

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Currently, pancreaticoduodenectomy (PD) is the standard treatment for malignant and benign neoplasms located in the periampullary and pancreatic head regions [1]. Since the first total laparoscopic Whipple operation was performed in the 1990s [2], laparoscopic PD (LPD) remains the most challenging procedure for surgeons that requires extensive resections and difficult reconstructive anastomosis; further, there is a long learning curve for surgeons for them to advance in their laparoscopic skills [3].
The quality of digestive reconstructions, including the reconstruction of hepaticojejunostomy, pancreatojejunostomy, and gastrointestinal anastomosis (GA), are vital factors that contribute to surgical success [4], and are closely related to postoperative complications that have recently been reported as prognostic factors [567]. The principal methods of digestive reconstruction comprise hand-sewn anastomosis (HA) and stapled anastomosis (SA). To save operative time and reduce the difficulty of the operation, SA has been widely used in subtotal stomach-preserving PD in laparoscopy since the stapling instrument was used on the gastrointestinal tract in the 1980s [8]. However, a recent meta-analysis evaluating the outcomes of SA vs. HA in 686 patients undergoing PD revealed a detriment of SA of higher rates of anastomotic bleeding [9]. Besides, the use of SA facilitates the operation, making SA more increasingly accepted in Whipple operation. For these reasons, an approach to optimize SA is urgent and highly demanded, to reduce the incidence of post-PD hemorrhage (PPH), mainly gastrointestinal-anastomotic hemorrhage (GAH).
Recently, we have used a simple skill to improve SA for LPD using a continuous suture to reinforce the stapled line. In order to introduce this reinforced method, we performed a retrospective comparison of the postoperative outcomes with those of SA in LPD.
Go to : 
METHODS
Study population
We retrospectively analyzed patients for whom LPD in Whipple operation was performed by the same surgical team from December 2014 to December 2020 in The First Affiliated Hospital of Chongqing Medical University. The selection criteria for patients included receiving LPD with a side-to-side GA using a linear staple. Moreover, the exclusion criteria were as follows: (1) patients who underwent pylorus-preserving PD, or a total PD; (2) those who underwent total HA; (3) those for whom the procedure was converted to laparotomy; and (4) the first 40 patients receiving LPD by this surgical time. Finally, 139 eligible patients, including the NR group (n = 71) with SA using a continuous suture to repair the defects (NR method) and R group (n = 68) with SA and our reinforced method (R method), were enrolled.
The Ethics Committee of the Chongqing Medical University approved this retrospective study; written informed consents were obtained from all the patients.
Surgical procedures
The 5 trocars were placed in a V-shape, as reported by Zhou et al. [10], as suitable for the body shape of Chinese subjects. Whipple operation was performed. When resection was performed for the common bile duct, gall bladder, pancreas head, part of stomach, and duodenum, Child method was used to reconstruct the digestive tract. After completing an end-to-side pancreaticojejunostomy (duct-to-mucosa) with a stent and an end-to-side hepaticojejunostomy combining the continuous and interrupted sutures, the GA was performed by a side-to-side anastomosis with a linear stapled between the posterior wall of the stomach and the jejunum. In the NR group, a 4-0 polyglactin suture, called the repair line, was used to close the mesenteric defect where staples were inserted using the running full-layer suture. In the R group, a 4-0 polyglactin suture, called the reinforced line, was sewn and reinforced from the posterior wall of the newly-built digestive tract, along with the anastomotic nails in the lumen by the continuous whole layer fashion. To expose the anastomotic nails in the deep and anterior wall of the new digestive tract, the suture was clamped, instead of the intestinal lumen, to tract the suture. After that, the defect was repaired using the same method used for the NR group (Fig. 1). Finally, 2 drainages were routinely placed; one was placed near the pancreaticojejunostomy, and the other was placed near the hepaticojejunostomy.
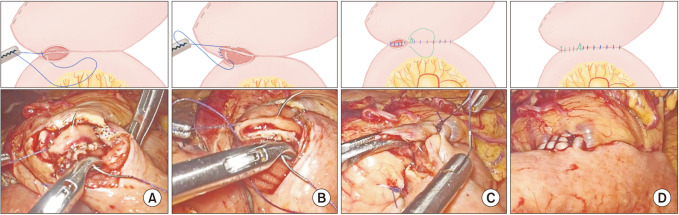 | Fig. 1Illustrations and photographies of the reinforced method in gastrointestinal anastomosis. (A, B) A 4-0 pyloric suture called as the reinforced line (blue line) sewn and reinforced from the posterior wall of the newly-built digestive tract along the anastomotic nails in the lumen by the continuous whole layer fashion; the stitch spacing was about 5 mm, and exposed the anastomotic nails in the deep and anterior wall of new digestive tract by clamping the suture instead of the intestinal lumen to tract the tract. (C, D) The reinforced line was sewn to the outside of the lumen and another 4-0 pyloric suture called as the repair line (green line) was sewn to the anastomosis and fixed with the reinforced line. The repair line was used continuous suturing through the full layer of the intestine to repair the defect of the anastomosis and the stitch spacing was also about 5 mm.
|
Perioperative variables and definitions
We defined the operative time from trocar placement to abdominal closure; the time from enterotomies in the gastric pouch and jejunum to defect closure (cutting the last stitch) in the GA was considered the GA time. The definition, classification and grading standard of postoperative pancreatic fistula (POPF), biliary fistula, delayed gastric emptying (DGE) and postoperative hemorrhage were made according to the previous studies [11121314]. The Clavien-Dindo (CD) grade was used to assess the postoperative complications [15]. Postoperative length of stay (P-LOS) was defined as the number of days from operation to discharge.
Postoperative management
Postoperative examinations and treatments were as identical as previous reports [16]. Treatments of PPH included conservative treatment and surgical intervention. Most patients with PPH could be treated with conservative treatments, including blood transfusion, hemostatic drugs, and infusion of cold normal saline through nasogastric tube (NGT). Hemostasis for patients with severe PPH (grade B or C, hemoglobin reduction of >30 g/L within 24 hours, with significant hypovolemic shock) or for those in whom conservative treatment was ineffective was achieved through gastroscope or reoperation.
Statistical analyses
All the statistical analyses were performed using IBM SPSS 26.0 for Mac (IBM Corp., Armonk, NY, USA). The normality of the variables was assessed. Data are expressed as mean± standard deviation values or median (the 25th to 75th percentile) values. Analysis of variance was performed to compare the normally distributed variables. The nonparametric Mann-Whitney U-test was used for skewed continuous variables, while the chi-square and Fisher exact tests were used for categorical variables. Univariate logistic regression model was fit to evaluate factors associated with GAH. A P-value of <0.05 was considered to indicate statistical significance.
Go to :
RESULTS
Comparison of the factors associated with gastrointestinal-anastomotic hemorrhage
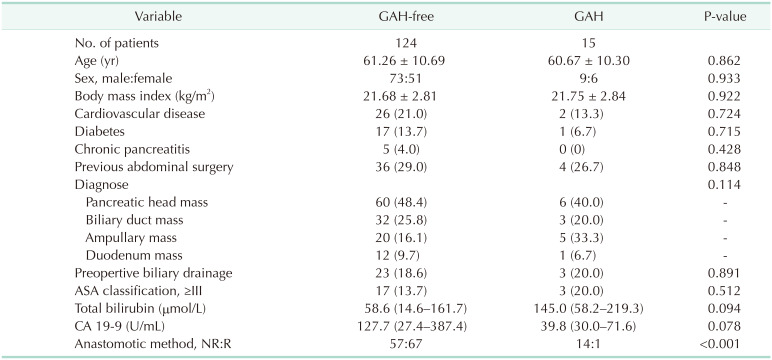
From December 2014 to December 2020, 139 eligible patients were enrolled in the study, including 71 patients who underwent conventional linear SA and 68 for whom the reinforced method of SA was used. Patients were divided into GAH-free and GAH groups based on the occurrence of GAH. The clinical characteristics and anastomotic methods of the 2 groups are shown separately in Table 1. With respect to the clinical characteristics, patients in both groups were matched by age, sex, body mass index (BMI), cardiovascular disease, diabetes, chronic pancreatitis, previous abdominal surgery, preoperative-diagnosis, preoperative biliary drainage, preoperative American Society of Anesthesiologists (ASA) classification ≥ III, preoperative total bilirubin (TBil), and preoperative CA 19-9. There were no significant differences in these parameters. However, compared with the GAH-free groups, patients with GAH were more likely to be performed R method (P < 0.01).
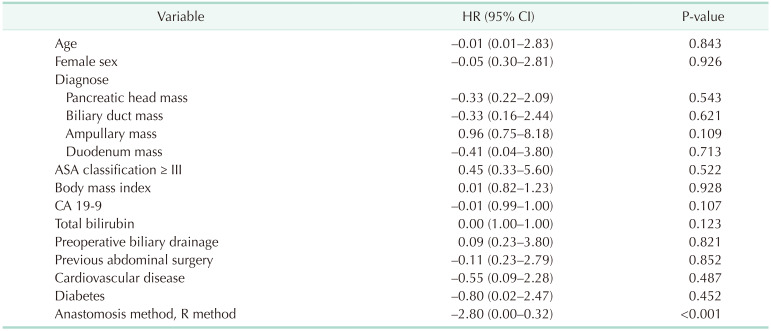
To identify the associated factors of GAH, univariate logistic regression analyses were performed, and the age, sex, preoperative diagnosis, ASA classification ≥ III, BMI, CA 19-9, TBil, preoperative biliary drainage, previous abdominal surgery, cardiovascular disease, diabetes, and anastomotic method of patents were included (Table 2); and, no baseline factor was associated with the likelihood of GAH. Only the anastomosis method was associated with it, and the R method could significantly reduce the odds of GAH compared with the NR method.
Comparison of the anastomotic methods
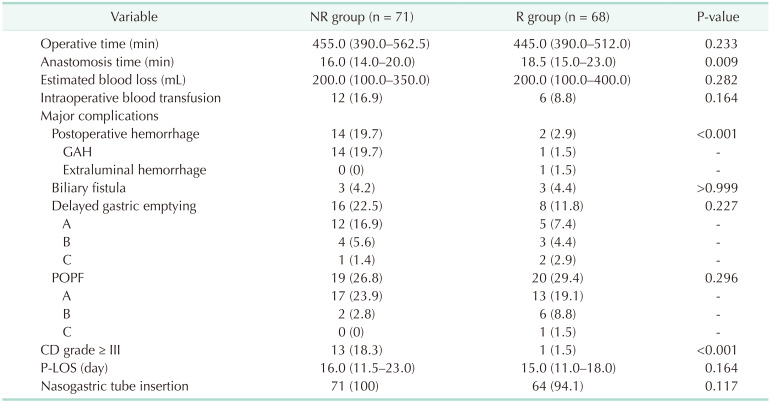
The operative parameters, the major complications, and P-LOS were compared between the R group and NR groups (Table 3). No considerable differences were observed in the estimated blood loss, intraoperative blood transfusion, the NGT insertion, and the P-LOS. The anastomotic time was significantly longer in the R group than in the NR group (18.5 [15.0–23.0] minutes vs. 16.0 [14.0–20.0] minutes, respectively; P = 0.009). While the operative times of the R and NR groups had no statistical difference (445.0 [390.0–512.0] minutes vs. 455.0 [390.0–562.5] minutes, respectively; P = 0.233), suggesting that an increase of several minutes in GA was not significant for the total operative time. As for the major complications, there were no statistically significant differences in the rate of biliary fistula, DGE, and POPF. However, the incidence of postoperative hemorrhage and postoperative complications whose CD grade ≥ III were significantly higher in the NR group compared with the R group. Especially for GAH, 18.31% of patients from the NR group suffered from intraluminal hemorrhage, while the percentage fell to 1.47% in the R group, whose difference was significant.
Go to :
DISCUSSION
The purpose of this paper was to figure out the potential factors of GAH and evaluate the efficacy and safety of our reinforced method against the normal gastroenterostomy operation of LPD. The most significant finding was the reduced incidence of GAH and CD grade ≥ III complications using our reinforced method. Although the time for GA used in the NR group was considerably shorter than that used in the R group, the total operative time of the 2 groups was the same.
Currently, intracorporeal digestive anastomosis is increasingly used in digestive reconstruction for its benefits in shorter wound length, earlier digestive function recovery, less postoperative analgesia, lower pain score, and fewer complications (paralytic ileus and gastrointestinal bleeding) [1718]. The intracorporeal suturing procedure is harder than extracorporeal anastomosis. Under this circumstance, SA has gained popularity in the reconstruction of the digestive tract because it is less time-consuming and requires a lower skill level than HA [19]. In operations, such as LPDs that are highly time-consuming, skill-demanding, SA is very advantageous. However, some studies demonstrated that SA is responsible for more anastomotic hemorrhages [92021]. These results are similar to our findings in which different staplers were used. During the time of learning how to carry out LPD, a reinforced method was developed to alleviate the postprocedure hemorrhage most likely caused by the SA.
PPH is still a major complication, most PPHs are intraluminal, often shown as hematemesis, melena, and hemorrhagic fluid in NGT [14]. Vâlcea et al. [22] reported that hemorrhages from hepaticojejunostomy and pancreaticojejunostomy are rare and that most of the intraluminal bleedings are GA. Besides, with the use of SA, the incidence is growing higher than HA. Therefore, we focused on PPH from GA, and finally, a reinforced method to reduce GAH was found. We used our method to reinforce the stapled line in 68 patients, and only 1 GAH case was observed in whom hemorrhage was treated by conservative treatments. Also, 1 case of extraluminal hemorrhage showing hemorrhagic fluid in the abdominal drainage tube was treated by using hemostatic drugs and blood transfusion treatments. In contrast, GAHs were observed in 14 patients in the NR group. These results indicate that GA using our reinforced method could be accepted as a better choice for lowering the incidence of GAH. GA is also widely conducted in gastrectomy for gastric cancer and gastroduodenal ulcer, while the incidence of postoperative bleeding after these surgical procedures ranges from 0.6% to 4.4% [23], representing a percentage that is extremely low as compared to that of LPD that is 20.2% [24]. Furthermore, a meta-analysis demonstrated that reinforcing the staple line had no significant advantage in laparoscopic sleeve gastrectomy [25]. Postoperative hemorrhage in PD may be more abundant because left gastric vessels, left gastroepiploic vessels, and short gastric vessels of remnant stomach and GA tract are kept in the procedure to ensure sufficient blood supply, whereas, almost of the blood-supplying vessel in the stomach are ligated in gastrectomy.
Studies revealed SA has an advantage in DGE over hand-sewn [926]. To avoid anastomotic edema and edema causing DGE, we clamped the suture instead of intestinal tube to help in exposing the stapled line. Also, the incidence of DGE being similar between the 2 groups may show that sewing in one more layer without clamping the intestinal tube would not increase the rate of DGE.
The CD system has been widely used in the evaluation of surgical complications owing to its simplicity and feasibility. Since established in 1992 [27], and CD grade ≥ III complications are associated with operative safety [3]. In our study, CD grade ≥ III complications mainly occurred in the NR group, with only 1 complication associated with grade C POPF. A previous study has reported the same result [28]; while the incidence of POPF was high (28.10% in our research), most POPF could be treated by drugs, such as somatostatin, and should be classified into CD grade < III complications. In contrast, PPH was more harmful in terms of patient complications and requiring emergency treatments. Further, 63.6% of PPHs were classified as CD grade ≥ III complications. The significant difference in the percentage of CD grade ≥ III complications in the 2 groups (P < 0.01) suggested the feasibility of our method in reducing severe complications.
There are certain limitations of this study. Our study is based on the retrospective data from a single institution and employed a relatively small patient population. In contrast, the follow-up time was not long enough to compare the late complications related to anastomosis, such as gastrointestinal stricture, marginal ulcer of anastomosis, and gastrointestinal perforation, between the 2 groups. We also have limits in the absence of comparing the postoperative complications between the HA group and the R group.
Thus, our data suggest that this reinforcement method is feasible and effective in terms of operation and reduction in the postprocedure hemorrhage rate.
Go to :
 XML Download
XML Download