

 PDF
PDF Citation
Citation Print
Print


Introduction
COVID-19 is caused by a newly found virus named as Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) by Corona study group (1). Originally it was believed to be a zoonotic disease, and later it started infecting humans (2); now, its showing human to human transmission and has become pandemic involving more than 200 countries. The virus was initially believed to have transmission by close contact and air droplets (2, 3) then later it was found to have possible air transmission also (4, 5). Air transmission prompted regulatory authorities to impose involuntary social distancing, locked down at home, improving personal hygiene, and using masks and gloves while having symptoms or going out for medical treatment or emergencies.
Go to : 
Etiopathogenesis of COVID 19 Infection
COVID 19 virus enters the human cell binding (Fig. 1), through its S spike protein (6), to Angiotensin-Converting Enzyme 2 (ACE2) receptor (7) present on type 2 Alveoli cells, endothelial cells, heart, kidney, liver and other organs (8). The human body has been shown to have an overreactive immune response called cytokine storm (3) caused by increased level of interleukin (IL)-2, IL-6, IL-7, granulocyte colony-stimulating factor (GSCF), interferon γ-induced protein 10 (IP10), monocyte chemoattractant protein-1 (MCP1), macrophage inflammatory protein (MIP1A) and tumor necrosis factor-alpha (TNF-α). Cytokine storm causes severe pneumonia by diffuse damage of type 2 alveolar, small blood vessels injury with capillary leakage into the air space causing pulmonary edema, pulmonary infarct, reduced oxygen exchange, and eventually acute respiratory distress syndrome (9). Many patients have been shown to have multiorgan failure involving the heart (myocarditis, thrombosis) (9), kidney, liver, and vascular system.

Go to :
Current Issues with Treatment Options of Severe COVID-19 Infection
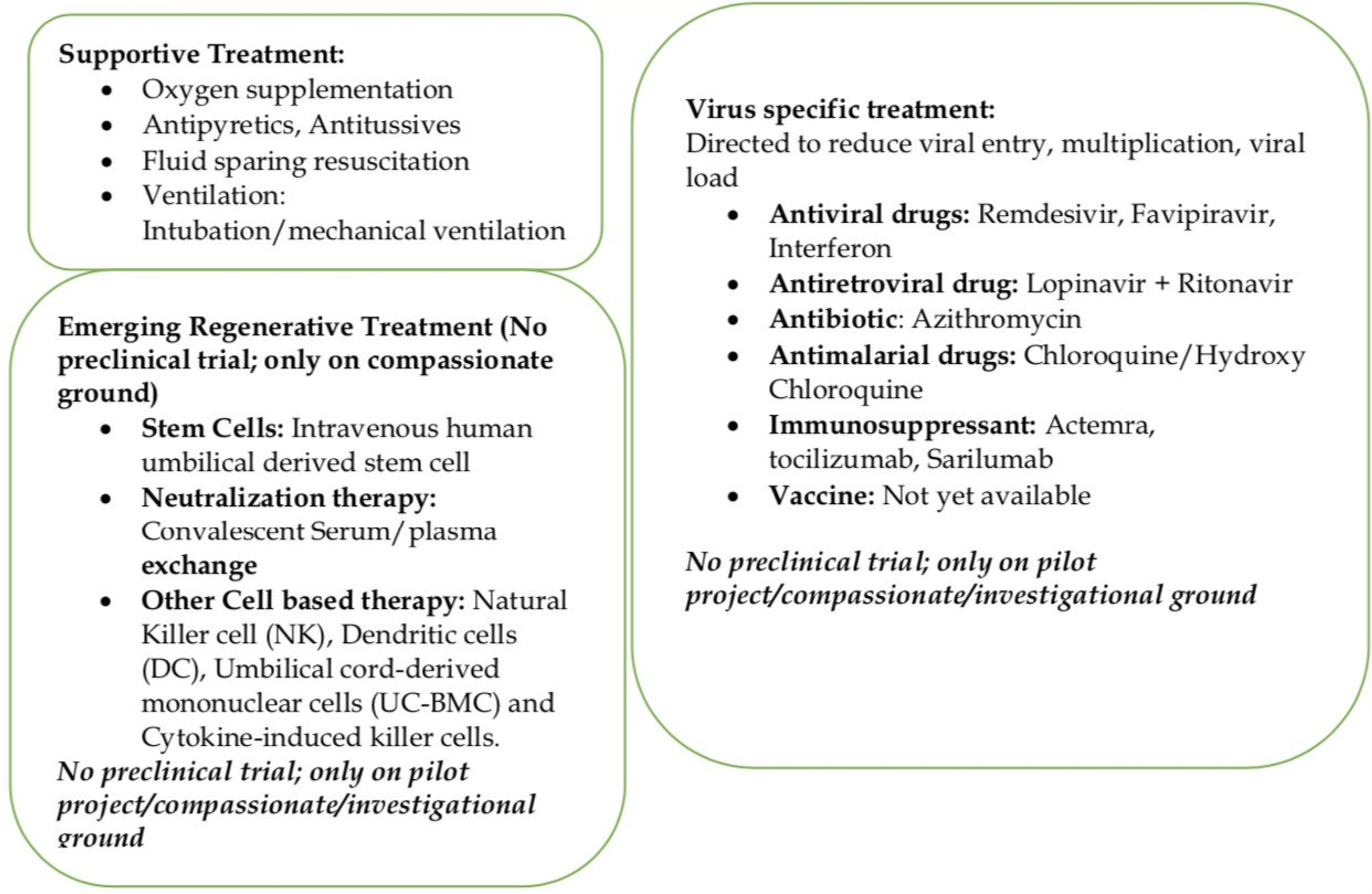
Around 80% of COVID-19 patients present with mild illness, 14% severe, and 5% present with critical illness (10). Severe COVID-19 infection leads pneumonia, ARDS (Acute Respiratory Distress Syndrome), multiorgan failure is being seen in elderly and patients with significant medical comorbidities like chronic lung disease, diabetes, cardiac, hepatorenal diseases, and cancer patients (10). Currently, there are no validated COVID-19 specific antiviral drugs, vaccines, immunotherapy, or other treatment options. These patients are being managed by supportive treatment (Fig. 2) with oxygenation, antibiotics, fluid and electrolytes replacement, mechanical ventilation with ICU support to prevent complications like pneumonia, ARDS, organ failure, and death (11). Over the last few months, some other treatment options (Fig. 2) including antiviral drugs (remdesivir, Favipiravir), antiretroviral drugs (Lopinavir+Ritanovir), antibiotic (Azithromycin), antimalarial drugs (Chloroquine/Hydroxy Chloroquine: increases the Ph in the endosomes of cell and prevent virus-endosome fusion required for viral replication; interfere with terminal glycosylation of cellular receptor ACE 2 (Angiotensin Converting Enzyme 2) and reduces virus affinity binding to ACE receptor), immunosuppressant (Actemra, or tocilizumab and Sarilumab/approved cks (chemokine) IL-6 receptor for Rheumatoid Arthritis) and vaccines are being used with variable results in many countries (11-14). Now many actual reasons for death, including virus-induced severe tissue damage, overactive body immune response (cytokine storm) to the virus, mechanical ventilation-induced injuries, are being debated among the treating physician and research scientists. Drug regulatory authorities and governments are also feeling pressure to ease the use of the options mentioned earlier on compassionate grounds in COVID-19 infection and to conduct clinical trials to validate their efficacy in COVID-19 infections.
Go to :
Role of Regenerative Medicine in Severe COVID 19 Infections
Stem cells
Mesenchymal stem cells have been shown to act by paracrine and juxtacrine signaling (15, 16) and to exhibit anti-inflammatory, anti-fibrotic (Fibroblast Growth Factor, Hepatic Growth Factor), angiogenic, mitogenic, antiapoptotic (17, 18) and immunoregulatory properties (pros-taglandin GE2, TNFα-stimulated gene-6, extracellular vesicles) (18-21). The majority of the intravenously injected stem cells get trapped in the lung veins and lung tissues. These trapped stem cells are resistant (immune) to Novel COVID-19 due to lack of surface ACE 2 receptor and TMRESS receptor on stem cells. Trapped stem cells release anti-inflammatory cytokines (22), angiogenic growth factor (23, 24), antimicrobial peptides (23, 25) extra-cellular vesicles (24, 25). These lung-specific anti-infla-mmatory mediators are released by stem cells activation through activation of Toll-Like Receptors (TLRs; pathogen-associated molecular pathogen receptors) present on stem cells by viral RNA (TLR3 also found in COVID-19) and viral unmethylated CpG-DNA (TLR9) (23, 26, 27). Angiopoietin-1 (Ang-1) and keratinocyte growth factor (KGF) help in the repair of alveolar-capillary barriers seen in ARDS (23, 28). Those promote lung healing and repair by improving the pulmonary microenvironment (IL-10, VEGF), protecting alveolar epithelial cells, and preventing pulmonary fibrosis (29-32). Stem cells also seem to work against COVID 19 by elevating the level of MSC-specific Interferon Stimulated Gene (ISG), which acts as a mediator of antiviral protection and by combined natural and inducible innate antiviral defense (23). Actions of stem cell at a pulmonary level are manifested in peripheral blood by a reduced level of inflammatory factors (pro-inflammatory cytokines: IFN-α, IFN-γ, IL-1β, IL-6, IL-12, IL-18, IL-33, TNF-α, TGFβ; chemokines: CCL 2, CCL3, CCL5, CXCL8, CXCL9, CXCL10) and increased level of anti-inflammatory factors and by suppressing immune cells (33). One recent study (34) reported the use allogeneic human umbilical cord-derived stem cells in a 65 years old female with COVID-19 infection on a non-invasive ventilator with severe pneumonia, ARDS, multiorgan failure, moderate anemia, hypertension, type 2 diabetes, electrolytes disturbance, immunosuppression and acute gastrointestinal bleeding (steroid side effect). The patient was not responding to steroid (methylpredniso-lone), antiviral drug (lopinavir/ritonavir, IFN-α inhalation) antibiotic (moxifloxacin) and immunosuppressant (Thymo-sin alpha). She had increased total leucocyte (TLC) and neutrophil count, decreased lymphocyte count, increased bilirubin and liver enzymes, and bilateral ground-glass opacity on C.T. (computer tomography) chest. The patient received three intravenous infusions of human umbilical cord-derived stem cells (5×107 hUCMSC) at three days apart; after second dosage her TLC/Neutrophil count reduced to a normal level, lymphocyte count increased to normal; serum bilirubin, CRP (C Reactive Protein), and ALT (Alaline Aminotransferase)/AST (Aspartate Amino-transferase) reduced gradually; the patient became ambulatory on 4th day and was out of ICU on 13th day with improved C.T. lung findings. The authors acknowledged, single case experience might not be suitable to recommend stem cell therapy but did suggest either alone or in combination with other immune-modulating agents, stem cells could help severe COVID-19 infected patients.
Similar results were seen in a pilot project (33) looking at the role of single intravenous dose (1×106 cells/kg body weight) of allogeneic human umbilical cord-derived stem cells in COVID-19 patients not responding well to expectant treatments. The study was conducted in Beijing YouAn Hospital, Capital Medical University, China after ethical approval from hospital and trial was reviewed by the scientific committee at International Society on Aging and Disease (ISOAD) and registered in the Chinese Clinical Trial Registry (ChiCTR2000029990). The study included seven COVID 19 infected patients (one critically severe, four severe, two common). Patients were assessed for 14 days for safety (allergic reaction, secondary infections, life-threatening events), primary efficacy (level of cytokines, CRP, oxygen saturation), secondary outcome (total lymphocyte count, fever, dyspnea, respiratory rate, C.T. chest) after the injection. The study showed improvement in symptoms and pulmonary function in 2 days, and three patients (one severe, two common infections) were discharged ten days after the treatment. Laboratory results showed a reduced level of C-reactive protein and TNF-α (Tumor Necrotic Factor), the disappearance of overactivated cytokine-secreting immune cells CXCR3+CD4+ T cells, CXCR3+CD8+ T cells, and CXCR (chemokine receptor) 3+ Natural Killer cells (3∼6 days); increased level of peripheral lymphocytes, CD14+CD11c+CD11b, regulatory D.C. cell & IL-10 (stem cell group). They also performed the 10× RNA-seq survey on 12.500 captured MSCs (mesenchymal stem cell), and results showed MSCs are ACE2 or TMPRSS2 negative and expressed a high level of anti-inflammatory and trophic factors (Transforming Growth Factor -β, Hepatic Growth Factor, Leucocyte Inhibiting Factor, Fibroblast Growth Factor, Vascular Endothelial Growth Factor, Epidermal Growth Factor, Brain-Derived Neurotrophic Factor, and Nerve Growth Factor). They concluded that transplanted stem cells are safe, make immune to COVID-19 infection, and help in severe COVID-19 infections; although the main issue with the study is lack of detailed clinical information, levels of inflammatory cytokines, and lymphocytes in three patients treated by placebo and six non-critical patients in the stem cell group.
Nevertheless, these two reports of stem cells in COVID-19 patients do show the beneficial role of stem cells as an additional tool along with other treatments. More properly done randomized studies with long-term follow-up would help establish the treatment protocols (indications, timing, dosages, interval, route, type of stem cell, follow-up criteria, and safety) for stem cell treatment in these patients. Although both these studies have used human umbilical cord-derived stem cells, they avoided autologous harvesting-related complications and might have better clonogenic, proliferation, migration, and chondrogenic potential than bone marrow-derived mesenchymal stem cell (35, 36). However, they are allogenic and might have cultural/social issues; and most of the published literature is on the efficacy and safety of the bone marrow or adipose tissue-derived stem cells. Mesenchymal stem cells from bone marrow, adipose tissue, or umbilical cord should be able to show a similar effect in COVID-19 infections. These can be harvested (bone marrow, adipose tissue) at an early stage in patients with a high risk of developing the severe COVID-19; can be expanded in the lab (for 1∼3 weeks) and used if the need arises at a later stage. Recently several clinical trials without any preclinical evidence have been registered in NIH and Chinese Clinical Trial sites for COVID-19 infections (23). These trials will be using MSC alone (systemic administration of human umbilical cord-derived, human menstrual blood-derived, adipose tissue-derived, Wharton Jelly derived stem cell), or in a combination of MSCs derived products (MSCs Exosomes by inhalation; Umbilical derived mononuclear cells conditioned medium; drugs like Ruxolitinib) or MSC derived exosomes (inhalation route) alone (23). A variable 1∼5 dosages of intravenous stem cell between 0.4 and 42×106 cells/kg−1 at two days interval will be used for these trials (23).
Go to :
Other Cell-Based Therapies
Now many trials are being proposed and will be started soon to see the efficacy and safety of other potential antiviral cells, including natural killer cells (N.K.), dendritic cells (D.C.), Umbilical cord-derived mononuclear cells (UC-BMC) and cytokine-induced killer cells (23). Recently, Cellularity, a clinical-stage company, has got FDA approval for Investigational New Drug (IND) application for the use of its registered CYNK-001 in adults with COVID-19 (37). It is a cryopreserved allogenic Natural Killer Cell derived from a human placental hematopoietic stem cell. CYNK-001 has been proposed to activating receptors such as NKG2D, DNAM-1, and the natural cytotoxicity recep-tors NKp30, NKp44, and NKp46, which bind to stress ligands and viral antigens on infected cells (37). It has also been proposed to show the expression of cytolytic molecules perforin and granzyme B, which kill recognized infected cells. Although these proposed actions of CYNK-001 have been suggested to help COVID-19 patients by reducing viral replication and eliminating the infected cells (37). However, there is uncertainty about the dosages, intervals, efficacy, and risk of increasing the severity by destroying the minimally infected cells or altering the other immune response against the COVID-19 virus.
Go to :
Convalescent Serum/Plasma
Historically, they had been one of the commonly used methods of providing passive immunological protection by transfusing convalescent serum/plasma to prevent or treat an infectious disease (measles, chickenpox). They have also been used for Middle East Respiratory Syndrome Coronavirus in the past and recently for COVID-19 infection in China; now increasingly being used in other countries (USA, Italy, France), and FDA has also allowed it for COVID-19. They are collected from patients who were previously positive for the COVID-19 test, currently asymptomatic for 2∼3 weeks, and are negative for the COVID-19 test. The patient’s blood is collected and screened for other infections (Hepatitis B, C, HIV, Cyto-megalovirus, Syphilis) and serum or plasma (titer of 1:160) is prepared; usual dosage ranges from one to multiple infusion of 200∼400 ml (ABO compatible) at few days’ intervals. These are generally given as a rescue therapy (38, 39) at an early stage of infection (low viral load/inoculum) for immediate antiviral protection. They mainly work by neutralization of viruses from passive antibodies and possibly by antibody-dependent cellular cytotoxicity or phagocytosis (38, 40). Many benefits of these therapies have been proposed, including the reduced viral load, severity, and hospital duration of COVID-19 patients (38, 41, 42). Now they are also being proposed for asymptomatic or mildly symptomatic COVID-19 positive healthcare professionals, as it gives immediate immunity, and they can reduce or avoid quarantine period and can continue to work in highly loaded hospitals. These treatments are generally have been safe & effective, but doubt has raised about the quality and titer of antibodies present in these products; also, unknown risk of blood infection or unknown infection, and remote antibody-dependent lung injury or enhanced viral infection (39, 40, 43). Plasma exchange has also been shown to reduce inflammatory cytokines, stabilizing endothelial membranes, and resetting the hypercoagulable state (42, 44, 45). One study (41) used plasma exchange transfusion in 3 pediatric patients (35∼40 ml/kg) on mechanical ventilation with acute ARDS & hemodynamic instability during 2009 H1N1 influenza. All the three patients benefited from anti-cytokine storm effects of plasma exchange and survived without any side effects. One randomized study (46) involving 106 patients with severe sepsis and shock; compared combined plasma exchange and standard care with standard treatment only, and showed a 28 days mortality rate of 33.3% in the plasma exchange group while 53.8% in the control group.
Go to :
Conclusions
COVID 19 pandemic is threatening our existence and has changed human life forever due to the current unavailability of a particular medicine, vaccines, and other treatment options. Many efforts have been made to prevent viral entry, reduce viral load, and to control the COVID-19 induced tissue damage. However, mortality remains a big issue due to cytokine storm and inadequate healing potential in elderly and compromised unhealthy patients. Regenerative Medicine could become an essential adjuvant treatment in these severely affected patients by harnessing the anti-inflammatory, immune-modulatory, angiogenic and healing properties of stem cells and neutralizing actions of plasma/serum exchange and immunotherapy.
Go to :
 XML Download
XML Download