

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Compared to deceased-donor liver transplantation (DDLT), duct-to-duct (DD) biliary anastomosis is narrower and more complex in living-donor liver transplantation (LDLT). Because of that, post-anastomotic bile duct in LDLT is frequently angulated and deformed [1234]. In particular, when a right-lobe graft is attempted using single DD biliary anastomosis, there is a high risk of biliary stricture in the future if the size of a graft bile duct is smaller than 4 mm. Therefore, DD biliary anastomosis is considered to have an inherent deficiency that cannot be overcome with current surgical techniques, and Roux-en-Y hepaticojejunostomy is recommended as the preferred method in this situation [5]. Biliary stricture in LDLT recipients caused by such problems is a critical issue because it can significantly affect surgical outcomes and quality of life, and in severe cases can cause graft loss and mortality [67]. Biliary strictures occur more frequently in recipients with LDLT than in recipients with DDLT [68910].
To prevent postoperative anastomotic stricture, anastomosis by inserting a drain tube is sometimes performed. However, the current drain tubes are not naturally and easily removed. A drain tube used at the pancreaticojejunostomy anastomotic site is being used in anticipation of the effect of natural migration due to the pancreatic juice flow [1112131415]. However, it cannot be used for DD biliary anastomosis because drain tubes never migrate spontaneously and if a very thin drain tube is inserted, a critical problem occurs in the biliary drainage.
In previous reports, the use of biodegradable stents (BS) in animal models for biliary reconstruction led to good mechanical support properties and biocompatibility [1617181920]. Also, BS could serve as carriers for the controlled release of drugs, therefore playing the role of local drug treatment for the prevention of fibrosis at the anastomotic site [21]. However, there is a chance of stent or tube fracture, which can occur at any point during the biodegradation process. This is a critical point for the clinical application of BS. Thus, to be used in DD biliary anastomosis, the BS must be made as thin as possible and the radial force must be maintained for a certain period of time. In addition, after maintaining the original stent shape for the desired time, the degradation process must occur quickly, and the BS must totally disappear so that it does not affect bile flow.
Our previous study reported that the maintenance duration of BS can be adjusted by using different types of wires and sheath-core techniques [22]. In one of our BS prototypes with a polydioxanone (PDO)/magnesium (Mg) sheath-core BS, morphological changes occurred at 6 weeks, and the BS were totally degraded at 8 weeks. Therefore, we thought that if the overall thickness of the BS was made as thin as possible, it could be used to prevent biliary stricture and fibrosis after DD biliary anastomosis.
The aim of this animal study was to assess the biocompatibility and usefulness of novel BS and evaluate their preventive effect on biliary stricture and fibrosis after DD biliary anastomosis.
METHODS
Ethical statement
The animal study was performed in the animal center of the National Center of Efficacy Evaluation for the Development of Health Products Targeting Digestive Disorders (NCEED).
All stages of this animal experiment have been approved by the Institutional Animal Care Committee of KNOTUS Co., Ltd in Incheon, Korea (KNOTUS IACUC No. 20-KE-530). All experimental procedures were conducted in accordance with the guidelines of the ethics committee and the regulations in the manuscript. This study was carried out in compliance with the ARRIVE (Animal Research: Reporting of In Vivo Experiments) guidelines.
Fabrication of sheath-core monofilament and creation of prototype biodegradable stents
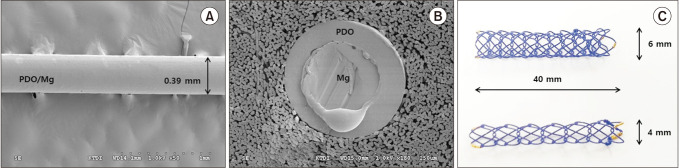
The PDO/Mg sheath-core monofilament was fabricated using a previously reported technique [22]. PDO as an outer sheath was coated onto an Mg wire by a melt-coating method. The thickness of the PDO polymer coated onto the Mg wire was controlled by adjusting the melting flow of the extruder and metering pumps. Since the degradation time of Mg is much shorter than that of PDO, the Mg core filament can degrade quickly after PDO degradation (Supplementary Fig. 1). The process of fabrication was adjusted and performed several times to find the optimal conditions so that there was no damage to the filament. The scanning electron microscopy image of the PDO/Mg sheath-core monofilament showed a smooth surface and uniform thickness without pores or cracks (Fig. 1A, B).
With these filaments, the specific prototype BS was made using the cross-and-hook knitting handmade method (Fig. 1C). The knitting interval was changed to make different diameter prototype BS. For use in DD biliary anastomosis, the diameter of the prototype BS was determined to be 4 mm and 6 mm, and the length was 50 mm. Two gold markers were attached at each end to evaluate the stent status under fluoroscopic examination. The radial force represented the average of 5 stents per type (mean ± standard deviation) measured at 37℃ (4-mm prototype BS, 0.829 ± 0.052 gram force [g·f] and 6-mm prototype BS, 0.543 ± 0.069 g·f).
In vivo animal study
Ten mini-pigs (Sus scrofa; mean age, 10 months; mean bodyweight, 68.8 kg) were used. The swine were evenly allocated to the control group (n = 5) and or the stent group (n = 5). The swine were fasted overnight before surgery but water was given ad libitum. The bodyweight of the swine was measured before surgery and then weekly until euthanization. Preanesthesia sedation was conducted, consisting of an intramuscular injection of atropine sulfate (0.04 mg/kg), xylazine (2 mg/kg), and tiletamine-zolazepam (5 mg/kg) under the supervision of a veterinarian. Then, the swine were intubated and general anesthesia was achieved using 0.5%–2% isoflurane through an endotracheal tube with 70% nitrous oxide and 30% oxygen provided by a ventilator. The swine were then placed in a supine position on the operating table. During the induction of anesthesia before surgery, the swine received cefazolin (Cefozol, Koruspharm, Chuncheon, Korea) of 22 mg/kg, intravenously (IV).
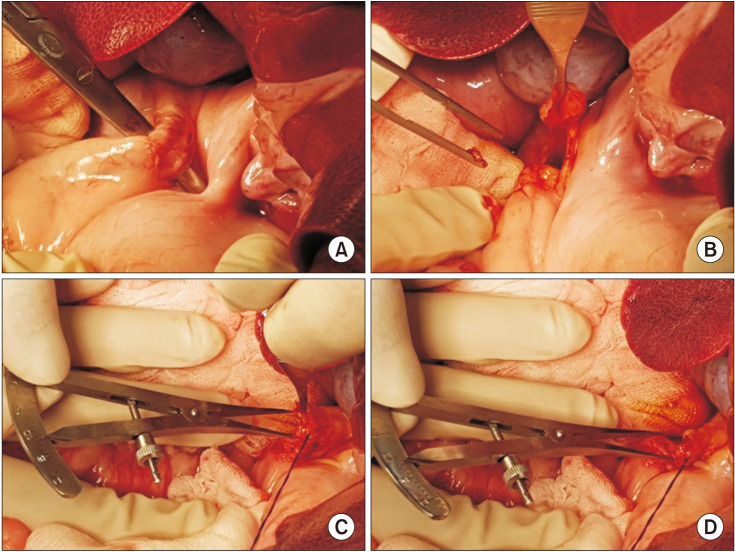
After performing midline laparotomy, the common bile duct (CBD) was isolated and divided transversely using Metzenbaum scissors. The inner luminal diameter and outer diameters of the transected CBD were measured using calipers (Fig. 2). In the control group, DD biliary anastomosis was done with continuous sutures for the posterior wall and interrupted sutures for the anterior wall using 6–0 polypropylene monofilaments (Prolene, Ethicone, Inc., Somerville, NJ, USA) (Fig. 3A, B). In the stent group, biliary anastomosis was made in the same manner. Once the posterior wall suture was completed, a 4-mm or 6-mm PDO/Mg sheath-core BS was inserted according to the width of the bile duct and positioned centrally at the transected CBD. Then, anterior wall interrupted suturing was performed (Fig. 3C, D). In all swine, cholecystectomy was performed to avoid any gallbladder complications due to the disturbance of biliary drainage after biliary anastomosis (Fig. 4). After checking for and confirming the absence of adverse events, such as anastomotic bile leakage or abdominal hemorrhage, a drainage tube was placed around the anastomosis site. The abdominal fascia was closed using 1–0 polyglactin sutures (Vicryl, Ethicone, Inc.) and the skin was approximated with a skin stapler. To reduce the influence of confounding factors, all the surgical procedures were performed by 1 hepatobiliary surgeon (SHC) using the same technique.
The swine received cefazolin (Cefozol) of 22 mg/kg IV, twice per day for 3 days to prevent intraabdominal infections and famotidine (Gaster, Dong-A ST, Seoul, Korea) of 0.5 mg/kg IV, twice per day for 3 days to prevent gastroduodenal ulcers. The swine were followed by repeated fluoroscopic examinations to confirm the status of the BS and by liver chemistry analysis for 8 weeks. They were fed standard pig chow and allowed free access to water and free movement in their pens. At the end of the follow-up time at 8 weeks, a laparotomy was performed under general anesthesia, and the CBD, a segment of the liver at the hilar area, and duodenum were extracted. Biliary duct inflammation, fibrosis, and stricture formation, especially at the DD biliary anastomosis area were evaluated histologically. The animals were then euthanized by exsanguinations.
A serious adverse event was defined as an event that led to death or serious deterioration in health (life-threatening illness or injury; permanent impairment of bodily structure or function; or fetal death, distress, or abnormality). Other adverse event measurements included operation-related complications, bleeding, perforation, cholangitis, and biliary obstruction.
Histopathologic examination
A gross examination of the CBD specimens was performed to identify any adverse events and measure the CBD circumference. Semiquantitative histologic examination of the formalin-fixed, paraffin-embedded CBD specimens was performed with H&Eand Masson’s trichrome stain and examined under light microscopy by an experienced pathologist (GK). Inflammatory reactions of the mucosa, the degree of submucosal fibrosis, and the quality of the fibrotic process were all analyzed.
Statistical analysis
The median and range were used to summarize the data for the continuous variables. The differences between the groups were analyzed using the Mann-Whitney U-test. A P-value of <0.05 was considered statistically significant. Statistical analysis was performed with IBM SPSS Statistics ver. 21.0.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Procedural and short-term outcomes
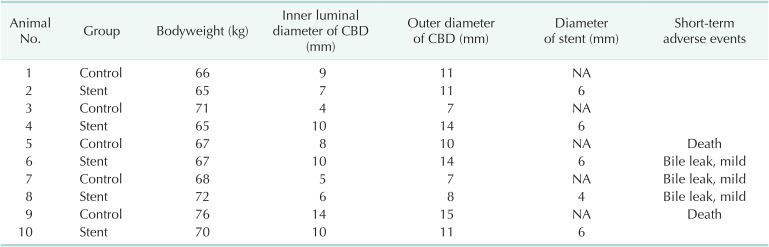
There was no major difficulty in the surgical procedures in a total of 10 animals, but mild bile leakage was observed in 3 swine (animals No. 6, 7, and 8), and the operation was completed after inserting a Jackson-Pratt drain catheter (Table 1). None of them had any special problems after surgery.
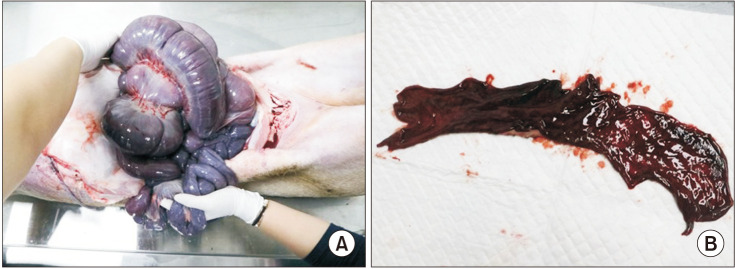
On the first day of follow-up, animal 5 swine died. At autopsy, ascites in the peritoneum was accompanied by major bleeding in the gastrointestinal tract (Fig. 5). The gastric mucosa and intestinal mucosa turned dark red. It was confirmed that the swine died due to gastric bleeding and intestinal ischemia. On the third day of follow-up, animal 9 swine also died. At autopsy, the same findings were observed as in animal 5. As the liver function test was not increased in either animal and the anastomosis area was not damaged, it was determined that the cause of death was stress-induced intestinal bleeding and hypovolemic shock, without biliary complications. No specific clinical symptoms, abnormal laboratory findings or adverse events were observed during the follow-up period in the other 8 swine.
Biodegradation of the inserted BS
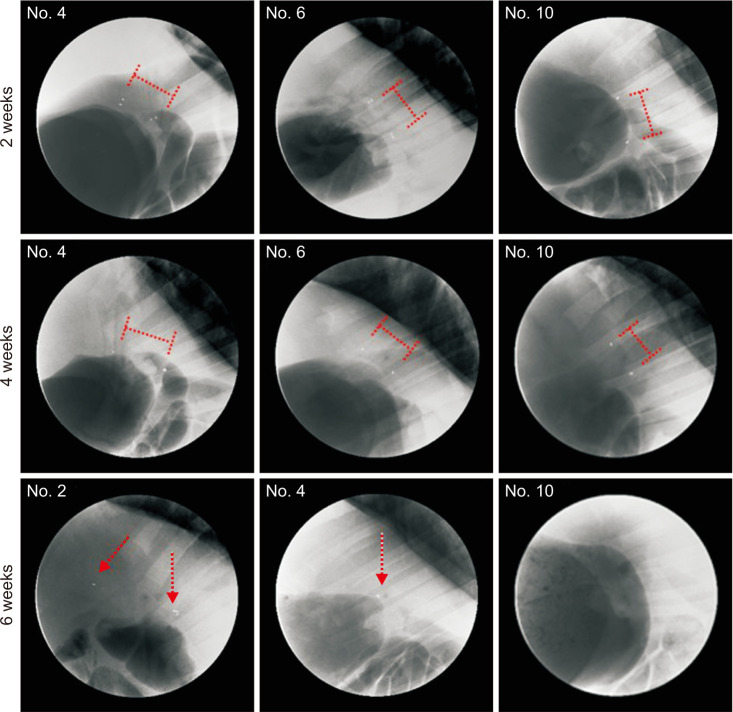
The biodegradation status of the inserted BS in the swine was checked by fluoroscopic examination (Fig. 6). The BS were observed without deformity up to 4 weeks in all swine. Then, all BS were degraded and deformed at 6 weeks and were not observed at 8 weeks.
Histologic examination results
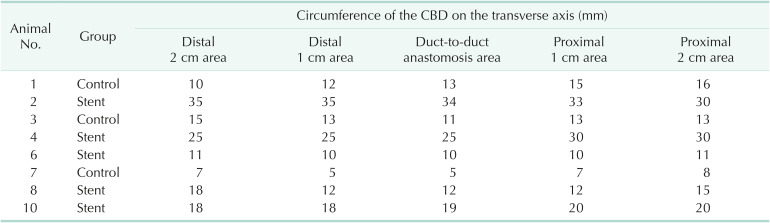
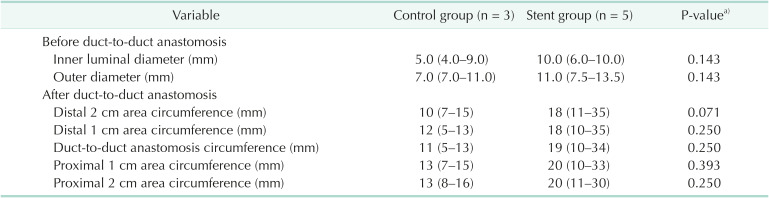
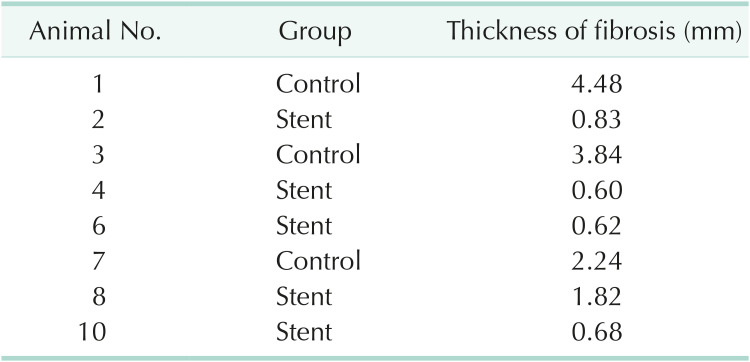
The inner luminal diameter and outer diameter of CBD measured before the creation of the DD biliary anastomosis were similar in the control group and the stent group (Table 1). Histopathologic examination was performed on the CBD specimens obtained from 8 swine (Fig. 7A). The circumference of the CBD on the transverse axis was measured centered on the DD anastomosis area, and the average values were relatively narrower in the control swine (Table 2). However, there was no statistical difference due to the limited number of specimens in each group (Table 3). According to the microscopic examination (Fig. 7B), Masson’s trichrome staining revealed that fibrosis of the DD anastomosis area was more marked in the control groups than in the stent group (median [range] of 3.84 mm [2.24–4.48 mm] vs. 0.68 mm [0.60–1.82 mm], respectively; P < 0.05) (Tables 4, 5).
DISCUSSION
We developed a novel biliary BS and conducted an animal feasibility study to evaluate the preventive effect of the BS on biliary stricture after DD biliary anastomosis. This study revealed that the maintenance duration of the original shape of the PDO/Mg sheath-core BS could be adequately adjusted for the prevention of anastomosis-related stricture and fibrosis. The PDO/Mg sheath-core BS, in which the wire consisted of a double-structure of different materials with different degradation times, could remain intact for an adequate time before abruptly breaking and biodegrading. Because of the good wire-thinning process, the use of these BS could prevent biliary obstruction, and the BS can be safely and quickly degraded from the bile duct. Also, using the cross-and-hook knitting handmade method, a relatively narrow diameter self-expandable BS with an adequate radial force could be applied to DD biliary anastomosis. We think that a stent with a diameter of 4 mm or 6 mm can be applicable for LDLT.
Before starting this study, we thought about the optimal BS maintenance period for the prevention of anastomosis-related stricture. The optimal duration of stent placement in DD biliary anastomosis is not known. In general, it is expected that if the indwelling period is less than one month, it will be shorter than the period in which anastomosis-related fibrosis is initiated and terminated, and if it is too long, stent-related adverse events in the biliary tract will occur. Some authors mentioned that a stent should not be used in biliary anastomosis because it may promote fibrosis of the anastomosis due to long-term irritation of the ductal mucosa [2324]. In addition, if a stent fracture occurs during the indwelling period and is not degraded quickly, fracture-related adverse events will occur [22].
To solve these technical problems, we used a sheath-core technique in which different biodegradable materials were inserted into the center of biodegradable wires (Fig. 1, Supplementary Fig. 1) and reported the results of a previous experimental study [22]. Using this novel method, Mg with high elasticity and short degradation time was inserted into the center of an outer PDO polymer. Because the degradation times of the 2 materials differed, it was possible to control the phenomena caused by biodegradation. This could be maintained for a certain period of time, and then the outer polymer could degrade with a stent fracture, and at the same time, the exposed Mg core could degrade very quickly.
To use BS in DD biliary anastomosis, a thin BS with an adequate radial force is required. Initial animal studies were carried out in the form of a tube to make the thickness of the BS as thin as possible, and it was confirmed that it was completely degraded within 6 months [161718]. Then, a clinical trial using this tube-type BS in DDLT patients was conducted, and its potential was suggested [25]. However, additional clinical trials using this tube-type BS are not in progress, and the effect and benefit cannot be objectively presented. In an animal study conducted by Laukkarinen et al. [20], a braided, self-expandable BS with a diameter of 4 mm was used for hepaticojejunostomy. In general, a self-expandable BS could be considered to cause fewer adverse events than those of tube-type BS due to biodegradation or fracture-induced fragmentation. Six months after the operation, it was confirmed that the diameter of the anastomosis area was statistically significantly wider in the BS insertion group than in the control group. However, there was no specific mention of how the biodegradation process occurred. The same researchers conducted a clinical study with the same BS [26]. However, after inserting the BS into the pancreaticojejunal anastomosis site, the BS disappearance time varied from less than 1 month to more than 12 months. Less than one month was probably due to migration, but the fact that it was not degraded for more than 12 months suggests that adverse events can occur due to this long-standing status.
Therefore, the ideal mechanical properties a BS used for DD biliary anastomosis should have are (1) very thin but strong radial force; (2) the ability to stay in shape for as adequate as we want; and (3) when it begins to degrade, it must totally degrade as soon as possible. Our novel PDO/Mg sheath-core BS was maintained for an adequate time and degraded quickly after that for the prevention of anastomosis-related stricture and fibrosis. Using the cross-and-hook knitting handmade method, the BS had a relatively narrow diameter with an adequate radial force. As shown in Supplementary Fig. 1, the same degradation phenomenon was confirmed by conducting an animal study (Fig. 6). BS deformity (fracture) did not occur until 4 weeks, and then quickly disappeared. Histologic analysis was performed to determine whether this maintenance period could prevent anastomosis-related stricture. As seen in Table 3, the median circumference values and ranges in all the measured points were narrower in the control group than in the stent group. Although not statistically significant due to the limited number of specimens in each group, we think the results would have changed significantly, if the 2 animals in the control group did not die. As seen in Fig. 7, fibrosis of the DD anastomosis area was more marked in the control group than in the stent group. This thickening of fibrosis was statistically different (P < 0.05) (Table 4). Therefore, these results suggested that the BS, which were being accurately maintained for a certain period of time, had the effect of preventing anastomosis-related stricture because the BS inhibited the induction of fibrosis.
The limitations of this experimental study were as follows. (1) This study used an in vivo animal model, and the results from a human study may substantially differ from those of our experimental study. (2) A small number of BS was used in the in vivo animal model. This is because DD anastomosis can only be performed at one site per CBD. (3) Two animals died immediately after surgery in the control group, so statistics could not be obtained with the same sample number. The 2 deaths were not due to a CBD problem, but occurred in the control group and not the stent group. It is possible that this critical adverse event could have been prevented because stent insertion might improve the animal’s postoperative condition. However, since we could not prove this, we cannot adequately comment on the possibility. (4) If more radiopaque markers were attached to the BS, it would have been possible to observe the BS shape more accurately. Previous reports showed that the overall shape of the BS could be observed by fluoroscopic examination by mixing barium sulfate with a biodegradable polymer. However, when barium sulfate is mixed with the biodegradable polymer, the properties of the polymer filament itself change significantly, so we could not obtain the desired properties. (5) Changes in the mechanical properties of the BS in the CBD during the follow-up period were not measured. (6) In this study, due to the characteristic that BS is maintained for about 6 weeks, stricture formation was observed by autopsy at 8 weeks after BS insertion. Since this is not a long-term outcome, it might be difficult to assign the significance of the long-term preventive effect of stricture formation in actual clinical situations. Therefore, additional animal studies on long-term outcomes and clinical studies are needed in the future.
Nevertheless, although additional clinical studies are required to observe the biocompatibility and preventive effect of BS on biliary stricture after DD biliary anastomosis, our current findings provide basic proof of concept for its use to prevent stricture and fibrosis after surgery. Our present results have thus yielded important insight into the potential benefits of the novel BS placement.
In conclusion, our study showed that our novel PDO/Mg sheath-core BS maintained its original shape and radial force for an adequate time and then disappeared without adverse events. The BS could prevent postoperative complications and stricture after DD biliary anastomosis. After further investigations and clinical trials, the novel BS have the potential to be used for temporary stent placement.




 XML Download
XML Download