

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19) first emerged in December 2019 in China. The World Health Organization declared it a global pandemic in March 2020. In South Korea (“Korea” from here on), the first confirmed case was on January 20, 2020. Through group infections (e.g., Shincheonji church and Daenam hospital) the number of people who contracted the disease between February and March 2020 increased sharply.1 During this period, fear and anxiety due to the pandemic and excessive stress caused by the restriction of social activities were heightened in society.23 Additionally, the spread of “fake news” related to COVID-19 led to increased public anxiety.4 The Korean government responded quickly and effectively to control COVID-19; however, the mental health of the population was already damaged.5
Specifically, suicide is an important issue that needs to be considered during epidemics. Previous studies6789 on mental health during epidemics (e.g., severe acute respiratory syndrome and Ebola virus outbreaks) showed worsened mental health, such that post-traumatic stress, anxiety, and depression were associated with suicide.10 Moreover, to prevent the spread of COVID-19, regulations to enforce social distancing such as lockdowns and business restrictions were implemented. The business restrictions could later lead to economic crises,11 which are a risk factor for increased suicide behaviors or suicide mortality.1012 However, it is not clear whether the COVID-19 pandemic has an impact on suicide.
A majority of recent studies1314151617 found that there was no increase in suicide rates during the COVID-19 pandemic, while one study from Japan18 showed an increase in suicide rates in the second half of 2020 compared to previous years. However, previous studies that have investigated the relationship between COVID-19 and suicidal behavior have mostly considered the general population131415161718; only a few of them have considered persons directly affected by COVID-19 (e.g., those confirmed positive for COVID-19). This group of people is expected to be more vulnerable to mental health problems or suicide due to fear, anxiety, social isolation, social stigma, and discrimination.219 Furthermore, some recent studies2021 have recommended that patients with pre-existing psychiatric disorders before COVID-19 should be monitored more carefully since they have shown worsened mental health conditions during the pandemic.
In line with the results from previous studies, the current study aimed to investigate the impact of the COVID-19 pandemic on self-injurious behavior (SIB) of the COVID-19 risky groups. The SIB includes non-suicidal self-injury (NSSI) and suicide attempts depending on the presence or absence of suicidal intent.22 One previous study23 indicated that those with a history of suicide attempt or NSSI are more at risk for suicide mortality (about 30%) compared to the general population. Therefore, the current study investigated SIB (i.e., suicide attempt and NSSI) during COVID-19 pandemic of COVID-19 risky groups. In this study, we investigated the SIB trend by COVID-19 subgroups (i.e., positive for COVID-19 test, negative for COVID-19 test, and control) during the short-term period of the COVID-19 outbreak using the National Health Insurance Service (NHIS)-COVID-19 cohort data. Furthermore, we examined whether the trend of SIB rate during the COVID-19 pandemic was significantly different between those with and without pre-existing mental disorders before the pandemic.
METHODS
Data source and study design
The NHIS-COVID-19 database was the source of data. The NHIS-COVID-19 database cohort-linked data from two organizations: the NHIS and the Korea Disease Control and Prevention Agency (KDCA). KDCA provided data regarding persons who tested positive (or negative) for COVID-19 from January 1 to May 31, 2020. NHIS provided data regarding persons who did not take the COVID-19 test. Stratified random sampling by age, sex, and place of residence was used to extract data from NHIS. The number of persons who did not take the COVID-19 test was 15 times the number of confirmed COVID-19 cases. The cohort data included demographic information, national health screening data, and medical history for the past five years, of all persons. We only included data of persons aged > 20 years. From these, we classified persons into three groups: 1) tested positive for COVID-19, 2) tested negative for COVID-19, and 3) not tested for COVID-19. Persons who did not test for COVID-19 were considered the control group.
Measure
Monthly data regarding COVID-19 confirmed cases were validated via KDCA. Since the data is comprised of health insurance claims data and registry data, we have classified suicide attempt and NSSI using ICD-10 codes. Suicide attempt was classified based on the ICD-10 code for intentional self-harm (X60–X84) and NSSI was classified by the ICD-10 code for probable intentional self-harm (ICD-10: S61.9, T43, T50.9, T52, T54, T58, T60, T65.8, T65.9, W32, W33, W34, W75, W76, Y10–Y34, R09.0, W13–W19) used in a previous study.24 Pre-existing mental disorders were defined as having a diagnostic code for mental and behavioral disorders (ICD-10 code F00–F99) at least once within 1 year before the COVID-19 pandemic.
Statistical analysis
We calculated the monthly SIB rate from January 2019 to May 2020, by dividing the number of people who showed SIB by the total number of people in each month. Additionally, from January 2020, the monthly SIB rate for each COVID-19 subgroups (i.e., positive for COVID-19 test, negative for COVID-19 test, and control) was calculated. Moreover, among those who were tested for COVID-19, we have calculated the monthly SIB rate of those with and without pre-existing mental disorder. Furthermore, moderated regression analysis was utilized to examine the statistical difference of SIB trend between COVID-19 subgroups and with and without pre-existing mental disorder. P values less than 0.05 were deemed significant, and all statistical analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
A total of 328,373 persons were included in this study, of which 145,758 were men and the rest, women. A total of 212,678 persons were tested for COVID-19 between January 1 and May 31, 2020, with 7,713 of them testing positive. A total of 115,695 persons included in this study did not take any COVID-19 test and were the control group of this study. A total of 73,097 persons included in this study had pre-existing mental disorders before the onset of the COVID-19 pandemic (Table 1).
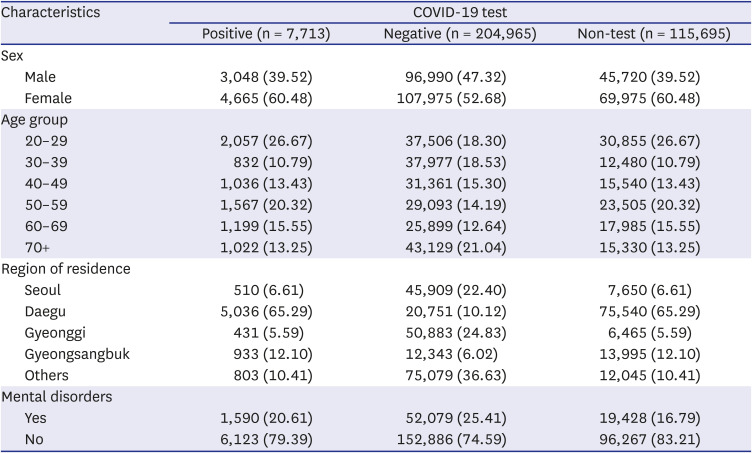
Table 1
Baseline characteristics of the study population
![]()
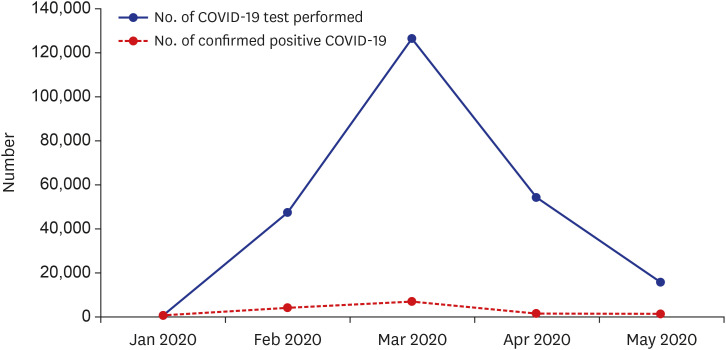
Fig. 1 shows the monthly frequency of COVID-19 tests and COVID-19 confirmed patients from January 1 to May 31, 2020. As illustrated, the frequency of the COVID-19 tests steeply increased until March, and then showed a decreasing trend from April.
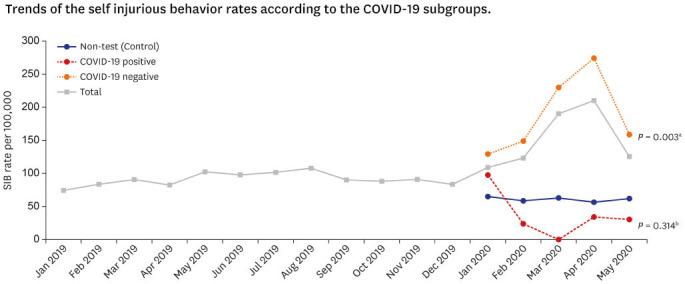
The trends in SIB rates between January and May 2020 among the total study population are shown in Fig. 2. The figure shows the SIB rates by each COVID-19 subgroup (i.e., positive for COVID-19 test, negative for COVID-19 test, and control). Persons who tested negative showed a large increase (P = 0.003) in SIB rates from January to April 2020, compared to those who were not tested for COVID-19 (control group). Those who tested positive showed a decreasing trend, but its trend was not statistically different compared to the control group (P = 0.314). These patterns of SIB rates were similar for both men and women. The comparison of SIB rates between COVID-19 subgroups is shown in Supplementary Table 1. Furthermore, we compared the trend of SIB rate between groups with and without pre-existing mental disorders among persons who were tested for COVID-19—a high-risk group for SIB. Although persons with pre-existing mental disorders had higher SIB rates during the study period, the trend between those with pre-existing mental disorders and without pre-existing mental disorders did not show a statistical difference (P = 0.137) during the COVID-19 pandemic in both males and females (Fig. 3). The comparison of SIB rates of those with and without pre-existing mental disorders are shown in Supplementary Table 2.
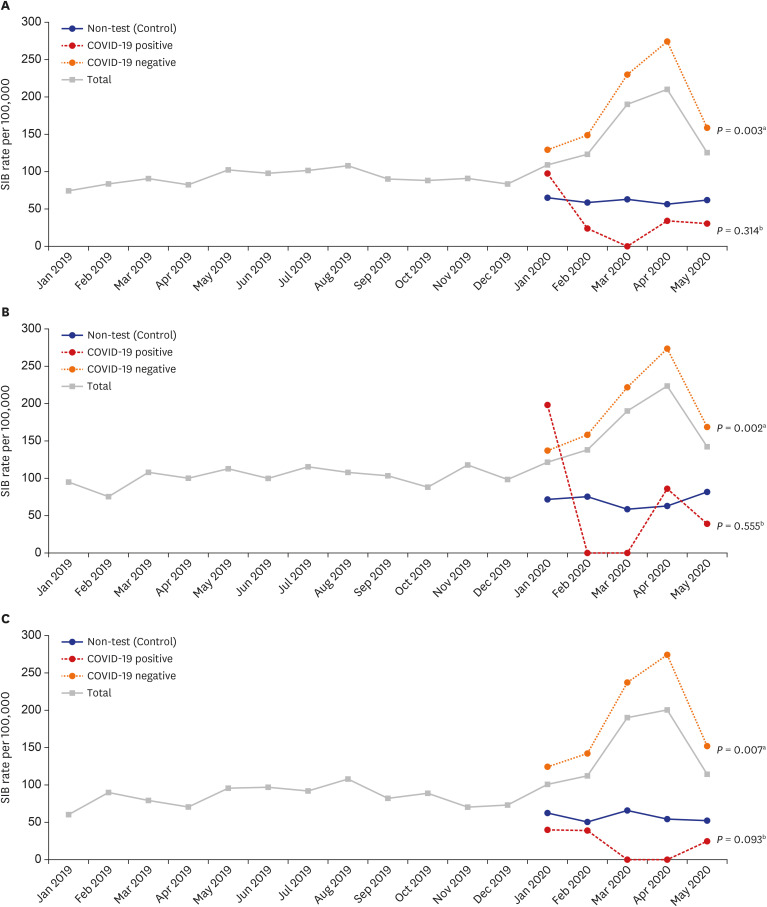
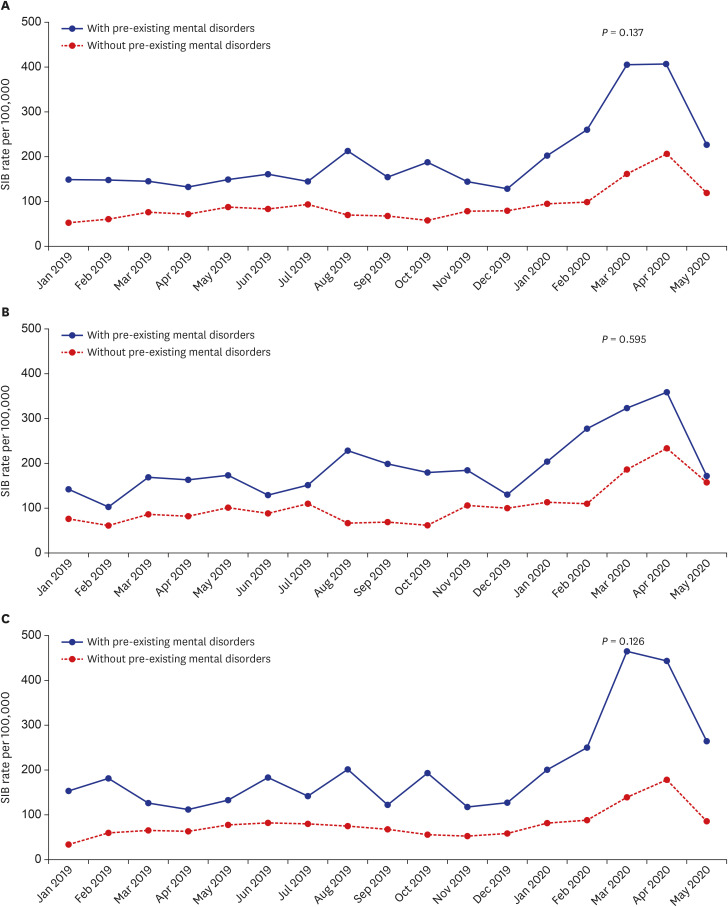
Fig. 2
Trends of the SIB rates according to the COVID-19 subgroups. (A) Total, (B) male, and (C) female.
SIB = self-injurious behavior, COVID-19 = coronavirus disease 2019.
aP values for difference of trend in SIB rate between COVID-19 negative and non-test (control) during the COVID-19 pandemic; bP values for difference of trend in SIB rate between COVID-19 positive and non-test (control) during the COVID-19 pandemic.
![]()
Fig. 3
Trends of the SIB rates according to groups with and without pre-existing mental disorders among those who received the test for COVID-19. (A) Total, (B) male, and (C) female. P values for difference of trend in SIB rate between groups with and without pre-existing mental disorders during the COVID-19 pandemic.
SIB = self-injurious behavior, COVID-19 = coronavirus disease 2019.
![]()
DISCUSSION
The current nationwide COVID-19 cohort study investigated the SIB rate of risky groups during the first peak of the COVID-19 pandemic. In whole, COVID-19 peaked in March and the SIB rate sharply increased in April. This suggests the association between COVID-19 test and SIB during the COVID-19 pandemic. During the initial phase of COVID-19, people who have been tested for COVID-19 were those who were suspected of contacting or carrying the infection. These individuals heavily suffered from isolation by quarantine, social stigma and discrimination which in turn could aggravate their psychosocial problems (e.g., acute stress disorder, depression, insomnia, anger, and post-traumatic stress disorder2325) that are associated with suicidal bahavior.10 An interesting fact is that the number of COVID-19 tests peaked in March and the suicide attempt rate sharply increased in April. This shows that there was a month delay between the time of COVID-19 test and suicide attempt. This result is in line with a previous study26 which studied the association between influenza epidemic and suicide mortality rate. This study found that suicidal mortality has significantly increased up to 2 months after being diagnosed with the novel influenza. The authors suggest that lag between diagnosis and suicide mortality could be due to the window time between exposure to influenza and clinical symptoms and the socio-economic problems. For COVID-19, the lag may have been due to the window time between COVID-19 test and various psychosocial problems such as stigma, financial problems, and discrimination.21119 This indicates that it is important for the government to provide continuous intervention to those who have been tested for COVID-19.
When the suicide attempt trend was compared between groups (COVID-19 positive, COVID-19 negative, and control [i.e., non-test]), COVID-19 negative showed an increasing suicide attempt trend compared to the control group. Also, the confirmed group showed a decreasing suicide attempt trend but not statistically significant compared to the control group. During the first peak of pandemic, the government collected personal information (e.g., credit card transaction, security camera footage, GPS data and other information) of confirmed cases,27 in order to find the epidemiological links of those who tested positive. These monitoring methods may have provided stress and affected the mental health of confirmed cases. However, majority of confirmed cases during this period were group infections which were comprised of long-term psychiatric inpatients19 and other confirmed cases were either hospitalized or admitted to a community treatment center depending on their symptom severity under the care of medical staffs.28 Moreover, the Korean government provided an active intervention and provided information regarding mental health services to confirmed cases.29 Therefore, they were under the care of the medical staffs from the hospital which may have alleviated suicidal behavior. Nevertheless, in order to investigate the direct effect of confirmed CODIV-19 on SIB, future studies need to include COVID-19 positive and negative samples outside of a controlled environment (e.g., hospital) where they are not being directly monitored by professionals. On the other side, those who tested negative were confronted with public stigma and discrimination but were provided with less external care or help from medical staff since they were on self-quarantine. The Korean government did provide mental health service to the whole population but only to those who seek help. Therefore, it could be implied that being tested for COVID-19 was a stressor for all individuals but confirmed cases were either under care of medical staff and got more active care compared to those who tested negative, which lead to decreased suicide attempt rate. However, due the relatively short follow-up period of our cohort data after the onset of the COVID-19 pandemic, mid-to-long-term effects of COVID-19 on suicide attempts were not derived from this study. According to previous research on the prevalence of suicidality (score ≥ 6 by the suicidality module of the Mini-International Neuropsychiatric Interview), 22.2% of the Middle East Respiratory Syndrome (MERS) survivors attempted suicide 12 months after the MERS outbreak in South Korea.30 In addition, since the proportion of confirmed cases among those tested was very small, it would be reasonable to interpret the COVID-19 test itself as a short-term risk factor for suicide attempts. Future studies are needed to examine the long-term effects of COVID-19 testing or infection on suicide.
Our results indicate among those who were tested for COVID-19, those with pre-existing mental disorders showed an increasing trend of SIB compared to those without pre-existing mental disorders, however statistically insignificant. This is contrary to the previous research which showed that people with pre-existing mental disorders have a higher risk of suicidal behavior than those without mental disorders during the COVID-19 pandemic.31 This could be due to the short observation period of this study or the limited number of pre-existing mental disorder patients included in the data. Future studies need to extend the observation period to find a clear relationship between pre-existing mental disorder and SIB.
The strength of this study is that it used nationwide population-based COVID-19 cohort data that contains all persons who were tested for COVID-19 between January 1 and May 31, 2020, which means that the results from this study are representative of confirmed or suspected COVID-19 cases in Korea within that period.
Despite the strengths, this study had limitations. First, since the control group in this study contained persons who were matched by the characteristics (sex, age, and regions) of the COVID-19 confirmed cases, the results in the control group cannot be generalized to the general population of Korea. In addition, these data had a relatively short study period after the onset of the COVID-19 pandemic. Therefore, future studies need to investigate the effect of COVID-19 on suicide related behaviors over a longer time. The second limitation is that the experience of quarantine was not included in the data that we have utilized. Therefore, we only imply the association between quarantine and suicide related behavior, but can’t conclude the direct effect of quarantine on suicide related behavior. Third, the majority of the confirmed cases during the study period were comprised of long-term psychiatric inpatients. Therefore, future studies need to include confirmed cases outside of a controlled environment to have a clearer view of the effect of confirmed COVID-19 on SIB. Lastly, due to the innate characteristic of the data, we used ICD-10 codes to classify suicide attempt and NSSI. Future study needs to add survey or interview data on patients when investigating suicide attempts and NSSI.
To the best of our knowledge, this is the first study to investigate the impact of the COVID-19 pandemic on SIB according to COVID-19 risk groups. Our results suggest that people who are tested for COVID-19 are at a high risk of suicide-related behavior (i.e., SIB) during the peak COVID-19 pandemic. Therefore, screening for suicide risk and psychological interventions is needed for these high-risk groups. Experts are stating that COVID-19 will not easily disappear32 and studies are constantly showing that the mental health of the population,33 health care workers34 and public workers35 in Korea is at stake. Therefore, continuous efforts of experts in the field to enhance the social support system and to alleviate stigma related to COVID-19 are needed.4
 XML Download
XML Download