

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Breast cancer occurs frequently in women,1 and radiation therapy (RT) is being actively implemented as a postoperative treatment to prevent recurrence. One of the new trends in breast cancer RT is the introduction of hypofractionated RT.2 Generally, hypofractionated RT showed satisfactory results in terms of recurrence rate based on treatment.34
Biologically, it is known that good treatment results can be obtained when hypofractionated RT for breast cancer is performed because the estimated alpha/beta value of breast cancer is 3.6 Gy according to a previous radiobiologic report by Yarnold et al.5 Regarding radiation dose, the UK Standardization of Breast Radiotherapy (START) B trial6 showed that various hypofractionated radiation doses (2.7–3.3 Gy/fraction) were as effective as standard conventional RT doses (1.8–2 Gy/ fraction). However, the 3.3 Gy/fraction group showed a high rate of shoulder stiffness afterwards.7 Considering the high normal tissue side effect rate reported in the UK START trial7 and 1-week schedule UK FAST trial (CRUKE/04/015),8 the RT with a 3-week hypofractionated radiotherapy schedule of ≤ 3 Gy/fraction is currently preferred over a 1-week hypofractionated RT schedule. The recent Danish Breast Cancer Group (DBCG) 3-week schedule HYPO Trial9 also bolstered this view. Moreover, long-term follow-up results from the large-scaled Canadian hypofractionation RT trial clearly bolstered the view that hypofractionated RT (42.5 Gy/16 fractions, 2.67 Gy/fraction) was compatible to conventional RT (50.0 Gy/25 fractions) in terms of safety, cosmesis, and effectiveness.10 Acute skin toxicity in hypofractionated RT seems to be rare, even when treated with chemotherapy.11 The incidence of lung or cardiac toxicity in hypofractionated RT also seems to be rare.121314 Thus, the current National Comprehensive Cancer Network guideline15 recommended hypofractionated RT for early breast cancer patients and considered it a form of standard therapy.
In early-stage breast cancer patients, shortening the treatment period contributes to increased economic feasibility and patient satisfaction. If the same treatment effect can be obtained at a lower cost, it can be said to be a more efficient treatment. Hypofractionated RT is superior to conventional RT in terms of cost-effectiveness. For patients who have to go to the hospital from long distances, it is also advantageous in terms of the saving time required for commuting to the hospital. Thus, many breast cancer patients prefer hypofractionated RT.
Regarding tumor bed boost RT that usually consists of 4–5 times of an electron beam, a recent multinational large-scale study16 of ductal carcinoma in situ (Tis) patients reported better treatment outcomes for recurrence in the boost RT group than in the non-boost group. Therefore, it seems more desirable to implement boost RT in all patients, even in cases with hypofractionated RT. Therefore, our study also added boost RT to whole-breast RT in general.
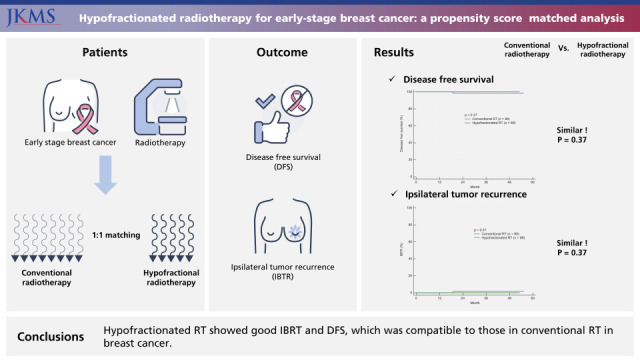
In this study, we compared the ipsilateral breast tumor recurrence (IBTR) of breast cancer patients treated with hypofractionated RT with that of conventional RT patients during the same period to compare treatment outcomes. We have treated patients by introducing breast cancer hypofractionated RT relatively early in Korea.2 Basically, we used the radiation schedule implemented in a previous Canadian trial.10 Herein, we demonstrated the effects of treatment and the safety of hypofractionated RT compared to conventional RT in breast cancer. The hypothesis is that hypofractionated RT for early stage breast cancer is as effective as conventional RT for local tumor control. The co-primary endpoints of this study were disease-free survival (DFS) and IBTR. Additionally, cost effectiveness analysis was implemented.
Go to : 
METHODS
Patients and treatment
Breast cancer patients who underwent breast-conserving surgery for early-stage breast cancer were divided into two groups based on RT methods: the hypofractionated RT and conventional RT groups. RT methods were selected based on physician preferences. Low nuclear grade, low T stage, and hormone receptor-positive patients were considered to have a low risk of local relapse, and those patients tended to be treated frequently with hypofractionated RT. A total of 13–16 fractions of whole breast RT and 3–4 fractions of tumor bed boost were used for hypofractionated RT. In contrast, 25–28 fractions of whole breast RT (median total dose: 50.4 Gy) and 5 fractions of tumor bed boost were applied for conventional RT. Most patients underwent boost RT after whole-breast RT. For hypofractionated RT, the commonly used dose scheme was 42.56 Gy/16 fractions whole breast RT plus 10.64 Gy/4 fractions tumor bed boost.
All patients enrolled in this study were women (aged > 18 years) and had undergone surgery and RT at our hospital. The exclusion criteria consisted of the following: patients 1) with a history of other cancers, 2) who received neoadjuvant chemotherapy, 3) who had positive margin with tumor at pathologic reports (R1 or R2 resection), and 4) who had regional lymph node metastases.
All patients underwent computed tomography simulation on the wing board. Treatment planning was performed using the Pinnacle radiation treatment planning (RTP) system (Philips Medical Systems, Cleveland, OH, USA) and Monaco RTP system (Elekta AB, Stockholm, Sweden) were acquired before the treatment contouring and planning were carried out, using 6 MV tangent fields using two photon beams and 9 MeV-12 MeV electron beam. Neither Intensity modulated radiotherapy nor 3-dimensional conformal RT was used for planning. The following dose constraints were used for computerized RT planning: ipsilateral lung V20 Gy < 40% and heart V35 Gy < 30%.
This study was conducted with patients who had no lymph node metastases and all the patients did not receive regional nodal irradiation. In addition, most hypofractionated RT patients additionally received four fractions of boost treatment after whole breast radiation. The total dose to the targeted ipsilateral breast was calculated using the biologically equivalent dose in 2 Gy fractions (EQD2) assuming the α/β ratio of 3.0 Gy; whole breast dose for hypofrationated RT and tumor bed boost dose were estimated 47.91–48.18 Gy and 11.00–12.04 Gy (as EQD2).
Measurement of treatment outcome
The IBTR, regional nodal relapse, and distant metastasis rates were assessed separately. Actuarial IBTR rate, DFS, and survival were defined from the operation date to events.
Acute toxicity was defined as side effects occurring within 6 months after RT. The acute skin toxicity rate was checked using electronic medical records. NCI Common Terminology Criteria for Adverse Events (CTCAE) version 5.0 was used for grading toxicity.
Statistical analysis
For statistical analysis, SPSS (SPSS Inc., Chicago, IL, USA) version 25.0 and MedCalc (MedCalc Software, Mariakerke, Belgium) were used. The side effect rate, crude IBTR, and overall relapse were compared using a cross table and Fisher’s exact test. To reduce selection bias, propensity score matching (PSM) was applied to the evaluation. PSM was estimated using the following variables: T stage, age, tumor nuclear grade, and hormonal subtype. Hypofractionated RT patients were matched in a 1:1 ratio to conventional RT patients. Time-dependent IBTR and DFS were calculated using the Kaplan-Meier curve. The log-rank test was used to determine the effect of prognostic factors.
Ethics statement
This retrospective study was examined and approved by the Institutional Review Board in Inje University Busan Paik Hospital and the requirement for informed consent was waived (IRB No. 2021-02-010).
Go to :
RESULTS
Patient characteristics
Patients (n = 280) who received radiation therapy from September 2016 to December 2020 were followed up, and the median follow-up period was 23.6 months (range 3.0–55.3 months). Patient characteristics are summarized in Table 1. Most patients were in the T1 stage, whereas hormone receptor-positive (luminal A and luminal B) patients accounted for the largest portion in both groups. Additionally, there was no significant difference in pathological features between the two groups. Most patients received boost RT and received endocrine therapy, whereas less than half of the patients received adjuvant chemotherapy. Of all patients, few underwent targeted therapy. Although there were no statistical differences, older patients (> 50) tended to receive more conventional RT. Moreover, T2 patients, high nuclear grade patients, and non-hormone receptor-positive patients were slightly more in the conventional RT group, and this difference in ratio was corrected by PSM. The 89 patients treated with hypofractionated RT were matched with 89 patients treated with conventional RT (1:1 matching).
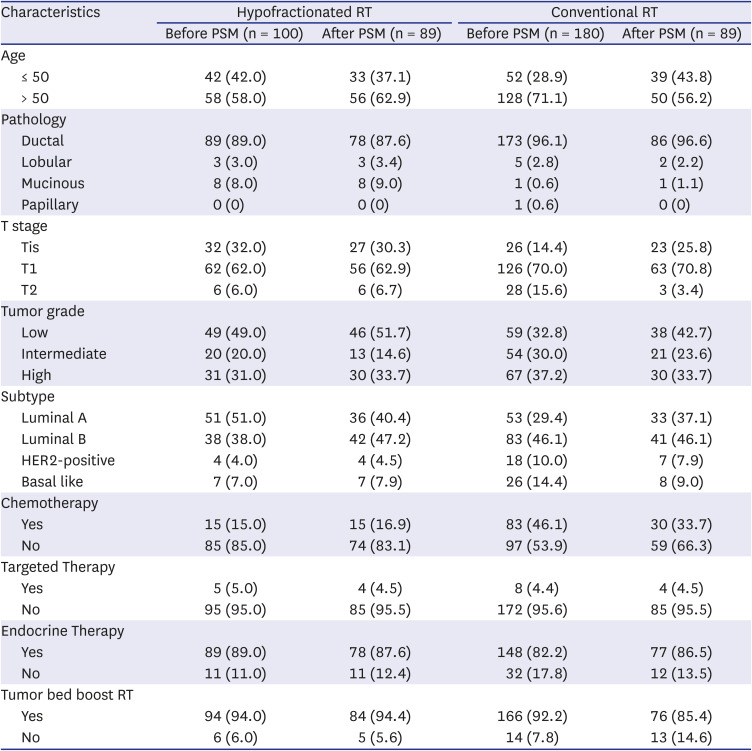
Table 1
Patient characteristics
![]()
Relapse patterns
Table 2 summarizes the characteristics of patients with relapse and shows the differences in recurrence rates between hypofractionated RT and conventional RT. After PSM, overall cancer recurrence rates were compared again.
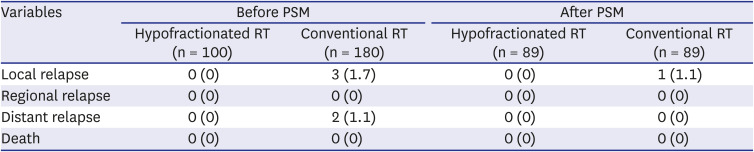
Table 2
Pattern of failure
![]()
Regarding treatment failure, three local recurrence occurred in the breast. The other two patients had distant metastases (relapses in the bone and lung) before PSM. Before PSM, IBTR was absent in the hypofractionated RT group and in three patients (3.0%) in the conventional RT group. After PSM, there was only one IBTR in the conventional RT patient group (1.1% vs. 0% in the hypofractionated RT group). No distant recurrence was observed in conventional RT group after PSM. Table 3 describes the characteristics of the patient with IBTR and overall recurrence rate.
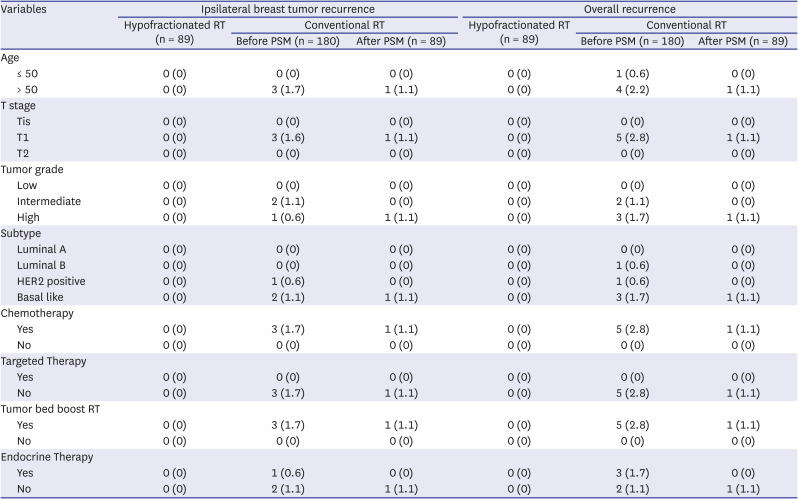
Table 3
Difference of ipsilateral breast tumor recurrence and overall relapse
![]()
There was no recurrence in the hypofractionated RT group with respect to the recurrence rate of the patients. In contrast, in conventional RT, five patients (5/180, 2.8%) had recurrence during the entire follow-up period. Table 3 also shows the distribution of the patients with relapse. One patient remained in relapse (1.1%) after PSM correction.
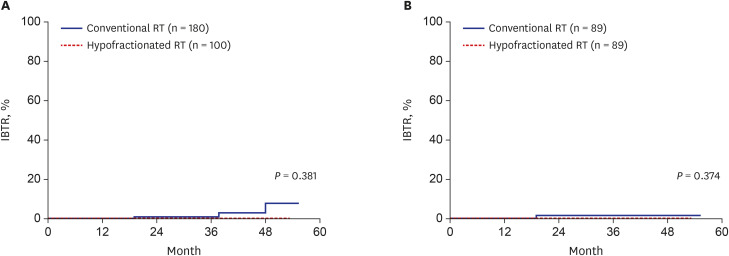
Fig. 1 shows the difference between the IBTR (local relapse) of both groups: Fig. 1A shows the difference between the hypofractionated RT group and the conventional RT group before PSM correction (P = 0.381), and Fig. 1B shows the difference in IBTR after PSM correction (3-year IBTR 0% vs. 1.6%, P = 0.374). There were no statistically significant differences between the groups after PSM correction.
Survival outcomes
Fig. 2 shows the differences in DFS between the two groups: Fig. 2A shows the DFS difference before PSM correction (P = 0.079), and Fig. 2B shows the difference after PSM correction. After matching, the 3-year DFS was 100% in the hypofractionated RT group and 98.4% in the conventional RT group; there were no statistically significant differences of DFS after PSM (P = 0.374).
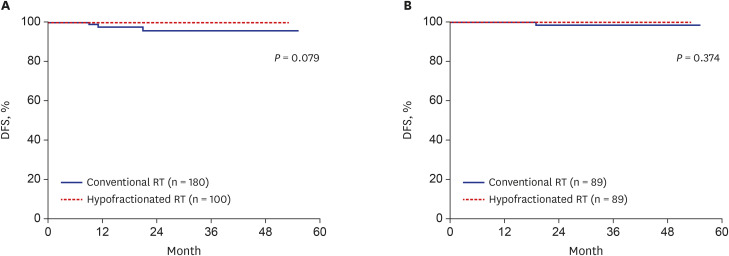
None of the patients died during the follow-up period. Thus, the overall survival was 100% in both groups.
Toxicity
Overall, acute skin toxicity of grade 2 or higher was rare (hypofractionated RT, 9/89 [10.1%] cases vs. conventional RT, 2/89 [2.2%] cases after matching), and there was no statistically significant difference in frequency. Three patients complained of fibrotic changes in the irradiated breast after hypofractionated RT, whereas one patient complained of fibrotic changes after conventional RT. In addition, one patient took medication because of pneumonitis after hypofractionated RT, and no patient took medication after conventional RT. Finally, no patients were hospitalized for side effects after RT.
Cost effective analysis
The cost of RT was compared in the Table 4. Hypofractionated RT saved 890,263 won (26.6% reduction) of the total cost of RT, compared to conventional RT (as of 31 August 2021). To be specific, a deductible for a patient were reduced by 45,861 won (26.8% reduction). Korea national health care insurance burden was reduced by 844,402 won (26.5% reduction). It can also be expected to reduce indirect costs due to shortening the treatment period (2 weeks) in hypofractionated RT.
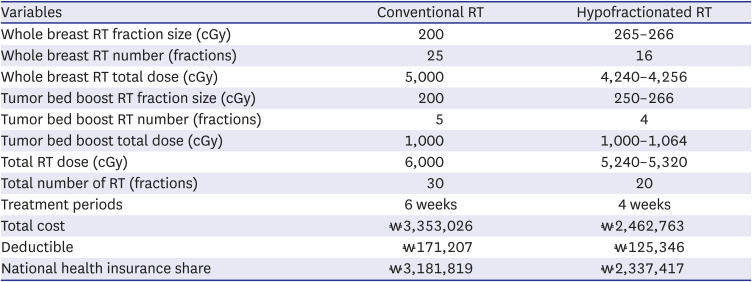
Table 4
Comparison of cost of radiotherapy in Korea by treatment schedule
![]()
Go to :
DISCUSSION
In this study, we confirmed that the treatment outcomes of hypofractionated RT and conventional RT in breast cancer were not different in efficacy; there was no statistical difference in the annual recurrence rates between the two groups. Moreover, hypofrationated RT seems to be preferred to conventional RT in cancer treatment during pandemic. According to our present study, there were no statistical differences in the occurrence rates of acute side effects. Thus, we proved that hypofractionated RT is a safe and effective treatment for breast cancer. Hypofractionated RT is also a method that can reduce the economic burden on patients by reducing the total number of treatments. Furthermore, hypofractionated RT is a time-saving and convenient approach. Thus, hypofractionated RT is more likely to be actively applied to breast cancer treatment because of these advantages.
Table 5 shows the representative results of prospective randomized studies about breast hypofractionated RT. UK START B trial6 shows that breast hypofractionated RT could achieve equivalent local failure (IBTR) compared to conventional RT. Canadian trial by Whelan et al.10 and DBCG HYPO trial9 also bolstered this view. Those studies show no difference on local failure (IBTR) between hypofractionated RT group and conventional RT group. These study results also show the similar local failure rate after hypofractionated RT.
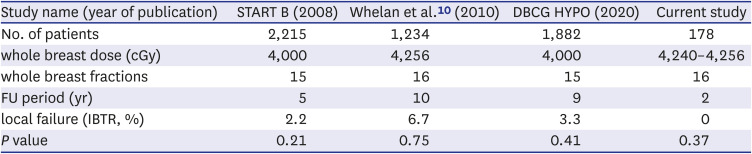
Table 5
Comparison of ipsilateral breast tumor recurrence among breast cancer hypofractionated radiotherapy trials
| Study name (year of publication) | START B (2008) | Whelan et al.10 (2010) | DBCG HYPO (2020) | Current study |
|---|---|---|---|---|
| No. of patients | 2,215 | 1,234 | 1,882 | 178 |
| whole breast dose (cGy) | 4,000 | 4,256 | 4,000 | 4,240–4,256 |
| whole breast fractions | 15 | 16 | 15 | 16 |
| FU period (yr) | 5 | 10 | 9 | 2 |
| local failure (IBTR, %) | 2.2 | 6.7 | 3.3 | 0 |
| P value | 0.21 | 0.75 | 0.41 | 0.37 |
![]()
The absence of recurrence in the hypofractionated RT group in this study could be explained by the large number of additional boost RT performed in patients (Table 1). Therefore, hypofractionated RT may have a biological dose slightly higher than that of conventional RT, which may contribute to a low rate of IBTR.
Although this study targeted patients with early breast cancer without lymph node metastasis, it is considered to be applicable in the future to advanced-stage cancer patients. Furthermore, nodal irradiation was not used in the present study. However, according to recent studies, the application of hypofractionated RT may be extended to regional lymph node-positive breast patients. According to a recent study by Wang et al.,17 hypofractionated RT to regional nodal irradiation can be safely and effectively applied even in high-risk patients with advanced-stage breast cancer. Current consensus reports in Europe have also shown a change in practice.18
The recently published FAST forward trial8 showed that ultra-hypofractionated RT of 26 Gy/5 fractions with 1-week schedule can be as safe and effective as hypofractionated RT with a 3-week schedule. It is also expected that low risk patients will receive ultra-hypofractionated RT soon. Moreover, a concomitant boost or simultaneous integrated boost technique could also be used to reduce the treatment time.1920
The limitations of this study include the relatively short follow-up period and the absence of patients who died during follow-up. Thus, a comparison of survival rates was impossible. Because our institution changed practice for breast cancer RT in 2016, the follow-up period of this study was short compared to other studies. In addition, the side effects have not been followed up in the long run. Therefore, we could not clearly assess the chronic side effects. The low recurrence rate of this cohort may be partially affected by systematic treatments, such as the administration of Trastuzumab,21 chemotherapy, and endocrine therapy.22 Furthermore, since this was a retrospective single-center study, selection bias may have occurred despite PSM correction. If long-term follow-up results are presented in the future, it will be possible to report more reliable treatment results.
In conclusion, hypofractionated RT is a very effective treatment for patients with early-stage breast cancer, even though it was a short follow-up period in this study. It is expected to be actively applied as treatment in more patients in the future due to its economic value and convenience in terms of shortening the treatment period. This study also showed that RT for patients with breast cancer evolved and developed consistently.
Go to :
 XML Download
XML Download