

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cholangiocarcinoma can be divided into intrahepatic cholangiocarcinoma and extrahepatic cholangiocarcinoma (EHC) depending on the anatomical location [1]. EHC is not a common disease, especially in Europe and Western countries; however, the incidence of EHC has gradually increased worldwide [23]. In the United States, the age-adjusted incidence rate of EHC has increased for the last 4 decades; the incidence of intrahepatic cholangiocarcinoma has remained stable [4]. On the other hand, since EHC is a relatively common disease in Asia, many studies have been conducted [567]. The highest incidence rate for EHC was found in Korea [8].
EHC can be further distinguished into perihilar cholangiocarcinoma (PHC) and distal bile duct cancer (DBC) [9]. Although PHC and DBC share the same extrahepatic bile duct (BD) origin, there are differences in surgical treatment and prognosis. Major hepatic resections, including hemihepatectomy and trisectionectomy, are performed for PHC; pancreaticoduodenectomy is typically performed for DBC [10]. In addition, the cancer staging systems of PHC and DBC are different according to the 7th edition of the American Joint Committee on Cancer (AJCC) guidelines [11]. Therefore, PHC and DBC are currently considered as distinct entities based on differences in their tumor biology rather than the anatomical location of the tumor [12].
Previous studies have reported that the prognosis is similar depending on the location of tumor in cholangiocarcinoma [131415]. On the other hand, there are also studies showing that PHC has a worse prognosis than DBC [161718]. Prognostic factors of each subtype are also different according to other studies [192021]. However, small cohort sizes in previous studies prevent meaningful comparison between PHC and DBC. A comprehensive analysis between these subtypes should be based on a well-established database that includes radiologic findings, surgical outcomes, pathological reports, and records of adjuvant treatment. Therefore, the purpose of this study was to compare oncological outcomes between PHC and DBC based on data from a single large institute.
METHODS
Patients and data
This study was a retrospective cohort study with prospectively collected data. Patients who were pathologically diagnosed with EHC and underwent curative intent surgery at Seoul National University Hospital (Seoul, Korea) from 2001 to 2017 were reviewed for inclusion in the current study. Patients with distant metastasis, who received palliative surgery or neoadjuvant treatment, were excluded. Patients were classified into the PHC and DBC group.
The baseline characteristics were investigated and included age, sex, body mass index, American Society of Anesthesiologists physical status, and underlying disease. Tumor markers that included CA 19-9 and CEA were also checked before surgery. The type of operation, operation time, and estimated blood loss (EBL) were investigated. Data from after the surgery, including the hospital stay duration, the number of patients with complications above Clavien-Dindo classification grade III, and the efficacies of adjuvant chemotherapy and radiation therapy were also investigated.
This study was approved by the Institutional Review Board of our hospital (No. SNUH-2104-123-1213). This study was performed in accordance with the Declaration of Helsinki and written informed consent was waived due to its retrospective nature.
Pathologic findings with T stage reclassification
All specimens were examined pathologically after surgery and were reported based on the AJCC 7th edition guidelines. They were classified into PHC or DBC based on the gross findings of the specimen and pathological reports. Patients with tumor invading the first confluence of common BD were classified as PHC group, while patients with tumor invading distal BD were classified as DBC group. The pathological reports included resection status, tumor size, T stage, and metastatic status of harvested lymph nodes (LN). In addition, the status of cell differentiation, angiolymphatic invasion, venous invasion, and perineural invasion were reported.
Pathological T stage had to be unified because there were differences between PHC and DBC in the cancer staging systems of the AJCC 7th edition guidelines. Therefore, all lesions were defined relative to the BD as ‘confined to BD’ or ‘beyond BD.’ In PHC, stage T1 and T2a were defined as tumors confined to BD; stage T2b, T3, and T4 were defined as tumors beyond BD. In PHC cases, stage T1 and T2a tumors were classified as confined to BD because they infiltrate the surrounding adipose tissue; stage T2b, T3, and T4 were classified as beyond BD because they infiltrate the hepatic parenchyma. In DBC cases, stage T1 and T2 could be classified as confined to BD because they infiltrated only the surrounding soft tissue, as listed in the pathology report; stage T3 and T4 were considered as tumors beyond BD.
Long-term oncological outcomes with stage matching
Overall survival of the PHC and DBC groups was evaluated by the Kaplan–Meier estimator for the 5-year survival rate (5YSR). Univariate and multivariate analyses were performed to identify prognostic factors for each group. Additional analysis was performed in 4 groups by stage matching using combinations of the tumor extent and status of LN metastasis. Recurrence rates and recurrence patterns were also investigated.
Statistical analysis
Continuous variables were calculated as the mean and standard deviation and were analyzed with Student t-test or the Mann–Whitney U-test, as appropriate. Categorical variables were compared using the chi-square test or Fisher exact test.
Survival analysis was performed using the Kaplan–Meier estimator. Statistical significance was defined as P < 0.05. To determine the independent prognostic factors for survival outcomes, multivariate analysis was performed using a Cox proportional hazards model. All statistical calculations were performed using IBM SPSS Statistics ver. 25.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Patients and clinicopathologic findings
There were 997 patients confirmed pathologically as EHC who underwent curative intent surgery between January 2001 and December 2017. Excluded from the study were 206 patients who underwent palliative surgery, 73 patients who had distant metastasis, and 13 patients who received neoadjuvant therapy; 25 patients were missed during the follow-up period. Consequently, 680 patients were enrolled in this study, of whom 295 (43.4%) were diagnosed as PHC and 385 (56.6%) were diagnosed as DBC (Fig. 1).

The baseline demographics and clinicopathological outcomes of each group are shown in Table 1. The demographics were comparable between the PHC and DBC groups. Patients with a CA 19-9 level of >37 U/mL were more frequent in the PHC group than in the DBC group.
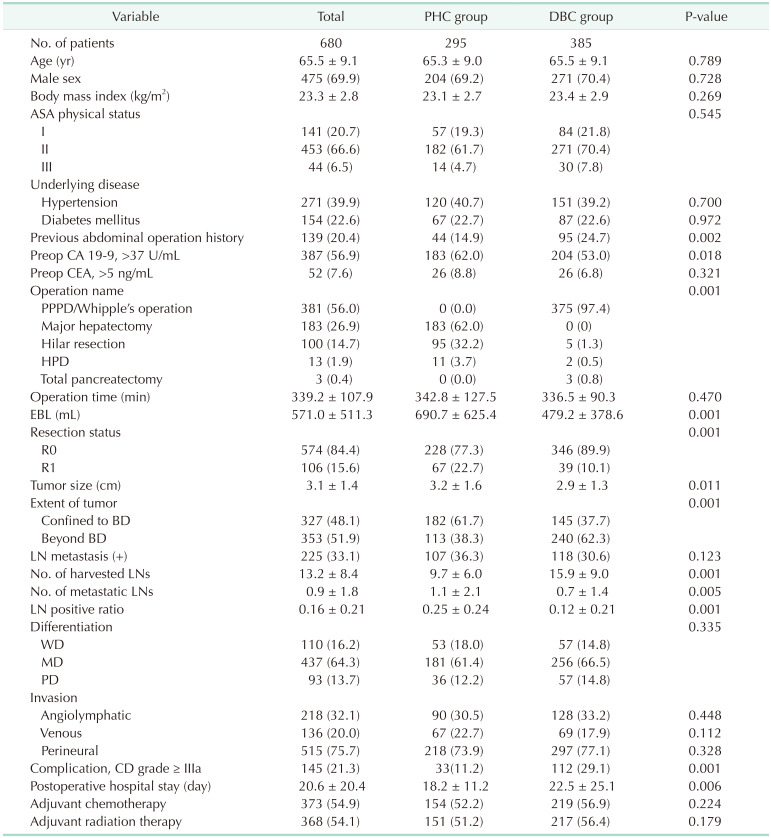
Table 1
Baseline demographics and clinicopathologic outcomes
Values are presented as number only, mean ± standard deviation, or number (%).
PHC, perihilar cholangiocarcinoma; DBC, distal bile duct cancer; ASA, American Society of Anesthesiologists; Preop, preoperative; PPPD, pylorus preserving pancreaticoduodenectomy; HPD, hepatopancreaticoduodenectomy; EBL, estimated blood loss; BD, bile duct; LN, lymph node; CD, Clavien-Dindo classification.
![]()
For the type of operation according to the location of lesion, major hepatectomy was the most common operation in the PHC group (62.0%) and pancreaticoduodenectomy was the most common in the DBC group (97.4%). Most of the operations were performed by open method (98.7%). Operation time was comparable between the 2 groups; however, EBL was much more prevalent in the PHC group.
The R0 resection rate was higher in the DBC group than in the PHC group (77.3% vs. 89.9%, P = 0.001). Patients in the PHC group demonstrated larger mean tumor sizes than those in the DBC group (3.2 cm vs. 2.9 cm, P = 0.011). However, tumors confined to the BD were more frequent in the PHC group than in the DBC group (61.7% vs. 37.7%, P = 0.001). The ratio of patients with LN metastasis in each group was comparable. Although patients in the PHC group demonstrated fewer harvested LNs (9.7 vs. 15.9, P = 0.001), the number of metastatic LNs was higher than that in the DBC group (1.1 vs. 0.7, P = 0.005).
Postoperative complications were more common in the DBC group (11.2% vs. 29.1%, P = 0.001). In DBC group, the most common complication was postoperative pancreatic fistula (n = 47, 42.0%), followed by wound-related complications (n = 23, 20.5%) and intraabdominal fluid collection (n = 20, 17.9%). In PHC group, the most common complication was intraabdominal fluid collection (n = 13, 39.4%), followed by wound-related complications (n = 9, 27.3%) and pleural effusion (n = 5, 15.2%). Patients in the PHC group demonstrated a shorter duration of hospital stay than those in the DBC group (18.2 vs. 22.5 days, P = 0.006). After recovery from surgery and discharge from the hospital, the ratio of patients who received adjuvant chemotherapy or radiation therapy in each group were comparable. There was also no difference in chemotherapy regimen between DBC and PHC groups (5-fluorouracil, 74.0% vs. 75.3%, respectively; gemcitabine, 15.1% vs. 15.6%, respectively; P = 0.659). Radiation up to 55 Gy was used for more than 4 weeks in all patients who received adjuvant radiation therapy.
Long-term oncological outcomes
The 5YSR of the entire study cohort was 40.4%. The 5YSR of the PHC group was worse than that of the DBC group (30.7% vs. 47.8%, P = 0.001) (Fig. 2). After stage matching into 4 subgroups based on combinations of tumor extent and LN metastasis, the patients of the PHC group showed worse survival outcomes than those of the DBC group in 3 subgroups; the exception was for the subgroup with tumors confined to the BD and positive LN metastasis (Fig. 3).
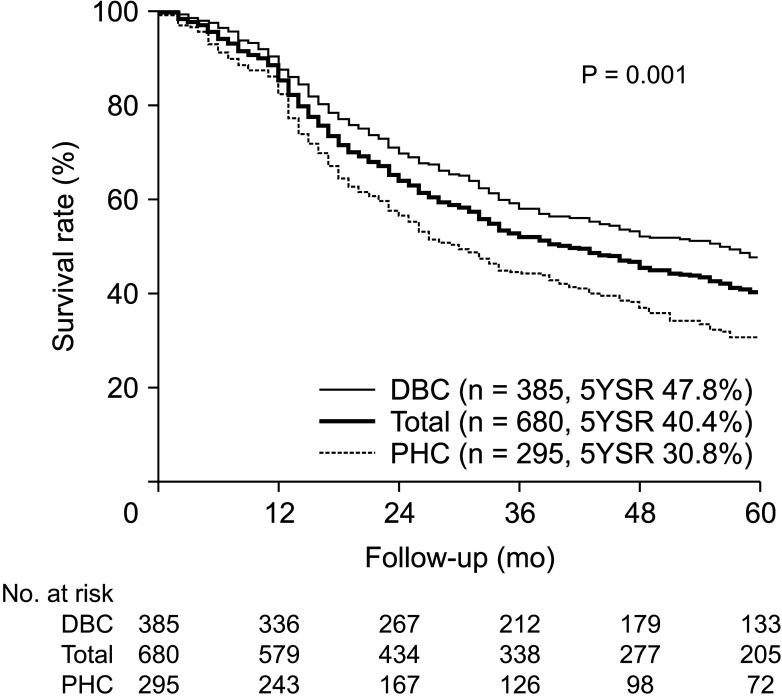
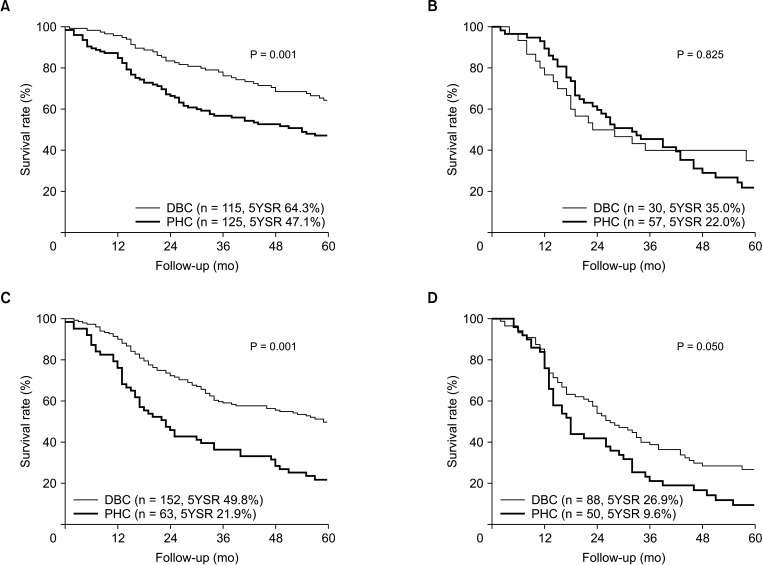
Fig. 2
Overall survival of extrahepatic cholangiocarcinoma according to tumor location. The overall survival of perihilar cholangiocarcinoma (PHC) was worse than distal bile duct cancer (DBC). 5YSR, 5-year survival rate.
![]()
Fig. 3
Overall survival between perihilar cholangiocarcinoma (PHC) and distal bile duct cancer (DBC) after stage matching. (A) The overall survival of PHC was worse in patients with tumors confined to bile duct (BD) and without lymph node (LN) metastasis. (B) The overall survival of PHC was comparable with DBC in patients with tumors confined to BD and LN metastasis. (C) The overall survival of PHC was worse in patients with tumors beyond BD and without LN metastasis. (D) The overall survival of PHC was worse in patients with tumors beyond BD and LN metastasis. CTx, chemotherapy; RTx, radiation therapy; 5YSR, 5-year survival rate.
![]()
The recurrence patterns are shown in Table 2. The overall recurrence rate was higher in the PHC group than in the DBC group (59.7% vs. 51.9%, P = 0.045). However, when recurred patients were divided into local and systemic recurrences, there was no difference in the type of recurrence between the 2 groups (P = 0.455).

Prognostic factors according to anatomical location
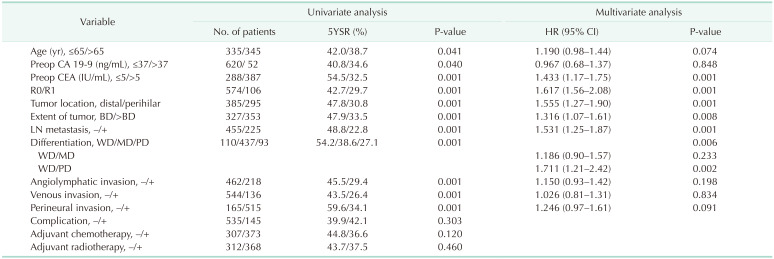
Further analysis was performed to identify prognostic factors that affect the survival outcomes. In multivariate analysis, the preoperative CEA level (hazard ratio [HR], 1.433; 95% confidence interval [CI], 1.17–1.75; P = 0.001), R0 resection (HR, 1.617; 95% CI, 1.56–2.08; P = 0.001), tumor extent (HR, 1.316; 95% CI, 1.07–1.61; P = 0.008), LN metastasis (HR, 1.531; 95% CI, 1.25–1.87; P = 0.001), and cell differentiation (HR, 1.711; 95% CI, 1.21–2.42; P = 0.002) were identified as prognostic factors for 5YSR in patients with resected EHC (Table 3). The tumor location was also identified as an independent prognostic factor in multivariate analysis (HR, 1.555; 95% CI, 1.27–1.90; P = 0.001).
To compare prognostic factors between PHC and DBC, multivariate analysis was performed in each group (Table 4). In the PHC group, the preoperative CA 19-9 level, R0 resection, and the tumor extent were revealed as independent prognostic factors. The most powerful risk factor of PHC was the preoperative CA 19-9 level (HR, 1.844; 95% CI, 1.37–2.48; P = 0.001). In the DBC group, age, R0 resection, LN metastasis, cell differentiation, and perineural invasion were revealed as important prognostic factors. The most powerful risk factor of DBC was poor cell differentiation (HR, 2.634; 95% CI, 1.62–4.28; P = 0.001).

Effect of adjuvant treatment in extrahepatic cholangiocarcinoma
For patients with advanced-stage tumors (above stage 2), adjuvant radiation therapy affected the survival outcome, but there was no effect for adjuvant chemotherapy (Supplementary Fig. 1A, B). The 5YSRs of patients who received or did not receive radiation therapy were 35.8% and 29.5%, respectively (P = 0.022). In addition, adjuvant chemotherapy was effective for patients with R1 resection (Supplementary Fig. 1C). The 5YSRs of patients who received or did not receive chemotherapy were 37.3% and 13.2%, respectively (P = 0.040). Adjuvant radiation therapy was statistically not important in R1 patients, but the 5YSR of patients who received or did not receive it differed by 35.2% and 15.7% (Supplementary Fig. 1D). For patients with R1 status, PHC group showed better 5YSR when they received chemotherapy (37.4% vs. 10.7%, P = 0.100; Supplementary Fig. 2A) or radiation therapy (33.6% vs . 13.5%, P = 0.586; Supplementary Fig. 2B). In the DBC group, although there was no statistical difference in overall survival, chemotherapy (37.0% vs. 20.0%, P = 0.367; Supplementary Fig. 2C), and radiation therapy (37.9% vs. 20.8%, P = 0.697; Supplementary Fig. 2D) were effective in increasing 5YSR for patients with R1 status.
DISCUSSION
PHC and DBC are classified as EHC because they have the same origin in the mucous membrane of the extrahepatic biliary tract. However, the cancer staging system and surgical treatment of each group are different according to their anatomical location. Therefore, they are treated as different types of carcinoma and studied separately. The epidemiological, pathological, and oncological differences between the 2 groups are not well studied. This study compared the oncological outcomes according to the tumor location between the 2 groups to improve survival rates by identifying factors that influence the prognosis.
The perioperative short-term outcomes are different between PHC and DBC because of the different methods of surgical treatment. PHC shows more EBL due to bleeding during liver resection as compared with DBC. After surgery, complications are more frequent in the DBC group than in the PHC group because of postoperative pancreatic fistulae. In the DBC group, intraabdominal fluid collection related to a postoperative pancreatic fistula was the most common complication, followed by wound complications. In the PHC group, intraabdominal fluid collection around the liver resection site was the most common complication, also followed by wound complications. Consequently, more complications led to longer hospital stays in the DBC group.
In 2015, Ercolani et al. [13] reported pathologic differences between subtypes of cholangiocarcinoma; however, the differences in the cancer staging systems between subtypes were not considered. To compare pathological findings and long-term survival outcomes between PHC and DBC, T stage reclassification and stage matching using tumor extent and LN metastasis status were performed in our study. The 5YSR of the PHC group was worse than the DBC group. In 2011, Murakami et al. [16] reported similar overall survival between the PHC and DBC groups (5YSR of 37% vs. 43%, respectively). In 2017, Waseem and Tushar [14] reported better median survival for the DBC group, although overall survival was not significantly different between the 2 groups. However, the results of these previous studies were limited by small sample sizes and different cancer stage proportions between the PHC and DBC groups. The number of patients in our study was 608, whereas the number of patients in the studies mentioned above was between 106 and 152.
There was also a difference in prognostic factors between the 2 groups. In 2018, Bird et al. [22] performed meta-analysis of prognostic factors for overall survival in patients with resected PHC. They reported T stage, LN involvement, microvascular invasion, perineural invasion, and cell differentiation as significant prognostic factors. However, in our study, the preoperative CA 19-9 level, resection margin status, and T stage were identified as prognostic factors for PHC. In addition, in 2016, Wellner et al. [23] performed a meta-analysis and reported that perineural invasion, LN metastasis, positive resection margin status, and not-well-differentiated adenocarcinoma were associated with shorter survival times in DBC patients. These results were consistent with the findings of our study. Achieving R0 resection could be very important, since it was a significant prognostic factor for both groups.
The role of adjuvant treatment in EHC remains unclear. In 2015, Hoehn et al. [24] reported that there was no benefit from adjuvant treatment in patients with resected EHC (median survival for surgery only, 2.8 years; surgery with adjuvant treatment, 2.76 years). However, they reported adjuvant chemotherapy and radiation therapy improved survival outcomes of patients with LN metastasis or positive surgical margins. In 2012, our institution also reported beneficial effect of adjuvant radiation therapy in patients with microscopic residual disease after surgical resection for EHC [25]. There was no difference in overall survival between patients with R0 and R1 status who received adjuvant radiation therapy (5YSR: R0, 46.3% vs. R1, 41.4%; P = 0.664). In current study, patients with advanced disease above stage 2 who received radiation therapy showed better 5YSR (35.8% vs. 29.5%, P = 0.022). In addition, patients who received adjuvant chemotherapy or radiation therapy in R1 status showed better 5YSR than who did not (chemotherapy: 37.3% vs. 13.2%, P = 0.040; radiation therapy: 35.2 vs. 15.7%, P = 0.448). Therefore, it is important to select the target for adjuvant chemotherapy and radiation therapy appropriately.
The present study has some limitations. First, since it was a retrospective study, the patients with missing data had to be excluded. Second, only patients who underwent surgery were included in our study, and patients with advanced disease that could not undergo surgery were excluded. Therefore, there was a limit to describing the entity of the entire disease. Last, there were changes in treatment methods over time because of the long study period. In particular, adjuvant chemotherapy and radiation therapy showed differences according to time and physician.
In conclusion, there were differences in oncological outcomes between PHC and DBC patients, including pathologic findings, survival outcomes, and prognostic factors. Therefore, it is important to plan a treatment strategy with consideration of the exact tumor location.
 XML Download
XML Download