

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
In the diagnostic radiology of nervous system disease, magnetic resonance imaging (MRI) is currently used as the standard test because it shows much better contrast in the soft tissue than computed tomography (CT) and can provide any kind of cross-sectional images, including the coronal image and sagittal image, as well as the axial image. The MRIs are obtained at once in 5 to 10 minutes of duration, while the CT cross-sectional images are taken 1 for each time. Thus, severe motion artifacts are found not only in 1 or 2 cross-sectional images, but also in all the images if the patient moves a lot during the 5 to 10 minutes of duration. In the cases where the patient is unable to remain in a certain position due to severe pain, the MRI is taken after epidural injections to obtain fine results. There are various methods of verifying the epidural space for the epidural injections, but the loss-of-resistance technique is the most frequently used method at present. This technique is to verify the epidural space by the loss of resistance that takes place when the needle punctures the yellow ligament and air or saline solution is employed. Although there are several advantages of using air, some complications such as incomplete nerve block, nerve root compression, subcutaneous emphysema, and pneumocephalus have been reported [1]. We report a case of the epidural block based on the loss-of-resistance technique for the MRI of a patient with severe pain where the injected air could be misidentified as a cervical herniated disc by the MRI, and we review the related literature.
Go to : 
CASE REPORT
A fifty-year-old, female patient underwent a severe pain at the cervical part and the left upper extremity from 1 day before her visit to the hospital and MRI was carried out. However, since the patient continuously moved due to the severe pain, the imaging was stopped after only the image of a part of the sagittal plane was taken. It was decided that the MRI should be carried out after pain control, and the patient was sent to the department of pain medicine. By the visual analogue scale, the pain was evaluated to be level 3 at the neck and level 9-10, which was very severe, at the left upper extremity. The Spurling sign was positive (+) and mild muscular weakness was found. It was decided to perform an epidural nerve block in order to control the pain. Under the C-arm guidance, the epidural nerve block was tried in the sitting position. The epidural space was found by the loss-of-resistance technique with air and 0.5 ml of a contrast material was injected to confirm the epidural space. Then, 2.5 ml of the contrast material was injected additionally and its diffusion to the C2-C3 position was verified. After that, 0.75% lidocaine 3 ml was injected and the epidural nerve block was carried out. For 1 hour following the nerve block, EKG, SpO2, blood pressure, and consciousness of the patient were monitored. The MRI was resumed since the pain was reduced to the degree where the patient was able to take the supine position for more than 10 minutes. In the T2 image of the sagittal plane that was taken for the second time, the C3-C4 and C5-C6 herniated disc were suspected (Fig. 1). However, the C3-C4 lesion which was suspected as the herniated disc was considered to be an air shadow in the CT cross-sectional image that was taken for the operation (Fig. 2A). The T2 image of the sagittal plane that was partially taken before the nerve block was compared in order to identify the lesion, and the result showed that it was a new shadow that had not existed before the nerve block procedure (Fig. 2B). Nerve root compression was found at the left C6 in the electromyogram that had been performed in advance, but no C3-C4 herniated disc was found before the nerve block. The shadow looked as if it was by air in the CT image and the shadow in the C3-C4 intervertebral space (Fig. 2C, D) was different from the shadow of the C5-C6 herniated disc in the T1 and T2 cross-sectional images (Fig. 2E, F). Therefore, we concluded that the shadow was an artifact by air and decided to carry out only the operation for the C5-C6 herniated disc. The patient underwent a C5-C6 anterior cervical discectomy and fusion (ACDF) during the next day and received an MRI 2 days after the operation. No air shadow was found in the C3-C4 intervertebral space in the postoperative MRI (Fig. 3). The pain of the patient was greatly reduced so that the visual analogue scale could be 0 to 1 on the 8th day after the operation and thus the patient was discharged.
 | Fig. 1T2 sagittal image after cervical epidural block shows low signal intensity lesion at C3-C4 and C5-C6. These lesion are considered herniated disc.
|
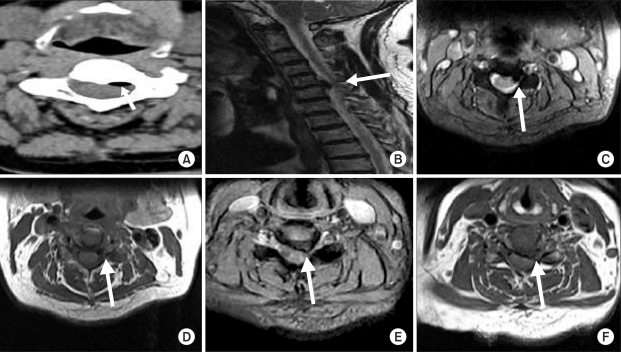 | Fig. 2CT axial image (A) shows low density lesion behind C3-C4 disc. At CT, it seems like the air, not herniated disc. Low signal intensity lesion behind C3-C4 disc seems new compared MRIs before and after cervical epidural block. There is no lesion behind C3-C4 disc in MRI before cervical epidural block (B). (C) and (D) show air as a low signal intensity. By contrast, (E) and (F) show C5-C6 herniated disc relatively higher intensity than lesion behind C3-C4.
|

Go to :
DISCUSSION
The epidural block is a commonly used technique applied to the patient who complains of pain at the neck, lumbar spine and lower extremity. The epidural block has been greatly developed by the advancement of various instruments and drugs. However, finding the epidural space appropriately is the key factor that determines a successful epidural block. Hanging drop technique and loss-of-resistance technique are the methods to find the epidural space, but the latter is preferred in general. Air or saline solution is employed in the loss-of-resistance technique. When saline solution is used, the loss of resistance is definitely felt because it is not compressed, but it has such disadvantages as it may not be distinguishable with cerebrospinal fluid (CSF) when a dural puncture is performed unintentionally, and the drugs may be diluted with it. Use of air is advantageous because it is simple and convenient, but it may cause complications such as air embolism, subcutaneous emphysema, pneumocephalus, or incomplete nerve block [2]. However, the importance of the loss-of-resistance technique using air should never be underestimated since it is a successful method that is frequently used worldwide. Dalens et al. [3] reported the cases of 2 patients who underwent incomplete nerve blocks after the epidural nerve block with the loss-of-resistance technique using air, and air bubbles were found in the part close to the nerve root of the spine which was corresponding to the dermatomes of which the nerve was not blocked according to the radiation test. Boezaart and Levendig [4] also reported the case where the nerve was not blocked by the epidural air bubbles, and they stated that an incomplete nerve block may take place at the corresponding dermatome as th access of the drugs approaching the nerve root is interrupted. Abbott et al. [5] commented that it would be better to employ saline solution than air for the loss-of-resistance technique, since the air may cause damage to the spinal cord or the nerve as it spreads along the nerve that extends around the spine.
Kennedy et al. [6] reported that case where low back pain and paraplegia took place as air was mistakenly injected into the epidural space while an epidural injection of opioids was continuously carried out for the treatment of cancer pain. The CT imaging result showed that the epidural space in between L1-L4 was filled with air and the injected air was so much especially in between L2-L3 that the thecal sac was severely compressed. The low back pain and paraplegic pain disappeared after about 15 ml of air was removed by inserting a needle into the epidural space. Hirsch et al. [7], Miguel et al. [8], and Petty et al. [9] also reported the cases where motor weakness, sensory loss, and paraplegia were found after the epidural nerve block, and the spinal cord was compressed by the air around the spinal part corresponding to the neurological deficit according to the CT image. Stevens et al. [10] radiologically observed the spread of air after injecting air to the epidural space of dogs. The air bubble injected to the epidural space was easily verified by means of epiduroscopy. They reported that the air bubbles were concentrated at the part near to the outlet of the nerve root coming out of the epidural space. The air bubbles were observed for 24 hours in all the dogs used for the experiment, but all of the air bubbles disappeared after 96 hours. Cuerden et al. [11] reported the cases of 4 patients in the obstetric department whose recovery was delayed because of neurological symptoms, such as sensory loss, motor weakness, and dystonia, after the epidural anesthesia. Since all the patients were recovered within 48 hours, the authors assumed that the symptoms of the patients might disappear, as the air was all absorbed within 24 to 48 hours, if the neurological symptoms were caused by the compression of the spinal nerve by the pooling air inside the epidural space.
In this case, a cervical epidural nerve block was performed in order to attempt resumption of the MRI imaging on a patient for whom MRI imaging was difficult due to severe cervical pain. When the loss-of-resistance technique using air was applied for the cervical epidural nerve block, the air pooling in the epidural space was misidentified as a herniated disc. In some cases, neurological symptoms are found when the air pools in the epidural space of the patients. Stevens et al. [10] reported from an experiment that the air bubbles were collected at the part near to the outlet of the nerve root coming out of the epidural space. Hence, an injection of a large amount of air can cause radiculopathy and even a small amount of air used for the epidural nerve block can be misidentified as a herniated disc on the MRIs. The methods to differentiate a herniated disc and air bubbles are: 1) to determine the correlation between the symptoms and the MRI lesion; 2) to refer to the CT image; and 3) to discern the difference between the signals by the air bubbles and the herniated disc. Since a suspected lesion was identified as air shadow in the CT image that was performed for the operation, an operation over the unnecessary range based on a wrong diagnosis could be avoided. The air was found to be all absorbed according to the MRI taken after the operation. As in this case report, it should be remembered that the air injected during the loss-of-resistance technique procedure can be misidentified as a herniated disc in the MRI taken after the epidural nerve block. It is necessary to analyze the differences of the lesion signals in the T1 and T2 images or verify with the CT image if the symptom is irrelevant or an unexpected shadow is found. The nerve block procedure should be carefully carried out since a large amount of air injected to the epidural space can cause radiculopathy or can be misidentified as a herniated disc. It would also be fine to use saline solution instead of air for the procedure.
Go to :
 XML Download
XML Download