

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
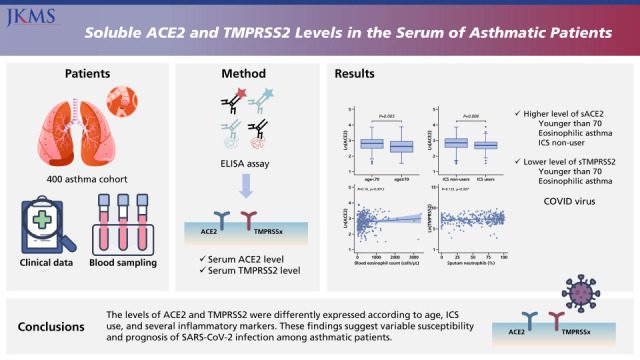
Nowadays, the world is facing unprecedented challenges from the coronavirus disease 2019 (COVID-19) crisis. Numerous clinical and epidemiological studies have been performed searching for risk factors associated with symptomatic infection or poor clinical outcomes. Thus far, males, older adults, and smokers are commonly considered susceptible to severe COVID-19 outcomes. Underlying diseases such as hypertension (HTN), diabetes mellitus (DM), cardiovascular diseases, and chronic obstructive pulmonary disease (COPD) have been identified as risk factors.12
The centers for disease control and prevention classified patients with moderate to severe asthma as a high-risk group. However, the contribution of underlying asthma on infection or progression of severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) infection remains largely unanswered.34 As angiotensin-converting enzyme 2 (ACE2) and transmembrane protease serine subtype 2 (TMPRSS2) serve as key entrance proteins in SARS-CoV-2 infection, their expressions have been evaluated in various airway specimens of asthmatic patients.5 The gene expression of ACE2 and TMPRSS2 varied according to atopy status or inflammatory phenotypes of asthma, indicating different vulnerabilities for SARS-CoV-2 infection.67 Nevertheless, the studies were mostly conducted at gene levels, not at the level of protein expressions.
Meanwhile, there were studies suggesting that higher circulating ACE2 levels may be associated with greater susceptibility to SARS-CoV-2 infection.89 These suggestions were mainly due to the findings that subjects with higher soluble ACE2 (sACE2) levels were in line with previously reported high-risk groups such as men, smokers, obese subjects, and diabetic subjects.89 On the other hand, in patients with COVID-19, a substantial increase in blood ACE2 was noted during the disease course, especially in severe diseases, suggesting sACE2 as protective proteins produced in response to viral shedding.1011 This is in accordance with the development of human recombinant sACE2 as a novel therapeutic option for COVID-19.12 As blood biomarker is easy to obtain and able to reflect the systemic condition of the host, more accumulated data regarding sACE2 are required to understand their role and assess their potential as biomarkers in various medical backgrounds.
Thus far, the level of sACE2 has never been investigated in the blood of asthmatics. In addition, there is a paucity of data on the soluble form of TMPRSS2 (sTMPRSS2). In the present study, we sought to evaluate levels of both circulating ACE2 and TMPRSS2 in adult asthmatics and examine how they vary with the clinical characteristics.
Go to : 
METHODS
Study population
We randomly selected asthmatic patients from a preexisting asthma cohort, which is the Cohort for Reality and Evolution of Adult Asthma in Korea (COREA). The COREA is a longitudinal clinical cohort of adult asthmatics based in 35 referral hospitals in Korea.131415 We included participants who had been diagnosed with asthma based on the presence of asthmatic symptoms with objective evidence of airway reversibility or hypersensitivity. Serum samples were obtained at enrollment.
Clinical and demographic variables
Data on demographic profile, comorbidities, and clinical features of asthma were collected. These data included demographic factors, age, gender, body mass index (BMI), and smoking history. Comorbidities such as HTN, DM, chronic idiopathic urticaria (CIU), and rhinitis were reviewed. Information on comorbidities was collected using a self-reported questionnaire. The participants’ primary diagnosis of aspirin-exacerbated respiratory disease (AERD) or asthma and COPD overlap (ACO) was also reviewed. Diagnoses of AERD and ACO were decided by a physician based on the history and airway obstruction pattern, respectively. The skin prick test (SPT), serum total IgE, induced sputum analysis, blood eosinophils, fractionated exhaled nitric oxide (FeNO), and spirometry were analyzed. Atopy was defined as the positive SPT for at least one aeroallergen. The levels of asthma treatment were classified according to Global Initiative for Asthma (GINA) 2020 guidelines.16
Measurement of ACE2 and TMPRSS2
Serum sACE2 levels were measured using an ACE2 enzyme-linked immunosorbent assay (ELISA) kit (CUSABIO, Wuhan, China). The detection levels of the kit ranged from 0.156 ng/mL to 10 ng/mL, with an intra-assay coefficient of variation (CV)% < 8% and inter-assay CV% < 10%. Serum sTMPRSS2 levels were measured using a TMPRSS2 ELISA kit (USCN Life Science &Technology Company, Missouri, TX, USA). The detection levels of the kit ranged from 0.156 ng/mL to 10 ng/mL, with an intra-assay CV < 10% and inter-assay CV% < 12%.
Statistical analysis
Continuous variables were expressed as mean ± SD, while categorical variables were expressed as frequency (%). The levels of sACE2 and sTMPRSS2 underwent a natural log transformation since they were not normally distributed. The level of TMPRSS2 was converted to pg/mL before log transformation. Comparisons between groups were conducted using student’s t-test or the χ2 test. Missing information was not imputed. Univariate linear regression analyses were performed to find factors associated with sACE2 and sTMPRSS2. Multivariate linear regression analyses were further conducted using the variables with P value under 0.1. Correlations between protein levels and clinical characteristics were evaluated using Spearman’s correlation tests. A two-sided P value < 0.05 was considered significant. All statistical analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA).
Ethics statement
The study was reviewed and approved by the Institutional Review Board of Asan Medical Center (2012-0234), and all patients provided written informed consent.
Go to :
RESULTS
Characteristics of the participants
The characteristics of the 400 participants are summarized in Table 1. The mean age of the participants was 51.54 years. Females comprised 63.2% of the study population. More than half of the patients (247/400, 61.8%) had never been smokers. The mean level of serum IgE was 417.84 kU/L, and 55.8% of the patients were atopic. A hundred and thirty-eight patients had blood eosinophils 200 cells/µL or greater. The mean percentage of sputum eosinophils and FeNO was 9.81% and 52.53 ppb, respectively. Regarding comorbidities, rhinitis was most common, followed by CIU, HTN, and DM. The proportion of patients with AERD and ACO was 4.3% and 8.3%, respectively. At the time of the blood sampling, 142 patients (142/400, 35.5%) were using inhaled corticosteroids (ICS), while the rest of them (258/400, 64.5%) were not. The patients who were not on ICS were either those with newly diagnosed asthma or were on a cessation of ICS for at least three months. When we reviewed the asthma medication after enrollment, 86.5% of patients (346/400) initiated or maintained medium-to-high-dose ICS, which was GINA step 4 and 5 treatment. The mean level of serum ACE2 and TMPRSS2 was 17.29 ng/dL and 2.28 ng/dL, respectively. When we compared the baseline characteristics of the patients according to use of ICS, demographic features, inflammatory markers, lung function, and required treatment level was comparable between two groups. Only higher BMI and lower prevalence of AERD was noted in patients who were using ICS when blood sampling was conducted.
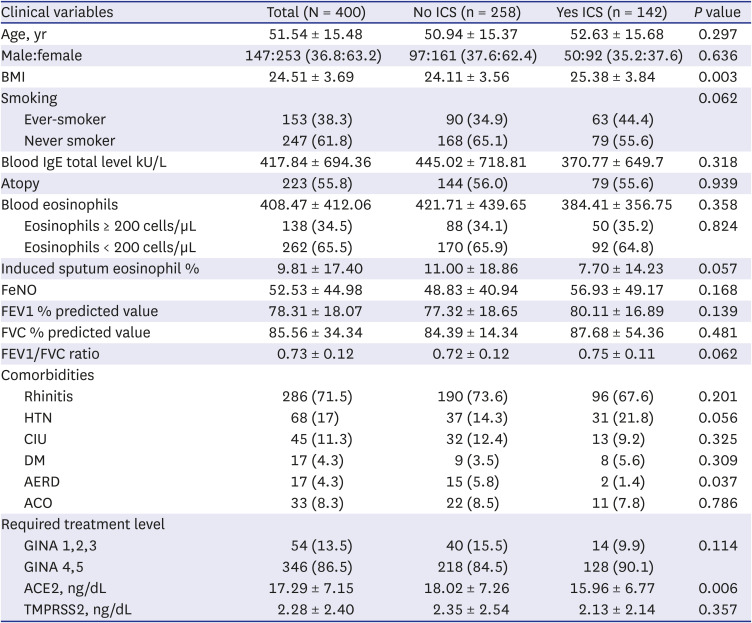
Table 1
Baseline demographics and clinical characteristics of the participants
Data are presented as mean ± SD or number (%).
BMI = body mass index, FeNO = fractional exhaled nitric oxide, FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, HTN = hypertension, CIU = chronic idiopathic urticaria, DM = diabetes mellitus, AERD = aspirin-exacerbated respiratory disease, ACO = asthma chronic obstructive pulmonary disease overlap, ICS = inhaled corticosteroids, GINA = Global Initiative for Asthma, ACE2 = angiotensin-converting enzyme 2, TMPRSS2 = transmembrane protease serine subtype 2.
![]()
Different levels of serum ACE2 according to characteristics of asthmatics
Univariate linear regression analyses found that the subgroups of elderly (≥ 70 years) (β coefficient [β], −0.178; 95% confidence interval [95% CI], −0.301, −0.054; P = 0.005), eosinophilic asthma (β, 0.104; 95% CI, 0.018, 0.190; P = 0.018), and ICS users (β, −0.116; 95% CI, −0.202, −0.031; P = 0.008) were significantly associated with serum sACE2. The levels of sACE2 were not significantly affected by sex, BMI, smoking history, atopy, and lung function. The coexistence of HTN, DM, CIU, or rhinitis also did not affect sACE2 levels (Table 2). In multivariate linear regression analyses, age and ICS still remained significant (Table 3).
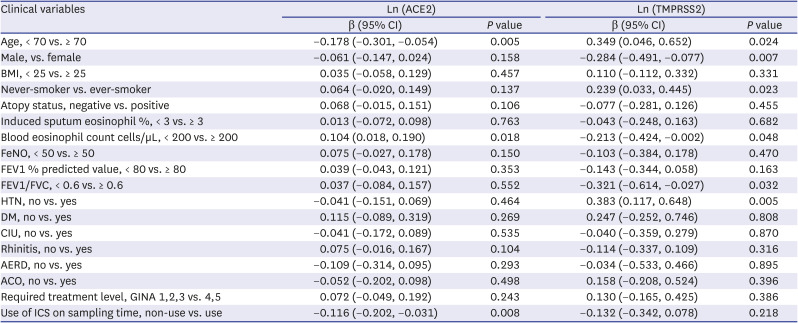

Table 2
Univariate linear regression analyses of subgroups associated with sACE2 and sTMPRSS2
ACE2 = angiotensin-converting enzyme 2, TMPRSS2 = transmembrane protease serine subtype 2, sACE2 = soluble ACE2, sTMPRSS2 = soluble form of TMPRSS2, CI = confidence interval, BMI = body mass index, FeNO = fractional exhaled nitric oxide, FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, HTN = hypertension, DM = diabetes mellitus, CIU = chronic idiopathic urticaria, AERD = aspirin-exacerbated respiratory disease, ACO = asthma chronic obstructive pulmonary disease overlap, GINA = Global Initiative for Asthma, ICS =inhaled corticosteroids.
![]()
Table 3
Multivariate linear regression analyses of subgroups associated with sACE2 and sTMPRSS2
ACE2 = angiotensin-converting enzyme 2, TMPRSS2 = transmembrane protease serine subtype 2, sACE2 = soluble ACE2, sTMPRSS2 = soluble form of TMPRSS2, CI = confidence interval, FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, HTN = hypertension, ICS = inhaled corticosteroids.
![]()
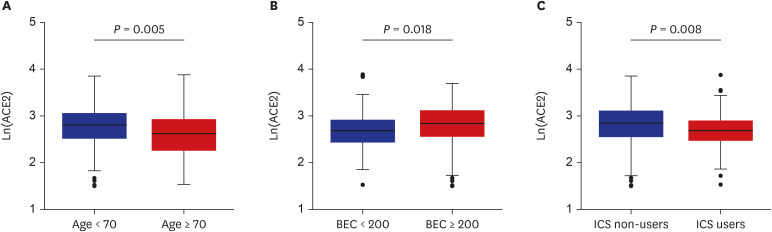
When we compared the level of sACE2 according to various demographic and clinical characteristics, the elderly (≥ 70 years) had significantly lower sACE2 levels than the younger patients (2.61 ± 0.49 vs. 2.79 ± 0.40, P = 0.005). The serum level of the natural log-transformed sACE2 was significantly greater in the eosinophilic (blood eosinophils ≥ 200/µL) asthma group (2.81 ± 0.42 vs. 2.70 ± 0.40, P = 0.018). Participants using ICS at the time of blood sampling reported significantly lower levels of serum sACE2 compared to the patients who were not taking ICS (2.69 ± 0.40 vs. 2.81 ± 0.43, P = 0.008) (Fig. 1).
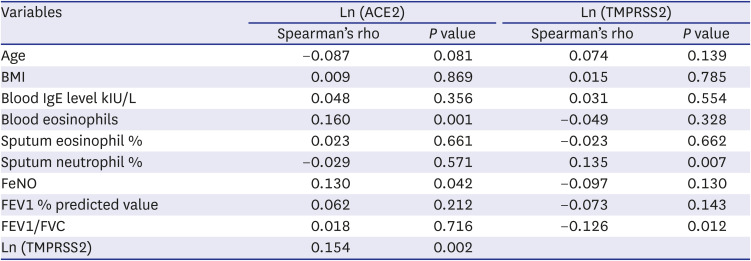
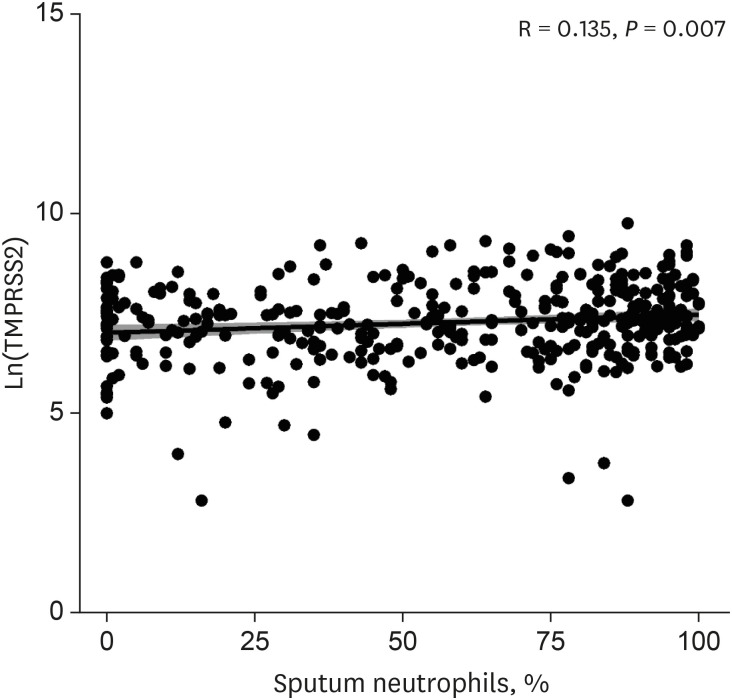
In regards to correlation between continuous variables and sACE2 (Table 4), blood eosinophils (Spearman’s rho [ρ], 0.160; P = 0.001) and FeNO (ρ, 0.130; P = 0.042) were positively correlated with sACE2 (Fig. 2), while the sputum eosinophil percentage did not show any significant association with sACE2. The level of sACE2 was significantly associated with sTMPRSS2 (ρ, 0.154; P = 0.002).
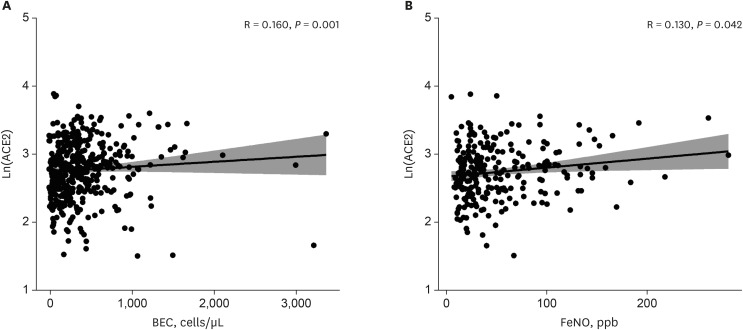 | Fig. 2Correlation between ACE2 and eosinophilic inflammatory markers. The correlation between ACE2 and eosinophilic inflammatory markers including BEC (A) and FeNO (B).ACE2 = angiotensin-converting enzyme 2, BEC = blood eosinophil count, FeNO = fractional exhaled nitric oxide.
|
Table 4
Correlation between ACE2, TMPRSS2, and clinical variables
ACE2 = angiotensin-converting enzyme 2, TMPRSS2 = transmembrane protease serine subtype 2, BMI = body mass index, FeNO = fractional exhaled nitric oxide, FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity.
![]()
Different levels of serum TMPRSS2 according to the characteristics of asthmatics
The univariate linear regression analyses found that the subgroups of elderly (≥ 70 years) (β, 0.349; 95% CI, 0.046, 0.652; P = 0.024), female (β, −0.284; 95% CI, −0.491, −0.077; P = 0.007), ever-smoker (β, 0.239; 95% CI, 0.033, 0.445; P = 0.023), eosinophilic asthma (β, −0.213; 95% CI, −0.424, −0.002; P = 0.048), forced expiratory volume in 1 second/forced vital capacity (FEV1/FVC) ratio greater than 0.6 (β, −0.321; 95% CI, −0.614, −0.027; P = 0.032), and HTN (β, 0.383; 95% CI, 0.117, 0.648; P = 0.005) were significantly associated with serum TMPRSS2. The levels of sTMPRSS2 were not affected by overweight status and atopy. Diagnosis with DM, CIU, rhinitis, AERD, and ACO also did not affect sTMPRSS2 levels. Contrary to sACE2, ICS use was irrelevant to sTMPRSS2 levels (Table 2). We have noted that none remained significant association with sTMPRSS2 when multivariate linear regression analyses were performed (Table 3).
Comparisons of the sTMPRSS2 levels between predefined subgroups also revealed that the elderly (≥ 70 years) had significantly lower sTMPRSS2 than the younger patients (7.59 ± 0.92 vs. 7.24 ± 1.0, P = 0.024). The TMPRSS2 levels were lower in females and never-smokers compared to males (7.18 ± 1.07 vs. 7.46 ± 0.92, P = 0.007) and ever-smokers (7.19 ± 1.09 vs. 7.43 ± 0.88, P = 0.023), respectively. Patients with lower blood eosinophils (< 200 cells/µL) and FEV1/FVC ratio (< 0.6) reported the higher TMPRSS2 than those with eosinophilia (eosinophils ≥ 200/µL) (7.42 ± 0.96 vs. 7.21 ± 1.05, P = 0.048) and better lung function (FEV1/FVC ≥ 0.6) (7.56 ± 0.91 vs. 7.24 ± 1.04, P = 0.032). Patients with HTN had higher serum TMPRSS2 compared to the others (7.60 ± 1.03 vs. 7.22 ± 1.01, P = 0.005) (Fig. 3).
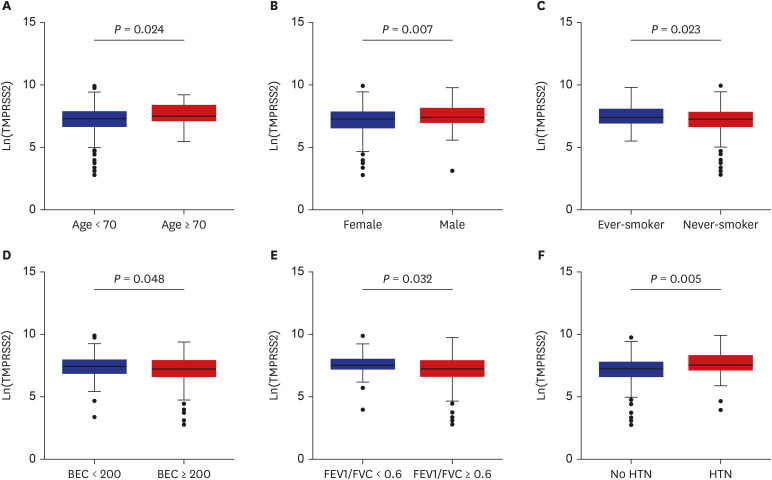 | Fig. 3Relationship between TMPRSS2 levels and clinical variables. The level of TMPRSS2 were compared between subgroups according to age (A), sex (B), smoking history (C), BEC (D), FEV1/FVC (E), and presence of HTN (F).TMPRSS2 = transmembrane protease serine subtype 2, BEC = blood eosinophil count, FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, HTN = hypertension.
|
Go to :
DISCUSSION
In the present study, we investigated the ACE2 and TMPRSS2 levels in the serum of patients diagnosed with asthma according to various demographic and clinical characteristics. Higher levels of serum ACE2 were noted in the patients younger than 70 years old, those with eosinophilic asthma, and ICS non-users. Meanwhile, greater sTMPRSS2 levels were observed in patients aged 70 years or older, males, and ever-smokers. The patients whose blood eosinophils were less than 200 cells/µL, FEV1/FVC less than 0.6, and were hypertensive were associated with the higher sTMPRSS2 levels. In multivariate linear regression analyses, only age and ICS use remained significantly associated with sACE2. Nevertheless, blood eosinophils and FeNO levels were positively correlated with serum ACE2, while the proportion of sputum neutrophils was positively correlated with sTMPRSS2. Collectively, different levels of sACE2 and sTMPRSS2 in asthmatics may suggest the heterogeneity of susceptibility and disease course of COVID-19 in asthmatics according to age, use of ICS, and expression of inflammatory markers.
In spite of numerous studies investigating gene expressions of ACE2 in tissues, far fewer data have been published on circulating ACE2, especially in asthmatic patients.91718 Kornilov et al.17 reported that plasma sACE2 levels were higher in the older participants in a large wellness program cohort composed of 2,051 subjects whose ages ranged from 22 to 87 years. Pavel et al.18 also identified a positive correlation between serum ACE2 protein level and age in healthy subjects. Meanwhile, in a cohort composed of elderly populations aged 66–96 years, age and sACE2 tend to have a negative correlation, despite statistical insignificance (β, −0.0014; 95% CI, −0.0029, 0.0000; P = 0.057). Most recently, AlGhatrif et al.19 reported a positive association in participants below the age of 55 years and a negative association in older participants. In our cohort, asthmatic patients aged 70 years and above had lower levels of sACE2 than younger patients, which was the first report of sACE2 levels in asthmatics.
Our study also found that there was a higher level of sACE2 in patients with eosinophilic asthma. In addition, blood eosinophils and FeNO were significantly correlated with serum ACE2. In previous studies, when analyzing bronchial epithelium from patients with asthma, those with peripheral eosinophilia reported lower ACE2 gene expression.7 In asthmatic children, ACE2 expression in nasal epithelial cells was inversely associated with type 2 biomarkers, such as the number of positive allergen-specific IgE test results, total IgE level, and FeNO, except blood eosinophils.6 When Kermani et al.20 measured ACE2 gene expressions in sputum, bronchial brushing, and bronchial biopsy, blood eosinophils were positively correlated with ACE2 expression in sputum. We have also demonstrated lower ACE2 serum levels in ICS users compared to non-users. Peters et al. found significantly lower ACE2 RNA expression levels in the sputum cells of asthmatics on ICS.21
The expression pattern of serum TMPRSS2 was different from that of ACE2. In contrast to ACE2, aged (≥ 70 years) patients had higher levels of TMPRSS2 than younger patients. Moreover, males and ever-smokers were associated with higher TMPRSS2 expressions. Regarding the clinical features of asthma, sTMPRSS2 was lower in eosinophilic asthma. Rather, it was positively correlated with sputum neutrophil percentage and negatively correlated with the FEV1/FVC ratio. The different expressions of ACE2 and TMPRSS2 have been persistently reported in studies evaluating gene expressions.2022 Even though the role of circulating TMPRSS2 is still elusive, we could infer that the demographic and clinical features of asthma are associated with gene and protein expressions of TMPRSS2.
The inconsistent directions between gene expressions of target tissue and circulating protein could be explained by several reasons; 1) the expressed genes do not always result in the production of proteins, 2) tissue ACE2 should undergo protein shedding to release sACE2, requiring the involvement of ADAM-17 proteases, and 3) ACE2/TMPRSS2 are widely distributed across the organs, and 4) the origin of circulating ACE2/TMPRSS2 is hard to determine.23 Therefore, further research is needed to understand the mechanical linkage between cell membrane receptors of tissue and circulating proteins in blood.
Mechanistically, sACE2 in the blood could play a protective role by trapping the circulating viruses, interfering with their cell entry.24 In accordance, an ex vivo experiment reported the inhibitory effect of human recombinant sACE2 on SARS-CoV-2 infection using human organoid models.25 Consequently, sACE2 is considered as one of the potential therapeutic agents working as a decoy receptor.26 In this regard, lower levels of baseline sACE2 could be a poor prognostic factor in COVID-19 patients with asthma, who were elderly (≥ 70 years), a non-eosinophilic phenotype, and ICS users. However, the clinical relevance of the sACE2 level remains to be determined, particularly in the context of SARS-CoV-2 infection. More data are needed to validate clinical usefulness and define the optimal cut-off value of sACE2 in diverse medical conditions. Although the role of circulating TMPRSS2 is yet to know, the level of ACE2 and TMPRSS2 was significantly correlated in our subjects. This may suggest the presence of linkage between each other regardless of viral infection.
There are several limitations to the present study. First, there was no reference range derived from healthy controls. However, in terms of gene expression, the level of ACE2 and TMPRSS2 in sputum was comparable between asthmatics and healthy participants, although different level was noted in sub-analyses among asthmatics.21 We have also noted similar level of serum ACE2 and TMPRSS2 in age and sex-matched patients with CIU (data not shown). Consequently, the results of our study need to be interpreted among the patients with asthma. Second, the relationship between the risk of infection or prognosis of COVID-19 and sACE2 or sTMPRSS2 is still largely unanswered since our study was conducted in a preexisting cohort unaffected by the SARS-CoV-2 infection. More data need to be accumulated regarding the disease course and expression of sACE2 in asthmatics diagnosed with COVID-19. Thirdly, since the presence of comorbidities was obtained from the self-reporting questionnaires, their prevalence might have been underestimated. In addition, we could not obtain information on the use of ACE inhibitors, which could have affected the circulating ACE2 levels especially in patients with HTN.27 Lastly, as this is an observational study conducted cross-sectionally, the causal relation between clinical hallmarks and ACE2/TMPRSS2 is hard to evaluate.
Nevertheless, this is the first study demonstrating the serum level of ACE2 and TMPRSS2 in a large asthma cohort. Our data suggest that the demographic and clinical features of asthma patients may contribute to the vulnerability or severity of COVID-19 infection. Future studies are warranted to define the clinical meaning of the sACE2 and sTMPRSS2 levels in the context of SARS-CoV-2 infection.
Go to :
 XML Download
XML Download