

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Papillary thyroid cancer (PTC) constitutes more than 90% of thyroid cancers, which are the most widespread neoplasms of the endocrine system. Despite the biological behavior and good prognosis, lymph node metastasis (LNM) is not uncommon in PTC, and the presence of LNM is the most significant determinant of recurrence [1]. The basic treatment of PTC where there is LNM is full resection of the primary tumor and regional LNM [2]. Depending on the level of lymphatic spread, central or modified radical lymph node dissection (MLND) are the treatment options used in surgery [3].
Some studies have reported that insufficient LN dissection has a negative effect on prognosis by causing recurrence [45]. Furthermore, the localization of important vascular and neurological structures in the surgical region can cause life-threatening or some permanent neurological injuries for the patient, which may lead to various medicolegal problems for the physician [67]. This may be caused in particular by inexperienced surgeons performing incomplete LN dissection. In the last 15–20 years, it has been reported that intraoperative neuromonitoring (IONM) [89], which is often used during thyroid cancer operations and neck dissections, has decreased temporary or permanent complications which may develop associated with identification of not only the recurrent laryngeal nerve but also of significant neural structures such as the phrenic nerve [10] and spinal accessory nerve [11] located in the neck dissection area. However, there is no study in literature that has evaluated the effect of neuromonitoring on the number of LNs excised in patients undergoing CLND or MLND.
The aim of this study was to evaluate the effect of neuromonitoring on the number of LNs removed when performed in patients receiving neck dissection.
Go to : 
METHODS
Approval for the study was granted by the Ethics Committee of Ankara Nomune Training and Research Hospital (No. E-17-1475). All procedures were applied in compliance with the 1964 Helsinki Declaration and its later amendments, and the institutional and/or the national research committee ethical standards. This retrospective study was conducted between January 1, 2012 and January 5, 2020 in the Department of General Surgery at Ankara City Hospital (Ankara, Turkey). Data were collected from patient records, computer system records, operating notes, clinic follow-up forms and the anamnesis related to surgical indications, intensive care unit forms, and the surgical procedures applied. Written informed consent for surgical procedures was obtained from all patients preoperatively.
The patients included in the study were those aged >18 years, diagnosed with PTC with fine-needle aspiration biopsy (FNAB), who were evaluated with neck ultrasonography, neck CT, MRI, or PET-CT to determine the disease spread preoperatively, and the presence of metastatic LNs in central or lateral LNs was verified with FNAB in patients determined with suspicious LNs in central or lateral zones, and who had undergone CLND or MLND in addition to total thyroidectomy by the same surgical team, and then continued treatment and follow-up postoperatively.
Inclusion or exclusion criteria
Patients were excluded from the study if they were aged <18 years, if surgery was performed because of PTC but LN dissection could not be applied, if they were determined to have recurrence following previous neck dissection, or if they had not continued with regular follow-up or full medical records were not available. Of a total of 756 patients identified who underwent total thyroidectomy because of PTC, 526 were excluded as LNM was not determined, 26 as their medical records were incomplete, and 38 as follow-up was interrupted; thus, a final total of 166 patients were included in the study.
CLND (zone VI) was applied to all the patients, and lateral neck dissection (IIa, III, IV, and Va, b) was performed additional to CLND in 55 patients. All the surgical procedures were applied by experienced endocrine surgeons with a primary method. Pathology specimens were evaluated by a pathologist experienced on the subject of endocrine surgery and, taking the LN stations into consideration, the total number of LNs, reactive LNs and metastatic LNs were determined separately.
The demographic and clinicopathological data collected from the medical records were recorded, including the patient age, the largest tumor diameter, multifocality and multicentricity, temporary or permanent nerve damage, the development of temporary or permanent hypocalcemia, the total number of LNs, and total numbers of reactive and metastatic LNs. The patients were separated into 2 groups according to whether or not IONM was performed. The monitoring group comprised 76 patients receiving neuromonitoring; and the non-monitoring group, 90 patients who did not receive neuromonitoring.
Surgical technique
All the operations were performed under general anesthesia by an experienced endocrine surgeon with an annual surgery volume of >100 operations and >10 neck dissections. In all the protocols, premedication was administered as intravenous midazolam, anesthesia induction was provided with fentanyl, thiopental, and suxamethonium, and maintenance with endotracheal intubation and sevoflurane. The IONM group was not administered any muscle relaxant agent. Standard cervicotomy was performed in all patients. In patients determined preoperatively with central zone LN positivity, CLND was performed additional to total thyroidectomy; and for patients determined to have LN positivity in a lateral neck station with FNAB, type 3 MLND dissection was performed.
In all the patients where IONM was applied, the Dr. Langer Medical GmbH (Am Bruckwald, Waldkirch, Germany) was used, which includes surface electrodes integrated with a 7.0–7.5-mm diameter endotracheal tube. The procedure was applied according to the International Neural Monitoring Study Group guidelines published in 2011. The surgical procedure was started on the side where malignancy was determined. After slight mobilization of the lobe, a vagus signal (V1) was obtained with stimulation of 1–2 mA. In patients with no response to the stimulus, the algorithm stated in the guidelines was applied to discount the possible residual effect of muscle relaxant or misplacement of the endotracheal tube. Before visual identification of the recurrent laryngeal nerve, the nerve was mapped through stimulation of 1–2 mA. In patients where a positive response (E1) was obtained, visual identification was made through nerve dissection, and nerve integrity was evaluated with repeated stimulations throughout lobe mobilization and removal, and CLND on the tumor side. Following completion of resection and CLND, if there were no metastases in lateral LNs, the total thyroidectomy and CLND procedure was completed by repeating the procedures applied to the tumor side to the opposite side lobe.
In addition to CLND, LNs along the internal jugular vein (level II, III), and in the posterior triangle (level V), were removed in patients receiving type 3 MLND. With both visualization and determination with IONM, the lymphatic dissection was completed by protecting neural structures such as the 11th cranial nerve and the phrenic nerve located in the dissection area.
After nerve stimulation with 1–2 mA, complete absence of the stimulation curve was defined as the length of stay, and a decrease of >50% of the baseline value in the nerve stimulation response was accepted as a significant drop in the signal.
The metastatic LN ratio (MLNR) was accepted as the ratio of metastatic LNs removed to the total LNs.
Statistical analysis
Data obtained in the study were analyzed statistically using SPSS for Windows ver. 17.0 (SPSS Inc., Chicago, IL, USA). Conformity of the data to normal distribution was assessed with the Kolmogorov-Smirnov test. Categorical data were stated as number and percentage; and quantitative data as mean ± standard deviation (SD) and median and range values. Paired groups were compared using the Student t-test or the Mann Whitney U-test, depending on the conformity to normal distribution. As complete lymphatic dissection was a factor effective in the development of recurrence, Pearson and Spearman correlation analyses were used to determine the risk factors for LNM and recurrence, and univariate and multivariate regression analyses were applied to calculate the level of contribution and relative risks to the development of LNM of the parameters determined to be correlated. Optimal cutoff values of MLNR determining the development of recurrence were determined with receiver operating characteristic (ROC) curves. The area under the curve (AUC) was stated in a 95% confidence interval (CI). A P-value of <0.05 was accepted as statistically significant.
Go to :
RESULTS
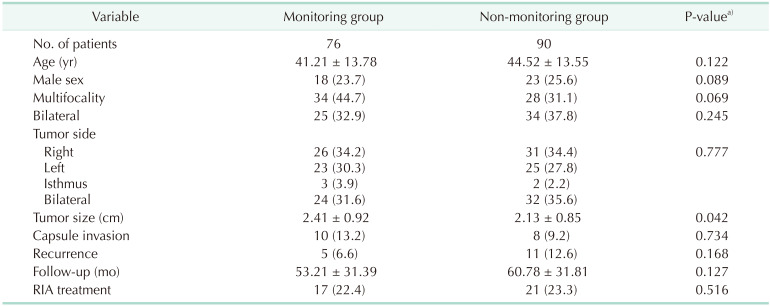
The mean age of the patients was 41.21 ± 13.38 years in the monitoring group and 44.52 ± 13.55 years in the non-monitoring group (P = 0.122). No significant difference was determined between the groups in respect to sex (P = 0.089) and tumor localization (P = 0.777). The mean follow-up period was over 50 months in both groups. There was no difference between the 2 groups in terms of follow-up times (P = 0.127). When the patients were evaluated in terms of radioactive iodine ablation (RIA) treatment, it was seen that 21 patients in the non-monitoring group and 17 patients in the other group were treated with RIA. There was no significant difference between the groups (P = 0.516). The demographic variables of the groups are shown in Table 1.
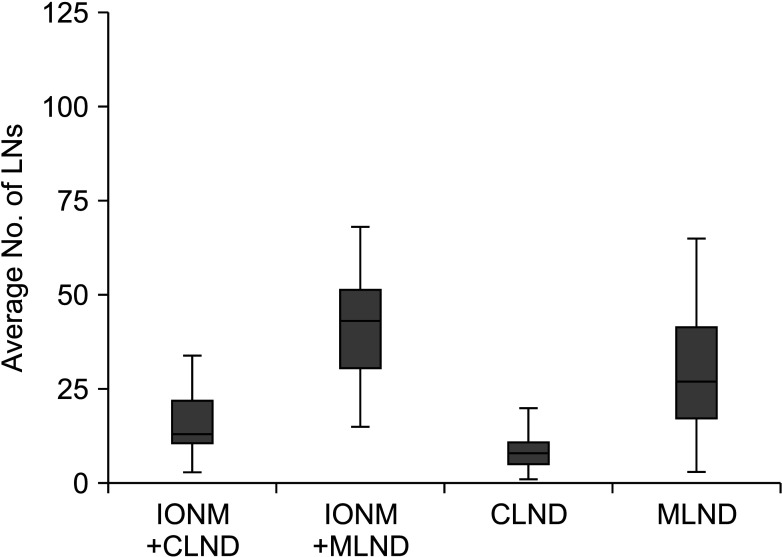
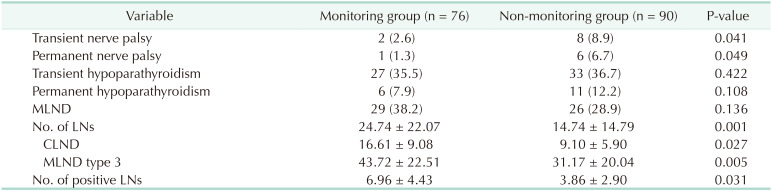
MLND was seen to have been performed at similar rates in both groups (P = 0.136). When the groups were evaluated in respect to surgical results, temporary (P = 0.041) and permanent (P = 0.049) nerve damage was observed to be significantly less in patients receiving monitoring. The number of LNs dissected was observed to be significantly higher in the monitoring group (P = 0.001) (Fig. 1), and no significant difference was seen between the groups in respect to the number of positive LNs (P = 0.031). When the 2 groups were evaluated according to the application of CLND and MLND, there was seen to be a significantly higher number of excised LNs in both the CLND material (P = 0.027) and the MLND material of the patients in the monitoring group (Fig. 2). The surgical results are shown in Table 2.
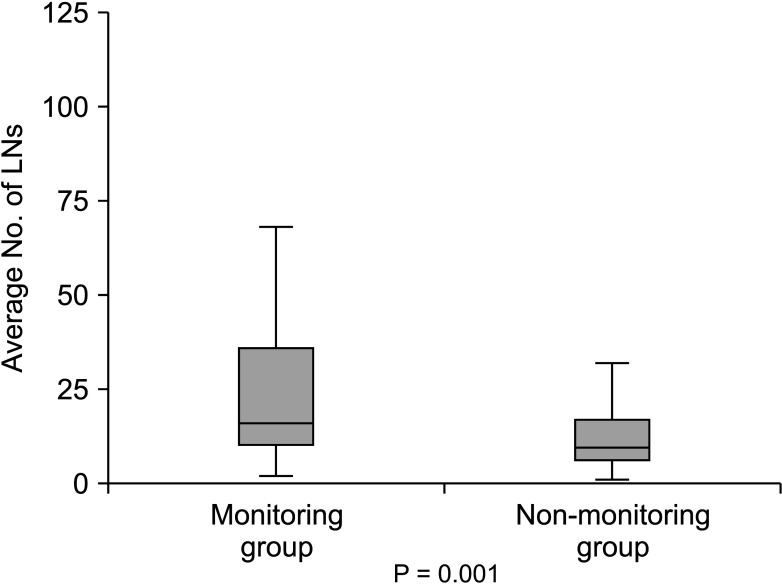 | Fig. 1The number of lymph nodes (LNs) dissected was observed to be significantly higher in the monitoring group.
|
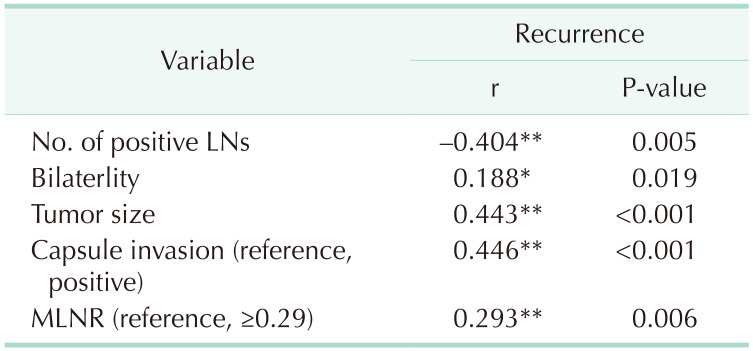
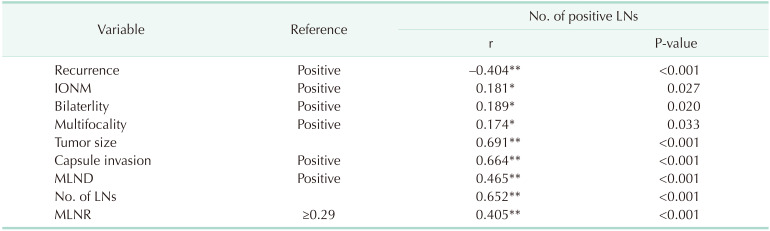
As the importance of the number of dissected metastatic LNs on the development of recurrence has been shown in previous studies, the factors related to metastatic development and recurrence were evaluated with correlation analysis. There was seen to be a negative correlation between the number of positive LNs dissected and recurrence (r = –0.404, P = 0.005), and a positive correlation between high MLNR and recurrence (r = 0.293, P = 0.006) (Table 3). When the factors related to the number of positive LNs dissected were evaluated, the use of neuromonitoring during surgery was seen to have a weak positive correlation with the number of positive LNs excised (r = 0.181, P = 0.027) (Table 4).
In the ROC analysis, a cutoff value of ≥0.29 for MLNR was seen to constitute a serious risk for the development of disease recurrence (AUC ROC, 0.886 ± 0.030 [95% CI, 0.826–0.946]; P < 0.001; sensitivity of 68.8% and specificity of 85.2%) (Fig. 3).
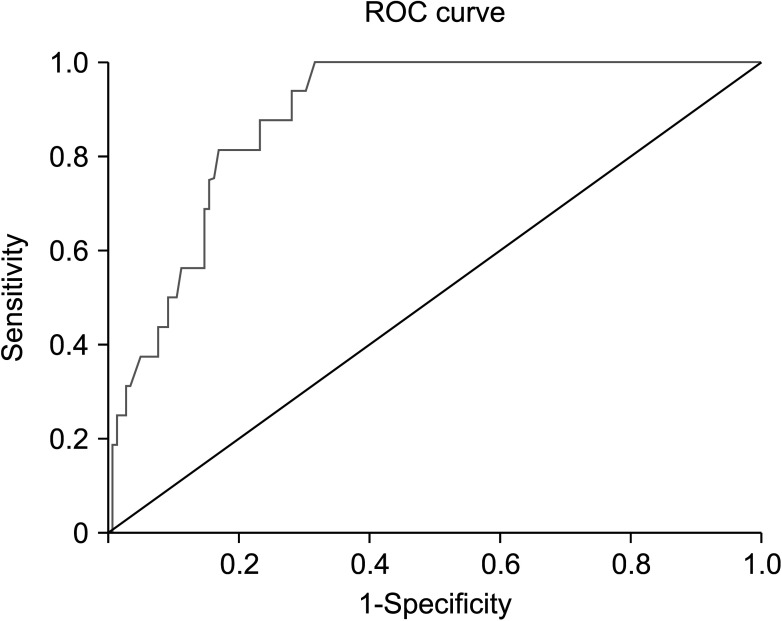 | Fig. 3In the receiver operating characteristic (ROC) analysis, metastatic lymph node ratio was seen to constitute a serious risk for the development of disease recurrence. Area under the curve ROC, 0.886 ± 0.030 (95% CI, 0.826–0.946); P < 0.001; sensitivity of 68.8% and specificity of 85.2%. Diagnal segments are produced by ties.
|
When the parameters determined to be associated with recurrence were evaluated with binary logistic regression analysis, not using IONM was seen to contribute to recurrence development 4.18-fold (95% CI, 1.190–6.570; P = 0.043), and the most significant contribution was seen to be the application of MLNR (odds ratio, 7.42; 95% CI, 2.467–15.374; P = 0.006) (Table 5).

Go to :
DISCUSSION
Although it has been shown in many previous studies that IONM in patients receiving neck dissection had reduced nerve damage, there has been no study that has examined the effect of IONM on the number of excised LNs [89]. It has been reported in the literature that LNM does not affect survival, but MLND in high-risk patients has been shown to reduce recurrence [12]. The aim of this study was to evaluate the effect of IONM on the total number of excised LNs and the number of metastatic LNs. As this is the first study to have evaluated this subject, it can be considered to make a significant contribution to the literature. To briefly summarize the results of the study, there was seen to not only be a decrease in temporary and permanent nerve damage (P = 0.041 and P = 0.049) in the group receiving IONM but also a significant increase in the total LNs excised (P = 0.001) and the number of metastatic LNs (P = 0.031).
In recent years, IONM has become a more widely used procedure because of various advantages in thyroid surgery [89], and it has been reported to have been used in 40% of all thyroid surgeries in the United States, and in up to 90% in Germany [13].
However, conflicting results have been reported about the effect on the prevention of postoperative nerve damage [141516]. Some studies have stated that the application of IONM makes no difference in the intraoperative identification of recurrent laryngeal nerve [1718], while in a recent group study, it was emphasized that the device could be helpful in reducing the risk of nerve damage [1419]. Thyroid surgery is known to encompass a broad range from benign causes to malignant causes, which can vary from limited thyroidectomy to central or lateral LN dissection. A previous study reported that the incidence of nerve damage seen could show a difference depending on the extent of the surgery [3]. Although nerve damage can develop associated with traction or thermal causes, it has been reported that in patients where neck dissection is performed, there is a higher risk associated with invasion of metastatic LNs [20]. Similarly, Ahn et al. [21] emphasized that nerve damage was increased in patients receiving neck dissection. In a study of 1,273 cases receiving CLND due to thyroid cancer, Liu et al. [22] reported nerve damage at the rate of 3.8%. When the study results were evaluated in respect to temporary and permanent nerve damage, it was seen that permanent nerve damage developed in 1.3% of the IONM group, and this rate was seen to be 6.6% in patients where the nerve was determined visually. The study results were consistent with findings in literature in respect to rates of nerve damage, and that the use of IONM would significantly reduce nerve damage (P = 0.041 and P = 0.049, respectively).
Although the main aim of this study was not to evaluate factors affecting LNM, as there is information that complete excision of metastatic LNs has a positive effect on recurrence, the factors affecting LNM were evaluated in this study to more clearly understand the importance of the study. So et al. [23] reported that tumor localization, capsular invasion, patient age, tumor size, and multifocality were predictive factors for LNM. In addition to the study by So et al. [24], a recent meta-analysis reported that bilateral localization and lymphovascular invasion are factors with an effect on LNM. The current study results showed a relationship between LN positivity and the variables of tumor size (r = 0.691, P < 0.001), the presence of capsule invasion (r = 0.664, P < 0.001), and the presence of bilateral tumor (r = 0.189, P = 0.020). In this respect, the results were found to be consistent with the literature.
A recent study showed that although LNM did not affect patient survival, it reduced the risk of MLND recurrence in high-risk patients [12]. In a recent questionnaire study that evaluated the use of IONM by endocrine surgeons, the extent of surgery was reported by the surgeons to be affected by the use of IONM. However, when this extent was due to not obtaining a signal on one side during surgery rather than the number of LN excised, it showed a limiting effect on intervention to the other lobe [3]. In contrast, in the current study, as the surgeon was sure of nerve damage on the device, the surgeon evaluated whether or not to make a more extensive LN excision and significant results were obtained. The increase in the total number of LNs excised in the current study was seen to be positively correlated with the increase in the number of positive LNs (r = 0.652, P < 0.001). As the use of IONM was the probable reason for the increased number of LNs removed, it was also the reason for the increased number of positive LNs excised, thereby showing a reduction in recurrence (r = –0.404, P < 0.001). This result can be explained by the effect of MLND in reducing recurrence as stated in the literature. Another significant parameter evaluated for the first time in the current study is MLNR. The study results showed a positive relationship between the development of recurrence and an increase in the MLNR to the total number of excised LNs (r = 0.293, P = 0.006). Although this does not seem to be consistent with the negative relationship between recurrence and an increase in excised metastatic LNs, it complements the data. Clinical experience has shown that during the follow-up of these patients, the number of positive LNs removed increases and the remaining metastatic LNs decrease but when the remaining LNs are ≥0.29 of this ratio, there is a serious risk of the development of recurrence, probably due to micrometastases (AUC ROC, 0.886 ± 0.030 [95% CI, 0.826–0.946]; P < 0.001; sensitivity of 68.8% and specificity of 85.2%). In addition, in the current study, the number of positive LNs, tumor size, capsule invasion, and high metastatic LN rate were found to be associated with recurrence. However, when both groups were examined, it was thought that more LN dissection was performed in the monitoring group, better clearing of metastatic LNs, and possibly fewer metastatic LNs left, resulting in lower recurrence rates.
There were some limitations to this study, primarily the retrospective design. However, as data has been kept electronically for more than 10 years in our clinic, data loss was not thought to have constituted a serious problem in the study. Also, due to the retrospective design, the MLND rate in the IONM group may have been greater, but there was no difference between the groups when evaluated statistically. Strong aspects of the study can be said to be that as all the surgical procedures were performed by surgeons experienced in endocrine surgery, the effect of experience in LN excision was reduced to a minimum, thereby preventing any bias in favor of IONM.
In conclusion, the results of this study clearly showed that the application of IONM during neck dissection not only prevents nerve damage but also contributes to the prevention of the development of recurrence by increasing the number of LNs and metastatic LNs excised.
Go to :
 XML Download
XML Download