

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Breast cancer (BC) is considered the commonest cancer in women [1]. During recent decades, the incidence of BC among young women has rapidly increased in Asian countries. Furthermore, 14%–16% of all BCs are diagnosed in women of childbearing age [234]. The mean maternal age at first childbirth has considerably increased in Organization for Economic Cooperation and Development countries, and the mean maternal age at first childbirth in Korea is approximately 5 years higher than that in the United States (31.6 vs. 26.8 years) [2]. Given the trend toward delaying motherhood, an increasing subgroup of women will develop BC before they have children. Thus, patients with BC may have questions on fertility-related issues and whether pregnancy might alter their risk of disease progression or possibly lead to poor survival outcomes.
Pregnancy that occurs more than several years after a diagnosis of BC does not appear to affect survival [56]. However, it is unclear how long women should wait after undergoing BC treatment before trying to conceive. The general recommendation is to postpone pregnancy for several years after BC treatment, and this is based on concerns that pregnancy-related hormones, especially estrogen, might stimulate dormant micrometastases and thereby worsen survival. Interestingly, pregnancy has dual effects on BC [7], with the risk of incident BC increasing shortly after pregnancy and subsequently decreasing. Moreover, previous studies have revealed contradictory results with regard to the pregnancy-associated effects on BC-related outcomes. For example, significant decreases in mortality were identified using data from 3 population-based cancer registries and a meta-analysis of 14 studies [89]. Conversely, another study revealed no difference in disease-free survival (DFS) between women who conceived after a BC diagnosis and a matched nonpregnant group [10]. Subgroup analyses have suggested that specific clinical factors may need to be considered, as some studies have revealed increased risk of recurrence in patients who conceived within 1 year after their BC diagnosis [1112], whereas other studies revealed differences based on the estrogen receptor (ER) status, breastfeeding history, and other maternal factors [13].
It is unclear whether pregnancy after adjuvant therapy for BC is associated with adverse effects or benefits that are related to the biased selection of relatively healthy patients. Thus, there are concerns regarding whether subsequent pregnancy may be linked to poor outcomes, especially in patients with ER-positive BC. Furthermore, there are few biological hypotheses that can explain how a subsequent pregnancy might confer protective effects. One hypothesis, based on preclinical models, is that high estrogen concentrations after estrogen deprivation might induce apoptosis in ER-positive BC cell lines [14]. Therefore, we aimed to evaluate whether pregnancy after a BC diagnosis was associated with positive or negative real-world outcomes in Korea, which might help clinicians provide their patients with crucial information and guide them in their decision with regard to conception. Few studies have included sufficiently large samples to perform subanalyses according to BC treatment and the time from BC diagnosis to conception. Furthermore, given the lack of information regarding an appropriate interval between BC treatment and subsequent pregnancy [1516], we evaluated the interval between BC treatment and pregnancy using real-world claims-based data from the Korean National Health Insurance Service Database.
METHODS
Study population and data source
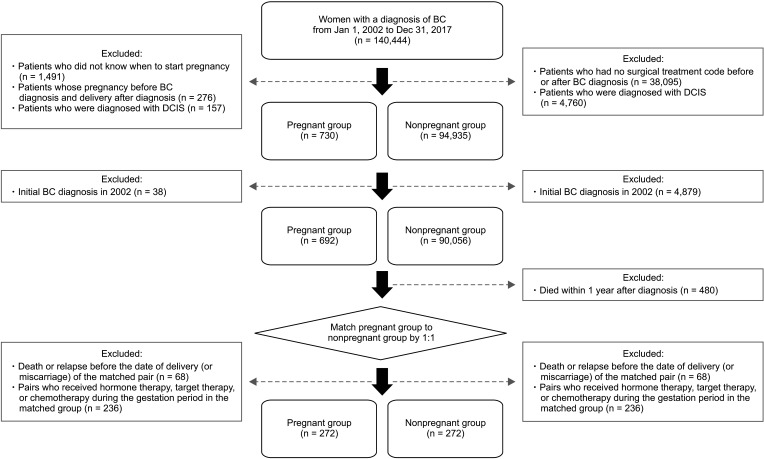
This study retrospectively analyzed Korean National Health Insurance Service data from a randomly selected sample comprising 50% of Korean women who were younger than 60 years, were diagnosed with BC from 2002 to 2017, and underwent surgical treatment for BC. The diagnosis of BC was identified using codes C50 and D05 from the International Classification of Diseases, the 10th edition (ICD-10). Patients were excluded if they did not know when they had conceived, if they were pregnant before the BC diagnosis, or if their pregnancy ended after the BC diagnosis. Patients were also excluded who were diagnosed with ductal carcinoma in situ using code D05 from the ICD-10. In addition, a washout period was created by excluding patients who were initially diagnosed with BC during 2002, and patients who died within 1 year after BC diagnosis were excluded.
Patient-level matching was performed to reduce the possibility of selection bias associated with the fundamental differences between pregnant and nonpregnant women. The matching was performed 1:1 (pregnant:nonpregnant patients with BC) according to age, the Charlson comorbidity index (CCI; Supplementary Table 1), the initial BC diagnosis year, chemotherapy use, hormone therapy use, and use of targeted therapy (Supplementary Table 2). After selecting the matched pairs of patients, we excluded patients who died or experienced a BC relapse before the pregnancy ended, given that the survival in the pregnant group would be extended by the gestation period. In addition, to ensure consistency between the pregnant and nonpregnant groups, we excluded matched pregnant patients who had undergone chemotherapy, hormone therapy, or targeted therapy during the gestation period. Thus, the present study identified 544 matched women with BC, who were assigned to the pregnant group (cases, n = 272) or the nonpregnant group (controls, n = 272) (Fig. 1).
Variable definitions
The pregnant group included patients who had a completed pregnancy (ICD-10 codes of O80–O84), with the beginning of the pregnancy defined as 37 weeks before the date of the delivery (identified using the claims with ICD-10 codes of O80–O84). Moreover, the pregnant group included patients who had a miscarriage (ICD-10 codes of O00–O08), with the beginning of pregnancy defined as 30 days before a claim that involved a pregnancy test procedure code. The nonpregnant group had the entry date for follow-up, as well as the completed pregnancy or miscarriage status, which were defined based on matching with regard to the pregnant group.
Survival outcomes were calculated from the pregnancy end date, and the DFS interval was defined based on the first instance of BC recurrence or death. All-cause mortality was evaluated during a follow-up period, which was identified by linking the patient’s records to death certificate data from the national death registry. In the pregnant group, recurrence was identified based on hospitalization for >2 days and BC-related surgery or chemotherapy that was completed after the gestation period. In the nonpregnant group, recurrence was identified based on hospitalization for >2 days and BC-related surgery or chemotherapy that was completed >1 year after the initial BC diagnosis.
The CCI [17] was used to identify comorbidities from the 12-month period before the initial BC diagnosis. The National Health Insurance Service data do not include information regarding BC subtype, given the nature of the health insurance claims; therefore, we inferred the BC subtypes according to the use of hormone therapy, targeted therapy, and/or chemotherapy. Data with regard to the prescriptions for hormone therapy, targeted therapy, and chemotherapy were extracted from claims during the study period using the Anatomical Therapeutic Chemical codes (Supplementary Table 2).
Subgroup analyses according to tumor subtype
The National Health Insurance Service data does not contain information regarding pathological BC subtype; therefore, we estimated the BC subtype for each case according to the use of chemotherapy, hormone therapy, and/or targeted therapy. This created 8 possible treatment combinations, although we excluded 2 subgroups that were deemed clinically irrelevant (hormone therapy plus targeted therapy without chemotherapy or targeted therapy without chemotherapy). Thus, we defined the BC cases as hormone receptor (HR)-positive BC (based on hormone therapy use) or HR-negative BC (based on hormone therapy nonuse). The use of targeted therapy was utilized to identify cases that involved human epidermal growth factor receptor 2 (HER2)-positive BC (Supplementary Table 3).
Statistical analyses
The baseline characteristics of the matched pregnant and nonpregnant patients with BC were compared using the chi-square test, Fisher exact test, or Student t-test, as appropriate. Cox proportional hazard models were used for univariate and multivariate analyses that were adjusted for age, CCI group, hormone therapy use, targeted therapy use, chemotherapy use, and the year of the initial BC diagnosis. All statistical analyses were performed using SAS software ver. 9.4 (SAS Institute, Cary, NC, USA) and differences were considered statistically significant at the P-values of <0.05.
To maximize comparability, we constructed propensity score-matched cohorts. Propensity scores of pregnancy were calculated using logistic regression analysis with the following covariates: age, CCI group, the 3 BC treatment types, and the year group of BC diagnosis. Each patient in the pregnant group was matched to a patient in the nonpregnant group. However, 1:1 matching may introduce unintended statistical errors; thus, bootstrapping was performed with the control group selected 10 times through random seeding, and the analyses were repeated for overall survival (OS) and DFS. In addition, the standardized mean difference of each variable was compared before and after matching to evaluate the adequacy of matching (Supplementary Table 4).
Post hoc analyses
To compare OS and DFS between the pregnant and nonpregnant groups, the noninferiority margin was set at 5% in consideration of both statistical reasoning and clinical judgment. The targeted sample size for the noninferiority tests between the pregnant and nonpregnant groups was calculated based on the formulas [18].
Ethics statement
The study was reviewed by the Institutional Review Board of Gachon University Gil Medical Center, which waived the requirement of ethics approval in compliance with governmental laws and regulations (No. GFIRB2019-240), and the requirement to obtain written consent was waived due to fact that human subjects were not involved in the study. All study methods were carried out in accordance with the tenets of the Declaration of Helsinki.
RESULTS
Patient characteristics
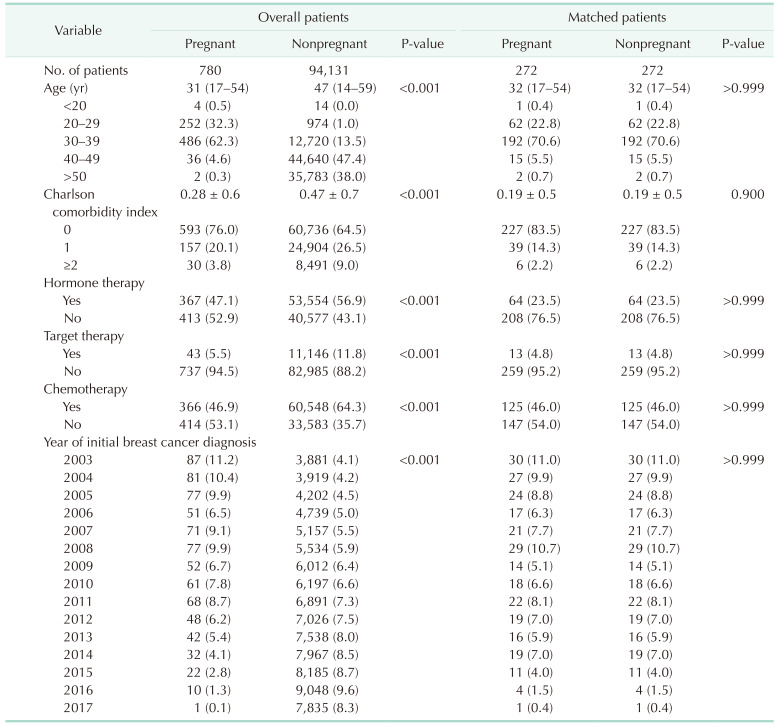
Table 1 shows the baseline characteristics of participants. The mean age at BC diagnosis was 32 years (median, 32 years; range, 17–54 years). The treatments included chemotherapy (250 patients, 46.0%), trastuzumab (26 patients, 4.8%), and hormone therapy (128 patients, 23.5%). The median times from the BC diagnosis to conception were 1 year among the 139 patients who conceived within 3 years after the BC diagnosis and 5 years among the 133 patients who conceived ≥3 years after the BC diagnosis.
Survival analysis
The median follow-up period was 10 years, which was calculated from BC diagnosis until death. The actuarial 10-year OS rates were 97.4% for the pregnant group and 91.9% for the nonpregnant group. The median DFS intervals were 8 years in both the matched groups of pregnant and nonpregnant patients. The pregnant group had a significantly better OS (adjusted hazard ratio [aHR], 0.29; 95% confidence interval [CI], 0.12–0.68; P = 0.005), including most subgroup analyses. A total of 45 patients (8.3%) experienced DFS events, including 25 pregnant patients (9.2%) and 20 nonpregnant patients (7.4%). The pregnant group did not have a significantly inferior DFS (aHR, 1.10; 95% CI, 0.61–1.99; P = 0.760) (Table 2), which prompted us to perform various subgroup analyses (Tables 3 and 4).
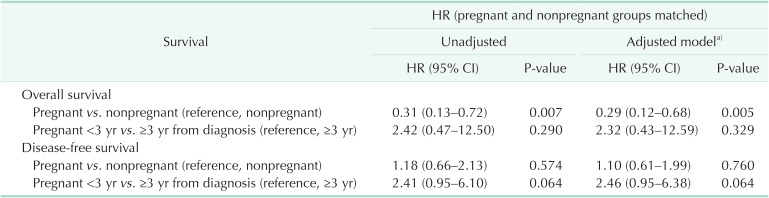
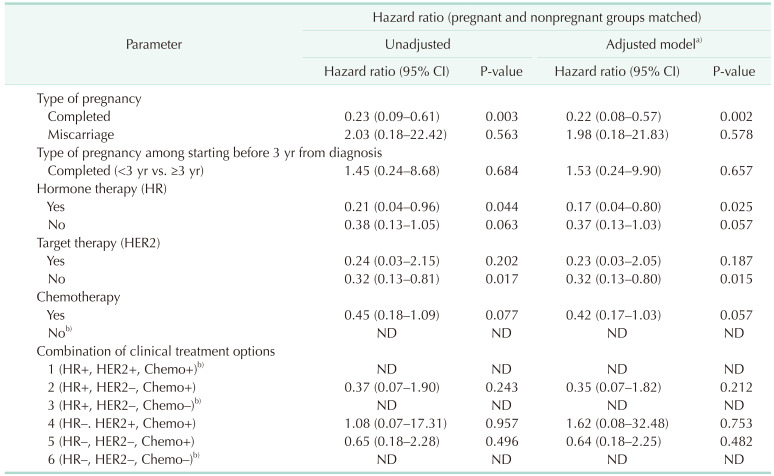
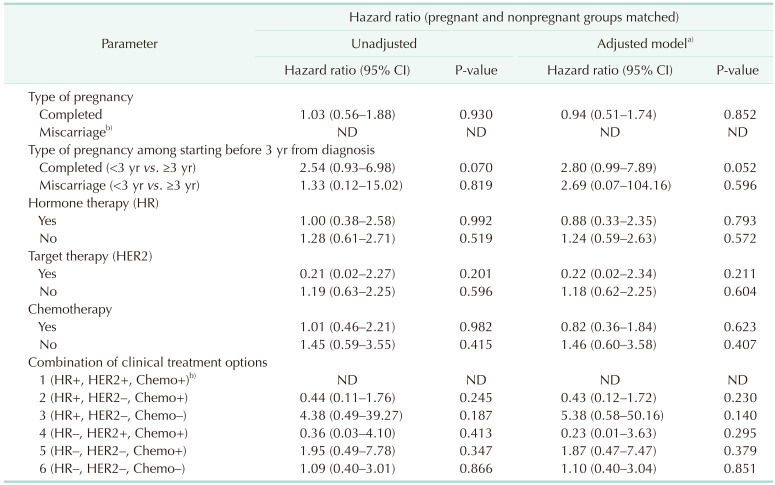
Table 2
Hazard ratios (HRs) for overall survival and disease-free survival according to pregnancy status
![]()
Table 3
Hazard ratios for overall survival according to subgroup
CI, confidence interval; HR, hormone receptor; HER2, human epidermal growth factor receptor 2; ND, not detected.
a)Adjusted for age, Charlson comorbidity index group, hormone therapy, target therapy, and chemotherapy, and the year of initial breast cancer diagnosis; b)No deaths occurred in the pregnant group during the observation period.
![]()
Table 4
Hazard ratios for disease-free survival according to subgroup
CI, confidence interval; HR, hormone receptor; HER2, human epidermal growth factor receptor 2.
a)Adjusted for age, Charlson comorbidity index group, hormone therapy, target therapy, and chemotherapy, and the year of initial breast cancer diagnosis. b)No cases of breast cancer recurrence or death occurred in the pregnant group during the observation period.
![]()
Subgroup analyses based on time to pregnancy after the BC diagnosis
Analyses of DFS were performed among pregnant women depending on whether they conceived <3 or ≥3 years after the BC diagnosis, although no significant difference was detected (aHR, 2.46; 95% CI, 0.95–6.38; P = 0.064). We evaluated whether this variable was associated with a protective effect or selection bias by comparing DFS among the nonpregnant patients and patients who conceived <3 or ≥3 years after the BC diagnosis. The results revealed that conception at <3 years after the BC diagnosis was associated with a noninferior DFS, even after adjustment for the use of hormone therapy, chemotherapy, and targeted therapy (aHR, 0.99; 95% CI, 0.50–1.94; P = 0.974). Furthermore, conception at ≥3 years after the BC diagnosis was associated with noninferior DFS, even after adjusting for the treatment covariates (aHR, 1.48; 95% CI, 0.42–5.24; P = 0.546). The pregnant group had a significantly better OS (compared to the nonpregnant group), including each subgroup of pregnant patients, and no significant difference in this association was observed for conception at <3 or ≥3 years after the BC diagnosis.
Subgroup analyses according to systemic therapy
Noninferior OS was observed for most of the treatment-specific subgroups of pregnant patients. In addition, no significant differences in DFS were observed according to the treatment subtype when we compared the pregnant and nonpregnant groups (Figs. 2, 3).
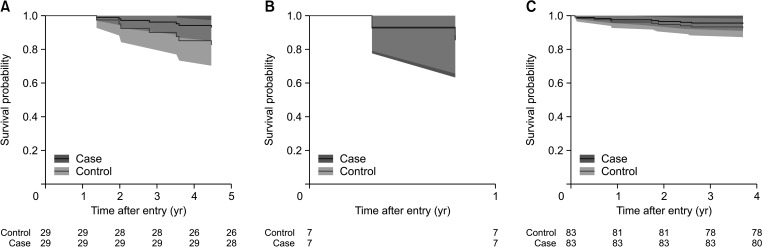
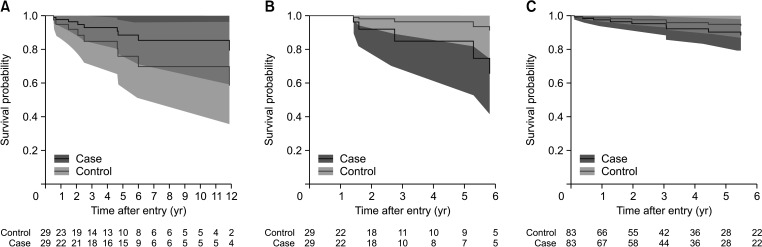
Fig. 2
Time-to-event curves for the overall survival for selective treatment groups. (A) HR, yes; HER2, no; chemotherapy, yes. (B) HR, no; HER2, yes; chemotherapy, yes. (C) HR, no; HER2, no; chemotherapy, yes. HR, hormone receptor (anti-hormonal therapy); HER2, human epidermal growth factor receptor 2 (target therapy). Created using SAS software (ver. 9.4; SAS Institute Inc., Cray, NC, USA).
![]()
Fig. 3
Time-to-event curves for disease-free survival for selective treatment groups. (A) HR, yes; HER2, no; chemotherapy, yes. (B) HR, yes; HER2, no; chemotherapy, no. (C) HR, no; HER2, no; chemotherapy, yes. HR, hormone receptor (anti-hormonal therapy); HER2, human epidermal growth factor receptor 2 (target therapy). Created using SAS software (ver. 9.4; SAS Institute Inc., Cray, NC, USA).
![]()
Subgroup analyses according to pregnancy outcomes
Subgroup analyses of DFS were performed according to whether the pregnancy outcome was delivery or an abortion/miscarriage. The matched nonpregnant patients (compared to the pregnant patients with an abortion/miscarriage) did not experience death or recurrence, and the DFS comparison could only be performed for the matched patients with delivery as the pregnancy outcome. No significant difference in DFS was observed between pregnant patients with delivery as the outcome and the matched subgroup of nonpregnant patients (aHR, 0.94; 95% CI, 0.51–1.74; P = 0.852).
The bootstrapping method revealed no significant difference in DFS between the pregnant and nonpregnant groups of patients with BC. After 10 resampling procedures, nonsignificantly better OS was observed in the pregnant group (Supplementary Table 5).
DISCUSSION
The present study revealed that pregnant Korean patients with surgically treated BC had significantly better OS (compared to nonpregnant matched Korean patients with BC), although no significant difference was observed for DFS in the various subgroup analyses. Furthermore, we failed to detect differences in DFS when we evaluated pregnant patients who had term delivery or miscarriage/abortion as their pregnancy outcome (compared to the matched control patients).
By calculating the required sample size based on a noninferiority margin of 5%, a sample size of 157 each for the pregnant and the nonpregnant groups was required to estimate the OS, and a sample size of 32 each was needed for the DFS. Most of the subgroup analyzes in our study had the required sample size.
Similar studies have indicated that patients who become pregnant soon after their BC diagnosis may introduce selection bias because of their relatively good expected prognosis. This type of selection bias cannot be completely eliminated because it is impossible to randomize whether patients will become pregnant, although an ongoing study is aiming to assess the contribution of such a healthy-mother bias [19]. In addition to selection bias, there are several potential limitations that are associated with studies suggesting a positive correlation between pregnancy after a BC diagnosis and OS For example, the “conclusive” reviews have included studies that were performed over many decades and, during that time, there have been significant improvements in the treatment of BC, especially HR-positive BC, which may create heterogeneity in the clinical and treatment characteristics of the cohort. Furthermore, it is difficult to control for biological factors and risk determinants, as these data are often missing in retrospective and population-based studies. The patient’s ER status is especially important because pregnant women with ER-positive BC might have poor outcomes, given the high estrogen concentration during pregnancy; however, retrospective studies often fail to determine the ER status. Azim et al. [10] were the first to report this issue and compared the survival outcomes according to the ER status in their multicenter observational study.
The interval between the BC diagnosis/treatment and pregnancy is another potential source of interstudy heterogeneity. We aimed to address this issue by performing subgroup analyses of patients with non-relapsed BC and an interval from diagnosis to pregnancy of <3 or ≥3 years. The 3-year cutoff point was selected based on Korea’s official practice wherein a 3-year disease-free status from the initial BC diagnosis is clinically regarded as being a safe interval for conception. We analyzed the interval issue based on clinical relevance and observed no survival difference between these 2 groups.
Young women have an increased risk of developing biologically aggressive forms of BC, relative to older women. In addition, the trend toward delaying pregnancy means that many young women will be diagnosed with BC and may still wish to have children after their diagnosis. Pregnancy-related concerns are a high priority for these patients; yet, there are limited data, according to BC subtype and stage, regarding the safety of pregnancy. Furthermore, there is persistent debate regarding the optimal timing of pregnancy after the patient has completed BC treatment. The current recommendation is that patients should delay conception for ≥2 years after their BC diagnosis, which is based on the high incidence of tumor recurrence during the first 2 years, as reported by Pagani et al. [20]. Moreover, this interval allows the patient to recover from chemotherapy-induced ovarian toxicity [21]. Other studies have indicated that pregnancy is safe at >6 months after the BC diagnosis, based on adjusted relative risk values of 1.7–2.2 for death among women who conceived <6 months after their BC diagnosis [5822].
The present study involved subgroup analyses according to the type of systemic therapy and time from diagnosis to pregnancy. The biological type of BC was inferred based on the patient’s treatment(s) because the health insurance database did not include pathological findings. For example, lymph node positivity would be expected if the patient had undergone chemotherapy, HR positivity would be expected if the patient underwent hormone therapy, and HER2 positivity would be expected if the patient had undergone targeted therapy. We only identified a relatively small proportion of HR-positive BC cases (24%) and failed to detect significant differences in DFS according to pregnancy status in the HR-positive and HR-negative subgroups. Furthermore, pregnant women had noninferior OS, regardless of their HR status. In addition, we failed to detect differences in DFS according to pregnancy status in the subgroups of patients with inferred HER2-positive or triple-negative BC, although the small sample size limited the power of these analyses. Lambertini et al. [23] have recently reported that HER2-positive BC was associated with positive pregnancy-related outcomes based on data from the Neoadjuvant Lapatinib and/or Trastuzumab Treatment Optimisation (NeoALTTO) and Adjuvant Lapatinib and/or Trastuzumab Treatment Optimisation (ALLTO) trials; however, these authors too failed to detect a significant difference in DFS according to pregnancy status among young patients with HER2-positive BC. According to a very recent study by Li et al. [24], the prognosis in HR-positive young BC patients was not worse than that in HR-negative young BC patients.
Chemotherapy administered during the first trimester may be associated with fetal complications, which has prompted a recommendation to delay chemotherapy in pregnant patients with lymph node-positive BC. However, the recommended delay may last until after delivery or only until the completion of the first trimester because delays in adjuvant therapy are associated with relatively poor survival [25]. Hormone therapy has traditionally been recommended for 5–10 years for endocrine-responsive tumors, which requires the patient to delay pregnancy because of the treatment’s potential teratogenicity. Increased risks of mortality have been observed, which might be associated with the adverse effects of pregnancy in women with more advanced disease; however, the effects of hormone therapy in this setting might be considered positive because of the healthy-mother bias [26]. Our findings suggest that survival benefits might be achieved by delaying pregnancy for >1 year after chemotherapy and for >3 years after hormone therapy, based on the results from the matched pregnant and nonpregnant patients with BC. We observed no difference in survival between the pregnant and nonpregnant groups, although it is possible that increased risks might be associated with the use of less aggressive treatments or delayed treatment initiation in pregnant women.
Pregnancy-related safety remains a concern for ER-positive BC, although one study in patients with ER-positive BC revealed no significant difference in the 5-year DFS rate according to the pregnancy status [27]. Another international multicenter study revealed no significant difference in DFS according to the pregnancy status among patients with ER-positive BC or ER-negative BC [1013]. However, that study also suggested that pregnant patients with ER-negative BC had significantly better OS. These data provide good evidence that women who wish to become pregnant after a diagnosis of BC will not have their prognosis directly and adversely affected by pregnancy. However, high-risk BC is associated with a high risk of recurrence, which may suggest that pregnancy should be avoided, albeit not because pregnancy itself is associated with poor outcomes. Thus, the decision to conceive after a BC diagnosis remains a complex and personal decision.
Previous studies have failed to address whether induced abortion may improve the patient’s prognosis, or to specify the optimal time to delay pregnancy after a BC diagnosis [61112]. We found that abortion/miscarriage did not influence the BC outcomes, regardless of the treatment type(s). Thus, induced abortion should not be considered from a therapeutic perspective. Unfortunately, the health insurance database does not include data regarding the child’s health status, and we hope to address this issue in future studies.
The present study has some limitations. First, although we confirmed disease-free status when appropriate for the various comparisons, we could not completely exclude the possibility of healthy-mother bias. Second, the National Health Insurance Service data do not contain complete information regarding recurrence status, although we attempted to infer this event based on changes in the prescribed treatments. Third, we inferred the BC subtypes based on the patients’ prescribed treatments, which may not completely or accurately identify the specific BC subtype.
Nevertheless, we failed to detect a significant association between pregnancy and total mortality after the diagnosis of HR-positive BC. Therefore, these findings may be useful for reassuring patients that pregnancy is safe after a diagnosis of BC, although the optimal interval between the BC diagnosis and pregnancy remains unclear.
 XML Download
XML Download