

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Anthropogenic volatile organic compounds (VOCs), such as formaldehyde, benzene, and xylene, are major indoor air pollutants produced that evaporate from various sources at room temperature.1 VOCs can cause irritation and allergic inflammation,2 and there is a plausible link of exposure to VOCs with the onset and exacerbation of atopic dermatitis.1 Atopic dermatitis is a chronic inflammatory skin disease that has become a global health problem because of its increasing incidence during recent decades.3 Research indicates that air pollutants have contributed to the increasing incidence of atopic dermatitis.4
However, previous studies that examined the effects of VOCs on atopic dermatitis had limitations,567891011 so this relationship remains inconclusive. In particular, these studies mainly employed air-sampling methods to estimate exposure to VOCs, therefore the effects of exposure to different environments and differences in exposure at the individual level were not under consideration. Several studies suggested possible adverse effects of exposure to indoor air pollutants and found that exposure increased the incidence or exacerbated atopic dermatitis,567 but other studies reported no direct link.8910 Authors of a systematic review concluded that more qualified and evidence-based examinations are necessary to establish a definite relationship between VOC exposure and allergic diseases.11
We monitored biomarkers of VOC exposure—urinary concentrations of VOC metabolites—a widely accepted method used to quantify exposure because it accounts for differences in route of exposure, residential environment, and personal lifestyle.2 There are virtually no population-level data on the burden of indoor contaminants based on measurements of urinary concentrations of VOC metabolites to childhood atopic dermatitis. We focused on the associations between atopic dermatitis and skin inflammations represented as SCORing Atopic Dermatitis (SCORAD) index with the urinary concentrations of 9 representative metabolites of VOCs in 7-year-old school children.
METHODS
Children from 11 elementary schools were enrolled and examined between June and July, 2016. All children were in the first grade (7–8 years old). The 408 children who agreed to physical examinations and properly completed the structured questionnaire were considered eligible. Demographic characteristics (age, sex, year of birth, height, weight), details regarding allergy, environment, birth history, and parental history were obtained using questionnaires. Body mass index (BMI) was calculated to derive BMI z-score. Among the urine provided by these participants, samples with inadequate volume or quality were excluded and 149 samples were finally prepared for metabolomics assays.
Definition of main outcomes
Children with an affirmative response of the following questions of the International Study of Asthma and Allergies in Childhood (ISAAC) were defined as atopic dermatitis: “Has your child ever had an itchy rash which was coming and going for at least six months?”. Diagnosis of asthma and allergic rhinitis were also determined by characteristic symptoms during the previous 12 months, based on the results of the ISAAC questionnaire.
Physicians who visited the schools assessed the SCORAD index of each participant by skin examinations.121314 At the time of skin examinations, physicians were not aware to the questionnaire answers. We considered subjects with SCORAD < 5 as “negative,” and those with SCORAD ≥ 5 as “positive.”15 In addition, we divided the results of SCORAD into three classes based on index values: mild (< 25), moderate (25–50), and severe (> 50).12
Measurements of urinary VOC metabolites
Personal exposures to VOCs were assessed using urine samples, a non-invasive procedure with minimal burden for children, which were collected on the same day as the skin examinations. Two of the 9 VOC metabolites (m-methyl-benzoic acid and phenylmercapturic acid) were below the limit of detection (LoD) in most samples and were not used for analyses. The 7 quantifiable urinary VOC metabolites (parent compounds) were: tt-cc-muconic acid (benzene), phenylglyoxylic acid (styrene), o-methylbenzoic acid (xylene), p-methylbenzoic acid (xylene), mandelic acid (benzene), benzylmercapturic acid (toluene), and thiazolidine-4-carboxylic acid (TZCA, formaldehyde). A simple high performance liquid chromatography method was developed for measurement of tt-cc-muconic acid, benzylmercapturic acid, aromatic carboxylic acids (phenylglyoxylic acid, o-/p-/m-methylbenzoic acid, and mandelic acid), and benzylmercapturic acid. A commercial Sep-Pak silica gel cartridge (Waters; Millipore Corp., Burlington, MA, USA) was used to determine TZCA. All mass spectra were obtained using an Agilent 6890/5973 N instrument for analyte identification. Calibration curves were established using derivatization and extraction, and the peak area of each internal standard was used for quantification.16 The urinary concentration of each VOC metabolite was expressed relative to grams of urinary creatinine (g Cr). For analysis of the relationships between VOC concentrations and atopic dermatitis, subjects were divided into two groups (high VOC and low VOC) for each compound based on the median concentration (Supplementary Table 1). Benzylmercapturic acid (LoD: 0.25 μg/g Cr) was detectable in only 29 children and tt-cc-muconic acid (LoD: 14 μg/g Cr) was only detectable in 55 children, and so subjects were divided into non-detected and detected groups for these compounds. When the association was insignificant based on analysis of low and high concentration groups, subjects were divided into quartiles for further analysis.
Specific IgE test
Skin prick tests were performed for 22 common allergens, 13 aeroallergens (house dust mites [Dermatophagoides farina, Dermatophagoides pteronyssinus], cat dander, dog dander, cockroach, birch, oak, elm, orchard grass, Japanese hop, mugwort, ragweed, and Alternaria) and 9 food allergens (cow’s milk, egg white, peanut, wheat, walnut, shrimp, apple, kiwi, celery). A mean wheal diameter greater than 3 mm was considered positive. Children with positive results to at least one allergen were considered to have allergen sensitization.
Statistics
The χ2 test was used to compare categorical variables. A generalized linear regression with a logit function that adjusted for confounding factors (sex, BMI z-score, prematurity and/or low birth weight, aeroallergen sensitization, current asthma, and current allergic rhinitis) was used to determine the associations. Associations between urinary VOC levels with the presence of atopic dermatitis, and with positive SCORAD results were analyzed based on adjusted odds ratio (aOR) and 95% confidence interval (CI). Non-parametric tests were used where appropriate. A P value below 0.05 was considered significant. Statistical analyses were performed using SPSS version 23.0 (IBM Co, Armonk, NY, USA). The strength of the effect of each urinary VOC metabolite on atopic dermatitis was ranked using the nonparametric random forest method with the package for R system version 2.8.2 (R Foundation, Vienna, Austria).
RESULTS
A total of 149 children met the study criteria, completed the physical examinations, and provided urine samples (Table 1). Eighty-eight children were boys (59.1%) and the mean age was 7.1 years. Based on the ISAAC questionnaire, the prevalence of atopic dermatitis was 30.2% (n = 45). Based on the SCORADs, 17 children (11.6%) had mild symptoms and 18 (12.2%) had moderate to severe symptoms. Seventy-two children (48.3%) were exposed to second-hand smoke, 18 (13.1%) were premature, and 8 (5.4%) had low birth weight. The skin tests (performed in 147 children) indicated that 64 children (43.5%) were sensitized to at least 1 allergen and 83 (56%) were not sensitized to any tested allergen.
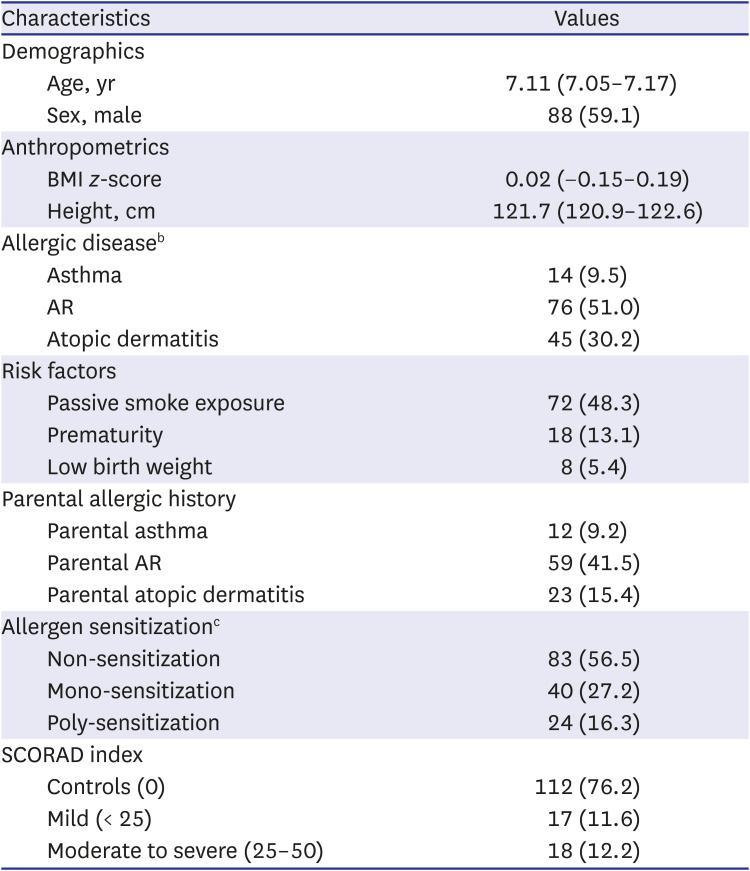
Table 1
Demographic and clinical characteristics of enrolled children (N = 149)a
Values are presented as mean (95% confidence interval), number (%), or median (interquartile range).
BMI = body mass index, AR = allergic rhinitis, SCORAD = SCORing Atopic Dermatitis.
aData were missing for asthma (n = 10), prematurity (n = 12), parental asthma (n = 18), parental AR (n = 7), allergic sensitization (n = 2), and SCORAD result (n = 2).
bCurrent allergic history (12 months) based on the International Study of Asthma and Allergies in Childhood (ISSAC).
cAllergy to 13 aeroallergens and 9 food allergens, as described in the Methods.
![]()
Relationship of atopic dermatitis and VOC concentrations
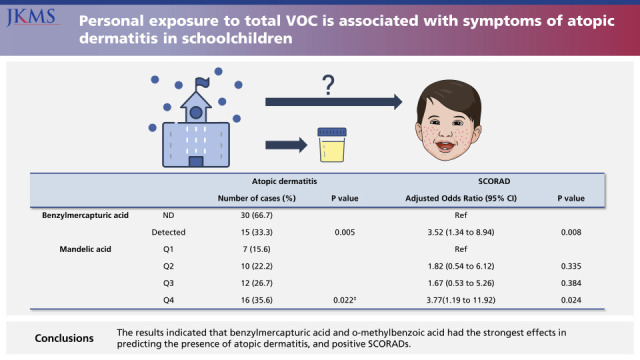
We first compared controls and children with atopic dermatitis based on ISAAC results (Table 2). The results indicated that benzylmercapturic acid was more common in children with atopic dermatitis (19.5% vs. 13.5%, P = 0.005), consistent with the results of the multivariate analysis for this compound (adjusted odds ratio [aOR], 3.52; 95% confidence interval [CI], 1.34–8.94; P = 0.008). Comparison of the first and fourth quartiles for mandelic acid indicated that atopic dermatitis was also associated with mandelic acid concentration (aOR, 3.77; 95% CI, 1.19–11.92; P = 0.024).
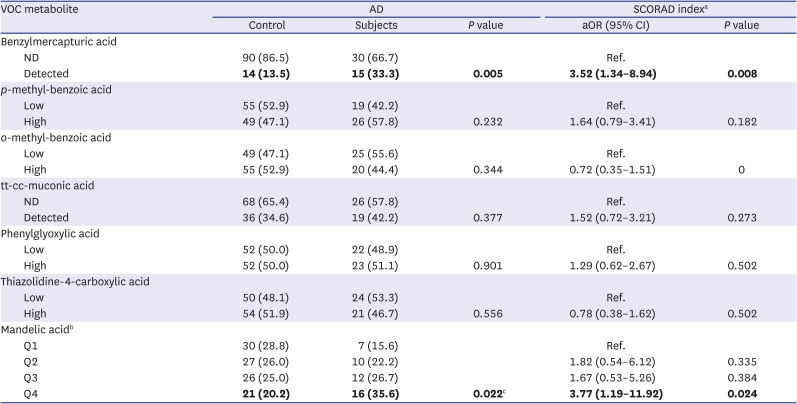
Table 2
Multivariate analysis of the association of VOC metabolites with AD based on ISAAC results (N = 149)
Values are presented as number (%). Bold values are statistically significant.
AD = atopic dermatitis, ND = not detected, SCORAD = SCORing Atopic Dermatitis, VOC = volatile organic compound, ISAAC = International Study of Asthma and Allergies in Childhood, aOR = adjusted odds ratio, CI = confidence interval.
aAdjusted for sex, BMI z-score, prematurity or/and low birth weight, allergen sensitization (no vs. yes), secondary smoking, current asthma, and current allergic rhinitis using a generalized linear regression with the logit function.
bOnly mandelic acid has shown significant linear relationships when range of concentration divided into four groups with equal intervals, therefore presented into quantiles.
c
P value for a linear relationship.
![]()
Relationship of SCORAD results and VOC concentrations
We used the same analysis to compare controls with children who had positive SCORAD results (Table 3). The results indicated that benzylmercapturic acid was more common in children with positive SCORAD results (34.3% vs. 15.2%; P = 0.007), consistent with the results of the multivariate analysis for this compound (aOR, 3.62; 95% CI, 1.41–9.29; P = 0.007). The results were similar for p-methylbenzoic acid (46.4% vs. 65.7%, P = 0.046; aOR, 2.47; 95% CI, 1.09–5.61; P = 0.03) and mandelic acid (18.8% vs. 45.7%, P = 0.015; aOR, 3.92; 95% CI, 1.30–12.00; P = 0.017). The association was similar when analysis was performed using SCORAD results stratified as mild, moderate, and severe (data not shown) or when considered as a continuous variable (Supplementary Table 2).
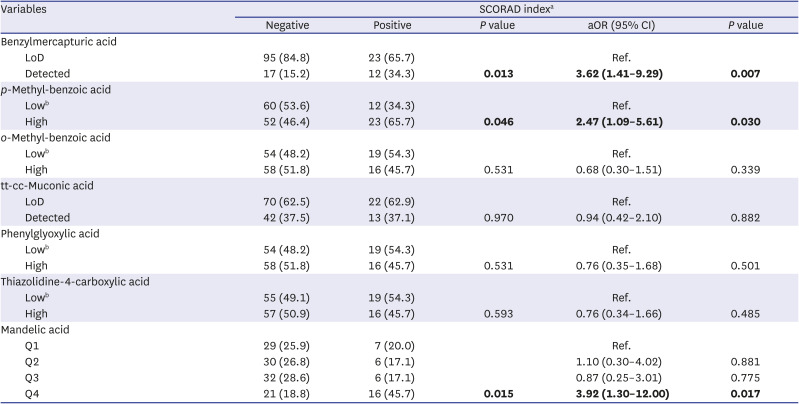
Table 3
Multivariate analysis of the association of VOC metabolites with atopic dermatitis based on SCORAD results (N = 147)a
Values are presented as number (%). Bold values are statistically significant.
LoD = limit of detection, SCORAD = SCORing Atopic Dermatitis, VOC = volatile organic compound, aOR = adjusted odds ratio, CI = confidence interval.
aχ2; Children with “negative” SCORADs vs. “positive” SCORADs (children with SCORAD = 0 was considered as “negative,” and children with SCORAD score 1 or higher as “positive” for SCORADs). Adjusted for sex, BMI z-score, prematurity or/and low birth weight, allergen sensitization (no vs. yes), secondary smoking, current asthma, and current allergic rhinitis using a generalized linear regression with the logit function.
bLow level and high level were subdivided based on median values.
![]()
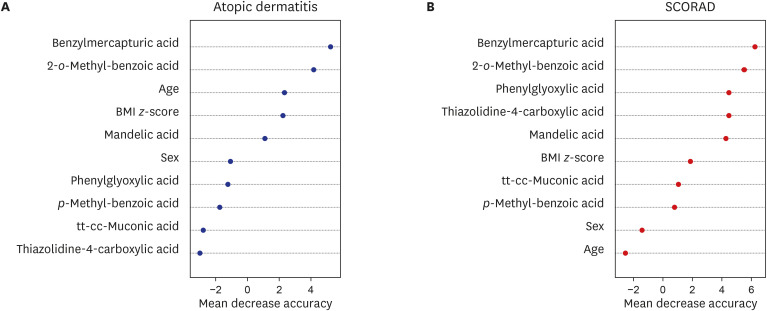
Contribution of each VOC to atopic dermatitis and SCORAD
We used a random forest analysis to evaluate the strength of the contribution of each metabolite in predicting atopic dermatitis based on ISAAC and positive SCORAD results (Fig. 1). The results indicated that benzylmercapturic acid and o-methylbenzoic acid had the strongest effects in predicting the presence of atopic dermatitis, and positive SCORADs.
DISCUSSION
The major finding of this study is that the urinary concentrations of benzylmercapturic acid (toluene metabolite), mandelic acid (benzene metabolite), and p-methylbenzoic acid (xylene metabolite) were significantly related with presence of atopic dermatitis diagnosed by ISAAC and atopic dermatitis symptoms represented as SCORAD results. To the best of our knowledge, this is the first study to identify positive associations of individual urinary levels of VOC metabolites with atopic dermatitis in children. Understanding the roles of indoor air pollutants in children is especially important because they spend most of their time indoors.1718 Thus, controlling indoor air quality by reducing the usage of products that emit VOCs, such as toluene, benzene, and xylene, might decrease the risk of atopic dermatitis in children. Importantly, we directly measured urinary VOC metabolites, and these data provide a better indication of the personal burden of VOCs than air samples. Previous environmental and validation studies documented that concentrations of these VOC metabolites and ambient concentrations are highly correlated, and accuracy values generally meet the criteria for bioanalytical method validation.1920
The burden of atopic dermatitis has increased in Korea3 and worldwide.2122 during recent decades, and several previous studies investigated the associations of exposure to indoor air pollution with atopic dermatitis.56101823 However, fewer studies have investigated the association of indoor air pollution with SCORAD results.724 Furthermore, most of these previous studies estimated VOC exposures using ambient air samples.710 Some studies reported no direct links between ambient air levels of VOCs and atopic dermatitis.1024 This may be because passive air monitoring does not consider personal variations, the chronic course of atopic dermatitis, and exposure to outdoor pollutants. An examination using individual monitoring overcomes these limitations.11 Thus, our study based on measurements of VOC metabolites provides strong support for the hypothesis that presence and symptoms of atopic dermatitis is associated with exposure to VOCs.25
Leipzig's Allergy Risk Study reported that excretions of toluene metabolites (based on urine measurements) were associated with atopic dermatitis.6 In agreement, we also found that benzylmethylmercapturic acid (a toluene metabolite) and ethyl-benzene (a mandelic acid metabolite) were significantly associated with the prevalence of atopic dermatitis and related symptoms. This is in concordance with earlier studies that measured VOCs using passive air sampling.242627 However, we found that mandelic acid appeared to be less important than toluene based on ISAAC and SCORAD results. This could be because of the low concentrations of the VOCs detected in urine samples of our findings compared with previous studies,2829 which intended to measure urinary VOC concentrations to estimate the extent of exposures, rather than a true non-association. Likewise, our random forest analysis indicated that the toluene metabolite had the strongest effect based on ISAAC and SCORAD results. Toluene is a well-known VOC, and previous studies reported its level correlated with atopic dermatitis and SCORADs.723 Previous molecular studies that investigated the association between atopic dermatitis and VOCs suggested that toluene exposure upregulated mRNA expression of thymic stromal lymphopoietin, a cytokine that plays a key role in the pathogenesis of atopic dermatitis in keratinocytes.3031 This result implies a strong association between toluene exposure and symptoms occurred in atopic dermatitis.32
The main strength of our study is that we used measurements of urinary VOC metabolites to estimate exposure to VOCs. These measurements using biomonitoring methods provide more accurate access to individual exposures and biological burdens, because children may differ in routes of exposure, environments where they spend most of their time, and individual health conditions. Previous data, which relied on measurements of VOCs in ambient air focused on occupationally exposed individuals, but ambient concentrations of air contaminants should be considered as a surrogate of true exposures. We believe that our findings using biomonitoring of VOCs hereby offer meaningful information for association with presence of atopic dermatitis and symptoms represented as and SCORAD results. In addition, physicians performed the diagnosis of atopic dermatitis using the ISAAC and scaled the severity of disease using the SCORAD index. Children with positive SCORAD index values did not concur with those diagnosed as atopic dermatitis based on ISAAC questionnaires. This might possibly because the diagnosis depended on parents’ answers. For this reason, we considered that notification of clinical signs/symptoms of atopic dermatitis by separate analyses performed by physicians has its own significance.
However, our measurements of urinary metabolites of VOCs do not indicate actual exposures to these compounds. A further longitudinal study of this topic is thus necessary. In addition, our results should be interpreted with caution because the sample size was small and limited to children of a single city in Korea. Selection or participation bias may exist as subjects that agreed to participation and properly completed the questionnaires were enrolled, and parents with specific health concerns were more likely to participate. Our study does not include measurement of VOC exposure before and at different phases of atopic dermatitis’s occurrence due to the nature of the cross-sectional study design. Causal relationships might be established through further prospective and controlled studies. Furthermore, the small sample size and undetectable levels of urinary VOC metabolites imposes limitations to our study, and large-scale data sets or reference levels for VOC metabolites might be helpful in establishing validated safety levels in children.
In summary, we documented an association between exposure to VOCs and atopic dermatitis in children based on measurements of their urinary levels of VOC metabolites. Our results imply that the urinary levels of VOC metabolites in children reflect exposure to these compounds and the incidence of atopic dermatitis. Our findings have shown associations between increased urinary levels of the mandelic acid and benzylmercapturic acid (metabolites of ethylbenzene and toluene) with presence and symptoms of atopic dermatitis in children. These findings elucidate that specific VOCs might be attributable to atopic dermatitis.
 XML Download
XML Download