter was tested by placing the dorsum of hind paw across the edge of the table, which normal mice put their paws forward into a position for walking. Next, pinna and corneal reflexes were evaluated with a paper string [19]. The first was tested by stimulation of the ear canal, which normal mice spontaneously shake their heads. The latter was tested by stimulation of the cornea, which normal mice spontaneously blink. All of four reflexes were judged as present or absent.
The data are expressed as mean ± SEM. The time-response data are presented as the withdrawal threshold in g. The dose-response data are presented as percentage of maximal possible effect (%MPE) according to the formula.

The dose-response data were analyzed using one-way analysis of variance (ANOVA). Differences in the withdrawal threshold between the sham and tumor mice were analyzed using unpaired t-tests. Results were statistically significant in case of P < 0.05.
Go to :
RESULTS
NCTC 2472 tumor cells inoculation into the intramedullary cavity of distal femur of mice radiographically induced bone destruction over time (Fig. 1). However, the bone tumor was not noted in MEM-injected femur (sham) until 21 days after injection. The inoculation of tumor cells into the femur resulted in a decrease of the withdrawal threshold in injected site (Fig. 2). By contrast, no change of the withdrawal threshold was noted in mice with sham injection.
 | Fig. 1Radiographics of sham-injected (A) and NCTC 2472 tumor cells-injected mice. Tumor cells were inoculated into the femur and radiological examination was done at 14 (B) and 21 (C) days after tumor cells injection. Tumor cells injections induced bone tumor and osteolysis over time. No change was seen in sham group. Arrows head indicated the bone destruction.
|
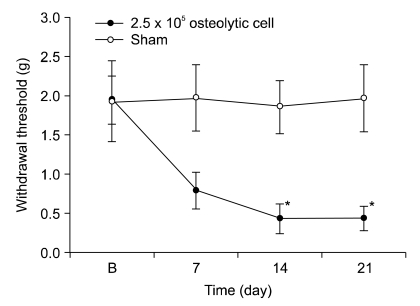 | Fig. 2Time course of the withdrawal response to von Frey filaments after tumor cells injection. Each line represents mean ± SEM of 4-6 mice. B = baseline withdrawal threshold measured before tumor cells injection. Paw withdrawal threshold (g) was plotted versus time in days. A significant difference was noted between the tumor and sham groups. *P < 0.05.
|
Intrathecal administration of ginsenosides dose-dependently increased the withdrawal threshold in mice with tumor cells inoculation (Fig. 3). At 150 µg, intrathecal ginsenosides did not affect the withdrawal threshold. At 500 µg, ginsenosides increased the withdrawal threshold, however, the effect was progressively declined. At 1,000 µg, the effect was maintained during the entire observation period.
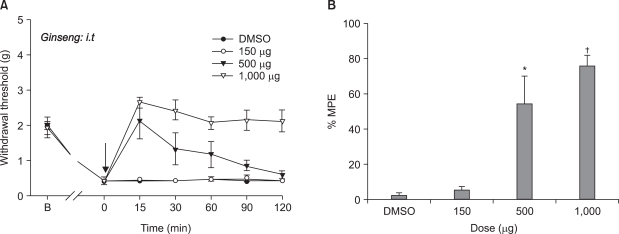 | Fig. 3Effects of intrathecal ginsenosides on the withdrawal response to von Frey filaments after tumor cells injection. The data are presented as the withdrawal threshold (A) or percent of the maximum possible effect (%MPE, B). Each line or bar represents mean ± SEM of 5-6 mice. B = baseline withdrawal threshold measured before tumor cells injection. DMSO = dimethylsulfoxide. The withdrawal threshold was measured immediately before ginsenosides delivery, and intrathecal ginsenosides were administered at time 0 (arrow). The withdrawal threshold was dose-dependently increased with ginsenosides. *P < 0.05, †P < 0.01.
|
After the intrathecal delivery of ginsenosides, the righting, placing-stepping, the pinna and corneal reflexes were present.
Go to :
DISCUSSION
In the present study, we evaluated the analgesic effect of ginsenosides in bone cancer pain model. The injection of NCTC 2472 tumor cells into the femur resulted in an osteolysis and decreased the withdrawal threshold in tumor cells-injected site. These observations indicated that the intrafemoral injection of NCTC 2472 tumor cells may properly induce bone tumor and bone cancer pain model as reported previously [16].
To date, NSAIDs and opiates have been considered as typical analgesics for bone cancer pain [8]. However, despite a variety of pharmacotherapies for bone cancer pain, the effect is relatively poor. Such difficulty of treatment is caused by a lack of knowledge of the basic neurobiology of bone cancer pain. But, the use of the mouse bone cancer model used in this study may expedite the understanding of the pathophysiology of bone cancer pain and advance the development of novel analgesics for treating bone cancer pain.
In this study, intrathecal ginsenosides produced a dose-dependent increase of the withdrawal threshold in the bone cancer site. Furthermore, the antinociceptive effect was persistent during the observation period at the highest dose. These findings suggest that ginsenosides are active against bone tumor pain at the spinal level. Ginseng has long been used in Eastern Medicine medicine to improve the weakened physical status brought on by stress or disease [11]. Ginsenosides, ginseng saponins, are the major components responsible for the effects of ginseng [20]. Previous experiments also suggest that ginsenosides are effective to a variety of nociceptive conditions. Intrathecal ginsenosides inhibit formalin-induced, substance P-induced and paw incision-induced pain behaviors in animals [13-15]. These observations, thus suggest that ginseng may afford an antinociceptive action in the spinal cord.
In spite of the wide use of ginsenosides in a various medical fields, the mechanism of action remains to be determined. Chemically, ginsenosides have a four-ring, steroid-like structure with sugar moieties attached and show properties similar to acetylcholine, adrenaline, and histamine [21], which suggests that these chemicals may be involved in the action mechanism of ginsenosides. Furthermore, recently it has been reported that opioid receptors may play an important role in the antinociceptive mechanism of action of ginsenosides at the spinal level [14]. Previous studies have also shown that the nicotinic acetylcholine receptor may contribute to the mechanism of action of ginsenosides [15,22]. Moreover, several lines of evidence suggest that Ca2+ channels play an important role in the pharmacological activity of ginsenosides [23-25]. On the other hand, it has been reported that alpha2, muscarinic, and GABA receptors are not the pharmacological sites of action of ginsenosides [23,26].
There were some limitations in this study. First, the authors only evaluated the effect of ginsenosides. More researches with different types of chemicals may be needed for the determination of the mechanism of action of ginsenosides. Second, the authors just used the behavioral study. Molecular works may help to examine the action mechanism of ginsenosides.
Spinal ginsenosides are not yet available clinically. However, ginsenosides may be used effectively in the management of bone cancer pain in the future. Thus, this is the first report which proposed the possibility for clinical use of ginsenosides.
Taken together, injection of NCTC 2472 tumor cells into the femur of mice caused bone tumor and pain. Intrathecal ginsenosides dose-dependently attenuated the bone cancer pain. Therefore, spinal ginsenosides may be useful for managing bone cancer pain.
Go to :
 XML Download
XML Download