

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Patients with hypertrophic cardiomyopathy (HCM) present with various symptoms, including exertional shortness of breath, chest pain, syncope, or pre-syncope.1 Even with preserved left ventricular (LV) systolic function, patients with HCM often develop dyspnea or fatigue, and the majority of these patients have exercise intolerance.2 In such cases, cardiopulmonary exercise testing (CPET) is an indicator of actual oxygen consumption and is a reliable method for objectively evaluating exercise capacity.3
Peak oxygen consumption (peak VO2) has been reported to be a useful marker of functional capacity in HCM.2 Exercise stress test is also an important and useful tool for evaluating symptoms and monitoring response to therapy in patients with HCM,4 and it can aid in risk stratification for future events, as previously described.567 Furthermore, evaluating exercise capacity could be a useful and simple way to assess hemodynamic status and clinical outcomes without the need for complex modalities in patients with HCM.18 Previous studies have shown several parameters that are associated with exercise intolerance in patients with HCM.89101112131415 However, few studies have conducted a comprehensive analysis of several parameters related to CPET, which can reliably demonstrate patients’ functional capacity.
The aim of this study was to determine exercise capacity in patients with HCM via CPET and to evaluate the determinants of exercise capacity in clinical, laboratory, and imaging studies.
Go to : 
METHODS
Study population and clinical characteristics
The study was performed as a cross-sectional study using data from the observational HCM registry of the Samsung Heart Vascular Stroke Institute, Seoul, Korea, which consecutively enrolled 591 patients who were diagnosed with HCM and underwent cardiac magnetic resonance imaging (CMR) between 2008 and 2015. The study population comprised 294 patients with HCM who were able to perform CPET (n = 295) and presented with normal LV systolic function (ejection fraction ≥ 50%). CPET and CMR were performed according to a standard protocol at baseline.
Echocardiographic criteria for inclusion in the HCM registry were as follows: 1) posterior wall thickness ≥ 1.3, in the absence of any underlying clinical condition that could lead to LV hypertrophy (i.e., longstanding systemic hypertension, aortic or subaortic stenosis, and clinical evidence of metabolic infiltrative disease or inflammatory disease), an end-diastolic LV wall thickness of ≥ 15 mm at any site, or LV septal thickness; 2) posterior wall thickness ≥ 1.5, in patients with systemic hypertension or end-diastolic LV septal thickness; or 3) LV hypertrophy confined predominantly to the LV apex (only the apical four segments and the apical cap according to the 17-segment guidelines of the American Society of Echocardiography) with a maximal apical wall thickness of ≥ 14 mm or a ratio of maximal apical to posterior wall thickness ≥ 1.3 at end-diastole.16 subjects with uncontrolled hypertension, uncontrolled ventricular arrhythmias, severe valvular diseases, other concomitant systemic diseases (including malignancy), and subjects who had poor echocardiographic windows for analysis were excluded.1171819
Clinical and laboratory evaluation
All clinical characteristics were obtained by reviewing the medical records. Symptoms were recorded, such as dyspnea (New York Heart Association [NYHA] functional classification) or chest pain. History of syncope or sudden cardiac death was recorded. Other past medical histories, which described the presence of hypertension, diabetes mellitus, or atrial fibrillation and information on family history of sudden cardiac death and HCM, were also reviewed. The family history was defined as history in first-degree relatives. We also obtained the value of the biomarker N-terminal pro-hormone of brain natriuretic peptide (NT-proBNP) at the time of CPET; 24-hour Holter monitoring was performed for all subjects.
Echocardiographic study and CPET
Conventional two-dimensional echocardiography was performed, and echocardiographic parameters were obtained according to guidelines. LV end-diastolic and end-systolic volumes were measured from apical two- and four-chamber views, and the ejection fraction was calculated using the biplane modified Simpson’s method. LV mass was calculated using the formula proposed by Devereux et al. and corrected by body surface area to derive the LV mass index.20 The left ventricular outflow tract (LVOT) was scanned with continuous Doppler to measure the maximal velocity and estimated pressure gradient in apical three- or five-chamber views. LVOT obstruction was defined as a pressure gradient ≥ 30 mmHg at rest.911192122
Left atrial volume was measured using the biplane modified Simpson’s method and adjusted for body surface area (left atrium volume index, LAVI). Early diastolic mitral annular velocity on the septal side (e) and peak early diastolic transmitral flow velocity (E) were measured, and E/e′ was calculated using these parameters.23
CPET was performed using the symptom-limited treadmill exercise test with respiratory gas exchange analysis in all patients using the Bruce protocol.242526 Twelve-lead electrocardiography was performed using conventional chest lead positioning before exercise and at the conclusion of each stage and after stress. Blood pressure (BP) was recorded every 2 minutes. Peak VO2 was measured using a Medical Graphics metabolic cart (St. Paul, MN, USA). Peak VO2 was the highest averaged 30-second VO2 during exercise and was expressed as absolute or normalized peak VO2 (percentage of age, sex, and weight predicted). Exercise was terminated if there was marked dyspnea, fatigue, chest discomfort, > 2-mm ST depression, or after completion of 15 minutes of the protocol (15.6 metabolic equivalents). Additionally, abnormal hemodynamic response to exercise was defined as follows: 1) blunted BP response, < 20 mmHg increase in systolic BP; or 2) hypotensive response, > 20 mmHg decrease in systolic BP from the baseline BP, or an initial increase in systolic BP followed by a decrease in systolic BP > 20 mmHg.2728
CMR acquisition and analysis
CMR was performed using a 1.5 T system (Magnetom Avanto, Syngo MR B15 version; Siemens Medical Solutions, Erlangen, Germany) with a 32-channel phased-array receiver coil during repeated breath-holding. The CMR protocol consisted of cine, T2W, first-pass perfusion, and late gadolinium enhancement (LGE) imaging. Cine imaging was performed with balanced steady-state free precession sequences along the long and short axes from the cardiac apex to the base of the LV. Cine images of steady-state free precession were obtained with adjacent short-axis slices (slice thickness, 6 mm; gap, 4 mm) to quantify LV function and volume.
Standard LGE imaging was performed as intravenously administered of gadobutrol (0.15 mmol/kg Gadovist; Bayer Healthcare, Berlin, Germany). LGE images were acquired from long-axial, short-axial, and apical 4-chamber views. These images used a multi-shot turbo field echo breath-hold sequence with a phase-sensitive inversion recovery method. The inversion time was usually 280–360 msec. LGE images were estimated 10 minutes after gadolinium administration. The field of view was 35 × 35 cm, and the field of matrix was 256 × 256 cm.29 LGE was regarded present when the signal intensity of the index myocardial segment was greater than 6 standard deviations above the remote normal myocardial signal. LGE volume was calculated by total summation of LGE coverage in all short-axis slices, which was demonstrated as the volumetric proportion of the total LV myocardium (%LV). CMR scans were visually interpreted by two experienced investigators who were blinded to the clinical and laboratory data.
Statistical analysis
Continuous variables were compared using Student’s t-test or the Wilcoxon rank-sum test where applicable and are presented as mean ± standard deviation or median with interquartile range (IQR). Categorical data were analyzed using the Fisher exact test or χ2 test, as appropriate.
We performed simple and multiple linear regression analyses to assess the relationship of relevant parameters with exercise capacity as a continuous variable. Simple correlations were analyzed using Spearman’s correlation. All parameters were analyzed via multiple linear regression analysis (step 1) after univariable analysis. Parameters from the multiple regression analyses (P < 0.2) or clinically meaningful parameters were then entered into the final multiple linear regression model (step 2). These variables were calculated using a stepwise multiple linear regression analysis and included age, sex, NT-proBNP, and E/e′ ratio.
All analyses were conducted using R for Windows (version 3.3.2; R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was set at P < 0.05.
Ethics statement
This study was approved by the Institutional Review Board of Samsung Medical Center, and the requirement for informed consent was waived (IRB No. 2015-12-136).
Go to :
RESULTS
Baseline clinical characteristics
The baseline clinical characteristics of the subjects are shown in Table 1. There were 252 men (85.7%), and the median age of the population was 53 years (IQR, 46–61). Nineteen (6.5%) and 16 (5.4%) patients had a family history of HCM and a history of syncope, respectively. Fifty-four subjects (18.7%) complained of NYHA class ≥ II dyspnea. The mean NT-proBNP level was 542.64 ± 629.61 pg/mL.
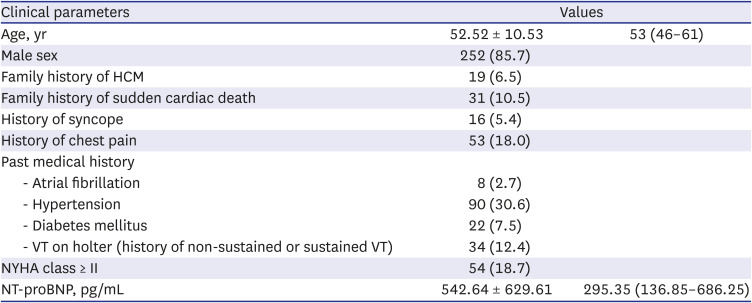
Table 1
Clinical characteristics of the study population
Data are presented are number of patients (percent) and average ± standard deviation or median (interquartile range).
HCM = hypertrophic cardiomyopathy, VT = ventricular tachycardia, NYHA = New York Heart Association, NT-proBNP = N-terminal pro-hormone of brain natriuretic peptide.
![]()
CPET and CMR parameters
Echocardiographic, CPET, and CMR parameters are shown in Table 2. The mean maximum LV wall thickness was 17.47 ± 4.07 mm. Mean LAVI was 41.87 ± 16.43 mL/m2 and the mean E/e′ ratio was 11.63 ± 4.34. LVOT obstructed was noted in 19 patients (16.7%).
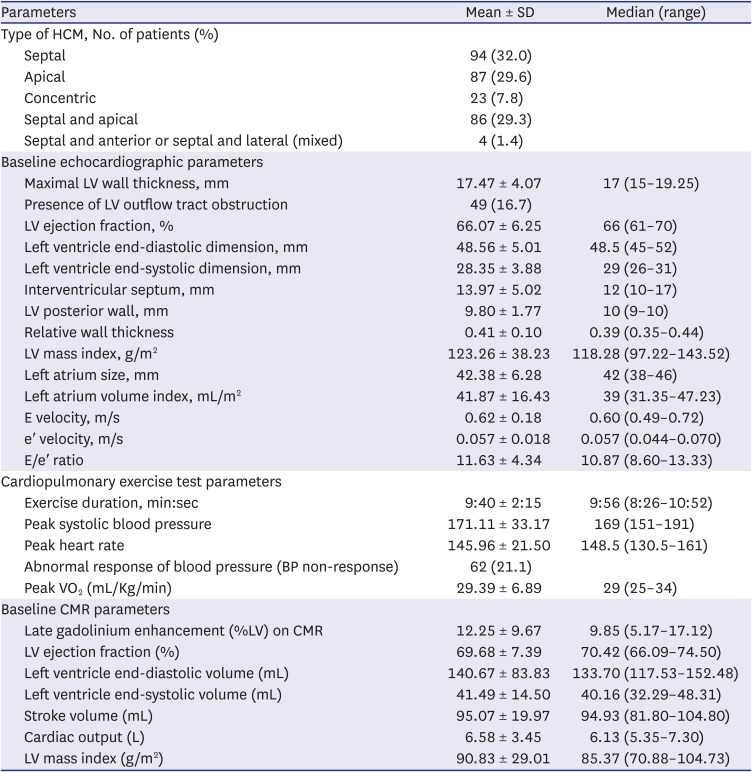
Table 2
The parameters of echocardiography, cardiopulmonary exercise test, and cardiac magnetic resonance on study population
Data are presented are number of patients (percent) and average ± standard deviation or median (interquartile range).
SD = standard deviation, HCM = hypertrophic cardiomyopathy, LV = left ventricular, BP = blood pressure, peak VO2 = peak oxygen consumption, CMR = cardiac magnetic resonance.
![]()
Sixty-two (21.1%) patients had abnormal hemodynamic responses on CPET. Moreover, the median value of peak VO2 as a representation of exercise tolerance was 29.0 mL/kg/min (IQR, 25.0–34.0) in the study population.
Mean amount of LGE on CMR was 12.25 ± 9.67%LV. LV ejection fraction and LV mass index on CMR were 69.68 ± 7.39% and 90.83 ± 29.01 g/m2, respectively.
Univariate and multivariate analysis regarding exercise capacity
The association of various parameters with peak VO2 in our study group is shown in Table 3. In univariate analysis with simple linear regression, several parameters were found to be associated with exercise tolerance, including age, sex, family history of HCM, history of syncope, NYHA class ≥ II, and increased NT-proBNP, echocardiographic parameters (LAVI, E/e′, maximal LV wall thickness, and the presence of LVOT obstruction), abnormal hemodynamic response on CPET, and various CMR parameters (LGE, LV ejection fraction, and LV mass index). Multiple linear regression analysis (step 1) revealed significant parameters, including age, female sex, NT-proBNP, and E/e′ ratio. The results of the stepwise multiple linear regression analysis (step 2) are shown in Table 4. Age (estimated β = −0.140, P < 0.001), female sex (β = −5.362, P < 0.001), NT-proBNP (β = −1.256, P < 0.001), and E/e′ ratio on echocardiography (β = −0.209, P = 0.019) were independent determinants of exercise capacity.
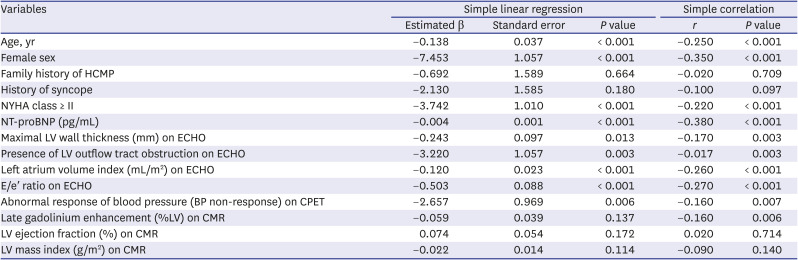
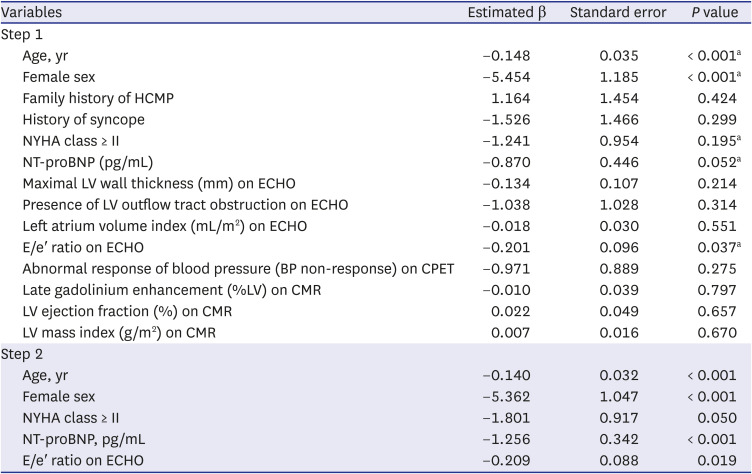
Table 3
Simple linear regression analysis and simple correlation of exercise capacity
Simple correlation was analyzed by Spearman correlation method.
HCMP = hypertrophic cardiomyopathy, NYHA = New York Heart Association, NT-proBNP = N-terminal pro-hormone of brain natriuretic peptide, LV = left ventricular, ECHO = echocardiography, CPET = cardiopulmonary exercise test, BP = blood pressure, CMR = cardiac magnetic resonance.
![]()
Table 4
Multiple linear regression analysis of variables for the correlation of exercise capacity (excluding 2 subjects as outliers)
HCMP = hypertrophic cardiomyopathy, NYHA = New York Heart Association, NT-proBNP = N-terminal pro-hormone of brain natriuretic peptide, LV = left ventricular, ECHO = echocardiography, CPET = cardiopulmonary exercise test, CMR = cardiac magnetic resonance.
aThe stepwise multivariable linear regression analysis was performed with including the indicated parameters, and predictive MODEL was established as adjusting with parameters such as age, sex, NYHA class ≥ II, NT-proBNP, E/e′ ratio.
![]()
Go to :
DISCUSSION
The principal finding of our study was that, on multivariate analysis, clinical variables (age, female sex), biomarker (NT-proBNP) elevation, and increased LV filling pressure (E/e′ ratio) were independent determinants of exercise capacity in patients with HCM. Among them, the significance of the E/e′ ratio is an important result in that it can be used very simply and usefully when following-up these patients in the real clinical field.
Parameters of LV diastolic dysfunction, especially E/e′, provide valuable information for determining exercise capacity in patients with heart failure symptoms.3031 Many studies have shown that patients with HCM have a spectrum of diastolic abnormalities, determined invasively or non-invasively, including increased LAVI, LV end-diastolic pressure (correlated with E/e′), and increased myocardial stiffness. Our study confirms that increased LV filling pressure is indeed related to decreased exercise capacity in relatively healthy HCM patients, regardless of the grade of myocardial fibrosis or presence of other prognostic indicators for hard events such as sudden cardiac death.
In previous studies, NT-proBNP level was associated with oxygen consumption in patients with HCM and was more notably influenced by functional impairment than by other conventional markers of disease severity. In accordance with the prior studies, we also found that elevated NT-proBNP level was also a significant determinate for exercise capacity in HCM. Many previous studies have reported that elevated NT-proBNP level shows correlation with LV filling pressure as E/e′ ratio on echocardiography.3233 Both parameters may serve as important indicators of LV functional reserve that affects exercise capacity in patients with HCM. Meanwhile, the association between female sex and reduced exercise capacity, as noted in our study, may possibly explain the relationship between the female sex and poor prognosis in previous studies.343536
Hemodynamic compromise reflected by biomarker elevation and increased LV filling pressure could play a crucial role in exercise capacity in clinical practice and seems closely associated with a poor prognosis. For deciding management plans for patients with HCM, risk stratification for worse clinical outcomes and evaluation of subjective symptoms are both required. However, in real-world settings, patients may present with heart failure symptoms but also can be subjectively asymptomatic regardless of LV systolic function. Accordingly, self-reported subjective symptoms may be insufficient for critical decision making. Physiological exercise stress testing is recommended for patients with HCM because it provides customized exercise capacity and information related to exertional symptoms of heart failure,3738 allowing the exclusion of invasive procedures or substances such as contrast agents. We recommend that when exercise testing is performed, CPET should be performed with measurement of peak oxygen consumption as in our study in most patients with HCM to evaluate the patients’ exercise capacity objectively. However, in patients who are unable to undertake such exercise testing, surrogate markers such as parameters presented in our study may be useful for estimating the current status of patients with HCM. Furthermore, NT-proBNP and E/e′ ratio could be used as practical follow-up indicators to determine the treatment plan and medication use and to establish important policies for the treatment of HCM.
The mechanism responsible for diastolic dysfunction and elevated biomarkers might be multifactorial; the pathological changes in myocytes, such as hypertrophy and disarray, could increase passive LV stiffness. Fibrosis measured by LGE has been found to be associated with a poor clinical prognosis.394041 Furthermore, abnormal diastolic parameters may be associated with the progression of myocardial fibrosis.42434445 Indeed, according to many previous studies, the amount of LGE on CMR and exercise capacity are both independent factors related to outcomes. Accordingly, we did anticipate that LGE and exercise capacity may show clinical correlation, which turned out to be not true in our study. However, in regard to hard outcomes, both parameters are independent factors showing independent associations. Furthermore, the prognostic value of LGE on CMR has been mostly reported to be associated with sudden cardiac death or ventricular arrhythmia rather than death from aggravation of heart failure, which may be more associated with functional capacity. Therefore, these parameters do not necessarily have to be related to each other, as there may be many confounding variables that exist between the parameters such as the pattern and shape of myocardial fibrosis represented by LGE. Additionally, as the patients enrolled in this study had various types of HCM, the amount of LGE may have had little effect on exercise capacity. This is because global changes that occurred in the LV—such as increase in LV filling pressure or diastolic dysfunction - rather than focal fibrosis should play larger roles in terms of exercise capacity.
This was a single-center cross-sectional study performed in a tertiary hospital. We only included patients who were able to exercise and had preserved LV systolic function, and we used an indirect outcome parameter to assess exercise capacity.
In our study, we could not conduct statistical prediction and assess the association of our parameters with clinical outcome. Although long-term clinical outcome is most important in clinical research, the purpose of our study was to identify parameters that were useful in the clinical field to predict the condition of HCM patients. We considered that exercise capacity would be helpful to predict and understand the overall condition and long-term course of HCM patients in the real-world clinical field. Additional studies should be performed for our parameters to be identified as factors that can predict the clinical composite outcome in HCM patients.
It is still controversial whether LV diastolic parameters at rest are major determinants of exercise tolerance in patients with HCM, and the true mechanism could still not be verified. Additionally, while we adjusted for many known determinants of exercise capacity, myocardial fibrosis assessed on CMR and the presence of LVOT obstruction did not have sufficient predictive ability. In our study, we only showed a simple correlation between exercise capacity and myocardial fibrosis and the presence of LVOT obstruction.
In patients with HCM and preserved LV systolic function, hemodynamic changes explained by biomarker (NT-proBNP) elevation and increased filling pressure (E/e′ ratio) and other clinical factors (age and female sex) were independent determinants of reduced exercise capacity, and they should be carefully considered while managing this patient population. Further studies are needed to determine the prognostic value of peak oxygen consumption rate for predicting the risk of major cardiovascular events such as sudden cardiac death.
Go to :
 XML Download
XML Download