

 PDF
PDF Citation
Citation Print
Print


Piriformis syndrome, the neuropathy caused by compression or entrapment of sciatic nerve due to pathologic condition and anatomical variation of piriformis muscle, is difficult to differentially diagnose from discitis, lumbosacral plexopathy, sacroiliitis, sciatica, and greater trochanteric bursitis [1]. It has been reported that about 6% of chronic back pain patients has such piriformis syndrome [2]. Though muscle and nerve tissue have resistance against radiotherapy, peripheral neuropathy including damage on muscle tissue can occur in low probability [3]. Here we report a case where peripheral neuropathy is caused by damage on muscle tissue after radiotherapy for a cervical cancer patient.
CASE REPORT
A 50-year old female patient visited the hospital, referred from the obstetrics and gynecology department, with the chief complaints of pain at the right hip and leg which had continued from five to six months ago. The strength of the pain was around 6/10 by visual analogue scale (VAS). The pattern of the pain was an ache spreading from the right part of the anus to the right thigh and the rear side of the calf. She felt the pain in all types of positions, but it was even more serious when she sat or walked for a long time. Physical examination, including the sensory and motor neurologic test, deep tendon reflex test, straight leg raise test, and flexion, adduction and internal rotation (FAIR) test, revealed no specific findings except tenderness at the right piriformis muscle and greater sciatic notch. The patient had previously had a total hysterectomy, due to cervical intraepithelial carcinoma 18 years before, as well as a few treatments of radiotherapy and chemotherapy for local recurrence and metastasis. Magnetic resonance imaging (MRI), performed at the time of the visit, showed no specific findings except a minimal diffuse bulging disc at the L3-4 and L4-5. There was no specific finding from the electromyography. There were no findings either by the pelvis MRI or the PET-CT, which may cause lumbosacral plexopathy or sciatic neuropathy by local recurrence and metastatic lesion. No inflammatory finding was revealed in the blood test. Although trigger point injection, epidural steroid injection, lumbar sympathetic ganglion blockade, and sacroiliac joint injection were performed to treat the pain, they only resulted in temporary pain relief with no continued improvement. In spite of oral administration of narcotic analgesics, the pain became even more severe. Seven to eight months later, the patient reported decreased leg strength and severe (VAS 7-8/10 score) pain at the buttock and thigh. The decrease in leg strength was limited to under the knee, and the dorsiflexion of the ankle and the plantar flexion was lowered to 3/5 grade, but no muscular atrophy was observed. Though the lumbar spine MRI at that time showed no significant change in spinal lesion, fatty atrophy was found at the right piriformis muscle. In addition, the electromyography showed right sciatic neuropathy. Suspecting the nerve entrapment syndrome by fatty muscle atrophy, local anesthetic and steroid were injected to the piriformis muscle under the fluoroscopic guide (Fig. 1). After the injection, the pain was maintained at the level of VAS 1-2/10 for a few months, but the reduced leg muscle strength was not recovered. After that, no additional treatment was performed because the patient rejected further treatment.

Go to : 
DISCUSSION
Piriformis syndrome is the uncertain disease entity that pathologic conditions of the piriformis muscle cause pain at the buttocks and legs. The major symptom is pain in the buttock while in the sitting position or pain that is worsened by movement of the legs, sometimes accompanying pain in the legs. The typical findings include tenderness on the buttocks from the sacrum to greater trochanter without the symptoms at the lower back or hip joint, piriformis muscle tenderness according to pelvic or rectal examination, or pain which is aggravated by FAIR positions. Discrepancy in leg length, weakened pelvis abductor muscles, and pain due to pelvis muscles abduction against resistance in the sitting position can be the findings as well [1]. It has been known that pressure on the sciatic nerve by piriformis muscles causes such symptoms. Usually, piriformis syndrome is clinically diagnosed by the symptoms and physical examination, and a definite research result has not been reported yet. Recently, it has been possible to evaluate anatomical variation in the sciatic nerve and piriformis muscles and the sciatic nerve entrapment of piriformis and adjacent tissue by means of magnetic resonance neurography and an interventional MRI so that a more precise diagnosis and treatment can be possible [4,5]. Through electromyography, normal findings are usually shown at the initial stage, but abnormal spontaneous activity can be observed as the pressure on the sciatic nerve continues. On the other hand, it has been known that normal findings in the paraspinal muscles of the lumbosacral spine can be helpful for differentiating radiculoparhy, and peroneal division of sciatic nerve is more susceptible to compression or entrapment [6]. In this case study, the electromyographic findings of paraspinal muscles were normal, which fit with the diagnosis of piriformis syndrome, but the neuropathic finding in the tibial division among the sciatic nerves was different from the common piriformis syndrome.
It is known that radiotherapy may cause damage to the nerves. The brachial plexopathy after radiotherapy on the axillary glands for a breast cancer patient was firstly reported. Post-radiation complications of intrapelvic tumor including cervical cancer usually occur at the bladder, intestinal tract, and ureter, but neuropathy is known to be very rare. However, lumbosacral plexopathy has been reported in the case where the radiotherapy of more than 70 cGy was performed on the pelvis, and plexopathy usually has bilateral symptoms or signs of a weakened muscle at the proximal part [3,7]. The case where sciatic neuritis occurred after the radiotherapy on metastasis of liver cancer to ilium and the pain relieved by sciatic nerve blockade has been also reported [8]. Post-radiation damage on muscles is rarely found, but muscular dystrophy, edema, fibrosis, and contracture can occur with increased probability of complications when chemotherapy is conducted in parallel. The patient in this case report was given radiotherapy for ten years over the dose of 80 cGy, including external beam radiotherapy and concurrent chemo-radiotherapy with brachytherapy and cisplatin. It has been reported that the damage on muscles occurs over several years and the probability of occurrence is increased as the total dose is larger or as the radiation dose per one time is larger even with the same total dose [3,9].
We have found the right sciatic neuropathy by electromyography and the fatty atrophy at the right piriformis muscle by conducting a lumbar spine MRI. The status of the piriformis muscle was reviewed based on the pelvic MRI, which had been performed on the patient to check the recurrence and metastasis of a tumor from the past. As a result, asymmetric piriformis muscle atrophy was also found in the pelvic MRI performed one year before the visit (Fig. 2A), and serious fatty atrophy and edema in the piriformis muscle were observed from the pelvis MRI that had been performed after the disease had progressed and decreased muscle strength was found (Fig. 2B).
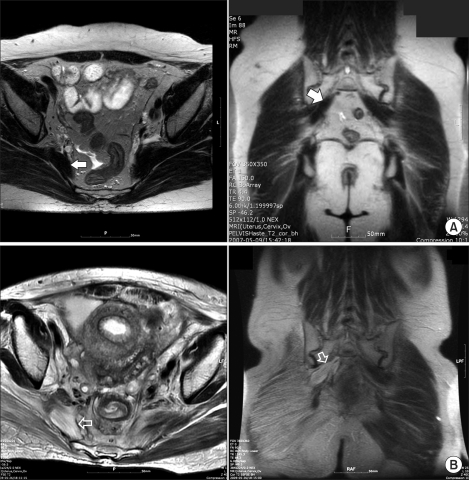 | Fig. 2Magnetic resonance imaging of the pelvis. (A) Axial and coronal T2-weighted MR images show mild atrophy of the right piriformis muscle (white arrow). (B) Two years later, axial and coronal T2-weighted MR images demonstrate marked atrophy of the right piriformis muscle (open arrow), producing a ghost-like appearance.
|
Based on the abnormal findings from the MRI, a local anesthetic and steroid were injected into the piriformis muscle so that the pain could be considerably reduced, but the patient's pain relapsed after several months. For a more definite diagnosis and treatment, surgical treatment was recommended, but it was not conducted because of the patient's refusal.
Thickening of the piriformis muscle is usually found in the piriformis syndrome. When there is a fatty atrophy finding in the piriformis muscle, there may be no symptoms at all [10], but it can compress the sciatic nerve by causing a muscular shortening. In addition, it is known that pain relief by injection in the piriformis muscle is not easily achieved [5]. It is assumed that relief of the symptom after the injection in the piriformis muscle in this case report might be the result of the anti-inflammatory action of the steroid. We have decided that the patient's symptoms were due to the proximal sciatic neuropathy caused by post-radiotherapy fatty atrophy of the piriformis muscle, based on the series of changes in the piriformis muscle as shown by the MRI, clinical symptoms, and electromyography findings.
When treating cancer pain, the pain due to the damage of muscles or nerves that may be followed by radiotherapy and chemotherapy must be considered. Especially when radiating pain occurs in buttocks and legs after radiotherapy of a tumor existing in the pelvis, evaluation of not only the spinal lesion, but also proximal sciatic neuropathy, must be conducted.
Go to :
 XML Download
XML Download