

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cancer survival rate has increased sharply over the past two decades due to early diagnosis and improved treatment strategies. Cancer is more appropriately considered a chronic rather than a terminal illness.1 As the number of cancer survivors and their survival time increases, their quality of life (QoL) after cancer treatment has become a more important issue, as has the management and treatment of complications that have a significant effect on QoL.
Breast cancer is the most common cancer among women in the Republic of Korea, excluding thyroid cancer.2 According to the 2015 nationwide cancer statistics in Korea, breast cancer occurred at a relatively young age compared to other cancers, and the 5-year survival rate was 92%, an increase of 14% from 20 years ago.2 Thus, in breast cancer patients, complications induced by cancer treatments affect QoL over a long period of time.
Peripheral neuropathy is one of the most frequent adverse event induced by chemotherapy, especially taxnes.3 Peripheral neuropathy occurs in 11–64% of patients receiving chemotherapy, is usually chronic, and recovery from symptoms is often incomplete.45 Therefore, identification of risk factors, early detection, and treatment of chemotherapy-induced peripheral neuropathy (CIPN) is essential for long-term management of breast cancer patients.
Among the risk factors for CIPN, clinical factors including chemotherapeutic regimen, cumulative dose and pre-existing neuropathy are known, and demographic factors include age and obesity.6 However, the role of psychiatric factors associated with CIPN is unknown, except one report that suggested an association between anxiety and persistent CIPN.7 Psychiatric symptoms are known to affect not only QoL but are also related to developing treatment complications.8 Therefore, investigating the prognostic role of psychiatric symptoms is important to prevent complications and alleviate mental distress.
Circadian rhythm disruption is associated with complications of chemotherapy.789 Chronotype is a behavioral manifestation influenced by individual differences in the timing of the endogenous circadian system. It is divided into morning, intermediate, and evening types. The discrepancy between personal chronotype and the socially preferred one, which may disrupt the circadian rhythm inducing poor general health, is called social jetlag, and evening chronotypes are known to be vulnerable to it.10 In previous studies, we showed that such misalignment between preferred and actual sleep time was associated with shorter disease-free interval in breast cancer,11 and that late chronotypes were associated with greater likelihood of chemotherapy-induced nausea and vomiting in this population.9 However, to our knowledge, there has been no study investigating the relationship between chronotype and CIPN. Given these findings, we hypothesized that since chronotype and chemotherapy complications are related to each other, the incidence of CIPN may be higher in the evening chronotype than the other chronotypes due to the vulnerability to social jetlag, and the morning chronotype protects against CIPN.
Go to : 
METHODS
Study design
The present study was conducted as one component of a primary cohort study named “The effects of circadian genes on sleep and associated symptoms in breast cancer patients under chemotherapy,” which was designed to evaluate the effects of sleep-related factors and genes on complications of breast cancer chemotherapy. The participants of the primary study were recruited from Seoul National University Hospital, which is a tertiary general hospital in Seoul, Republic of Korea, and were consecutively enrolled between February 2012 and May 2014. Clinical staff approached potential participants diagnosed with breast cancer who visited an oncologist’s outpatient clinic for adjuvant chemotherapy and provided detailed information about the study.
The inclusion criteria of the primary study were women aged 18 to 70 years with early-stage breast cancer, while waiting for adjuvant chemotherapy after completion of surgery, medically stable, and without a history of another cancer or significant medical conditions that could affect mood and sleep. Individuals with a history of psychiatric treatment for more than 1 month were excluded due to the possible effects of psychiatric symptoms and psychotropic medications. Patients who had worked on shifts in the preceding 6 months were also ineligible, as shift work could disrupt the circadian rhythm.
The current study proposed to identify the effect of chronotype on CIPN in patients with breast cancer. To investigate peripheral neuropathy induced by chemotherapy, subjects with moderate or higher numbness/tingling symptoms at the baseline were excluded. CIPN was defined as peripheral neuropathy symptoms of more than moderate severity 4 weeks after completion of chemotherapy.
Participants
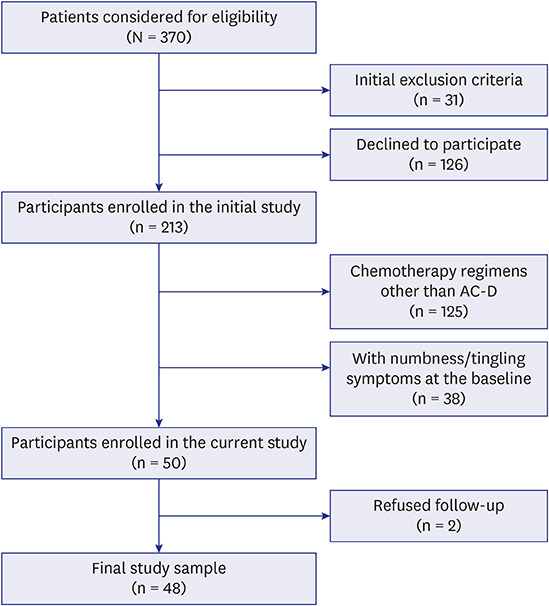
For the primary study, we approached 370 patients, of which 31 patients were ineligible. Among 339 eligible patients, 126 patients declined to participate. A total of 213 female patients from the oncology clinic were enrolled at baseline in the primary study (Fig. 1).
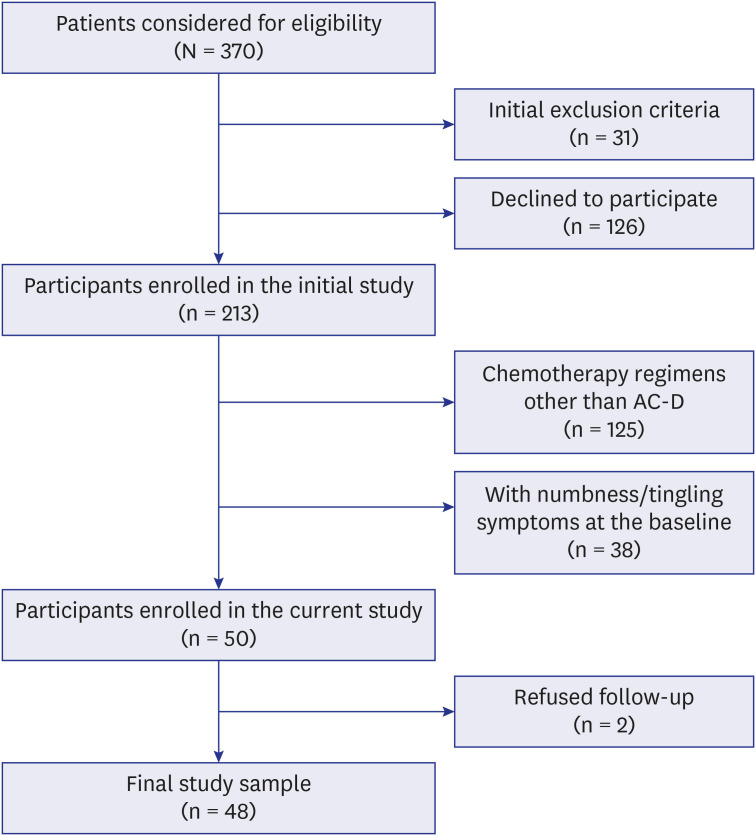
We included only one chemotherapy regimen including docetaxel in the current study to ensure homogeneity: AC-D (adriamycin and cyclophosphamide given once every two weeks for 4 cycles, followed by docetaxel administered once every two weeks for 4 cycles, n = 88). Of them, we selected 50 participants who were without moderate or higher numbness/tingling symptoms before adjuvant chemotherapy. Two of them refused follow-up. In total, 48 participants were included in the analyses (Fig. 1).
Measures
CIPN
Participants reported numbness and tingling on a numerical rating scale of 0–10 based on symptoms during the previous 24 hours. In previous studies using the same scale, it was reported that a grade of 3 or higher corresponded to moderate or severe peripheral neuropathy.12 In this study, the same criterion was used to define peripheral neuropathy.
Chronotype
The chronotype was assessed with the Composite Scale of Morningness (CSM).13 CSM is a 13-item scale, consisting of 9 items derived from Morningness-eveningness questionnaire (MEQ) and 4 items from the Diurnal Type Scale. Smith et al.13 reported that the CSM provided a better psychometric evaluation than MEQ. The total CSM score ranges from 13 to 55: the higher score represents the morning chronotype, and the lower score denotes the evening chronotype. Therefore, we categorized chronotypes into three groups: “morning chronotype,” “intermediate chronotype,” and “evening chronotype” based on the quartiles of CSM score, with the highest quartile representing the morning chronotype, the middle two quartiles the intermediate chronotype, and the lowest quartile the evening chronotype.1415
Sleep quality
Sleep quality and disturbance were assessed using the Pittsburgh Sleep Quality Index (PSQI).16 The PSQI scores range from 0 to 21. A higher score indicates poorer sleep quality, and a score higher than 8 was used to indicate poor sleepers in a previous validation study for the cancer patients.17 Therefore, a cutoff value of 8 was used to define significantly poor sleep quality in the current study.
Anxiety and depression
The Hospital Anxiety and Depression Scale (HADS) can be used to measure psychological adjustment.18 It comprises two sub-scales of anxiety and depression, consisting of seven questions each. We defined significant anxiety and depression as a score of 8 or higher on the respective subscales based on previous studies.19
Statistical analyses
Socio-demographic and clinical characteristics of participants with and without CIPN were compared using Student’s t-test, Wilcoxon rank-sum test, and χ2 test. Univariate logistic regression analyses were conducted to examine the variables associated with CIPN. A multivariate logistic regression model was built to identify the independent factors predicting CIPN. Variables that showed P < 0.1 in the univariate analyses were retained as covariates in the multivariate analysis, and we also included theoretical predictors as covariates. Statistical analyses were performed using R version 3.4.4 (https://www.r-project.org), and P values < 0.05 were considered statistically significant.
Ethics statement
The study was conducted in compliance with the ethical principles of the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board of Seoul National University Hospital (IRB No. H-1105-092-363), and the clinical trial registration number was NCT01887925 (www.ClinicalTrials.gov). Written informed consent was obtained from all participants.
Go to :
RESULTS
Demographic and clinical dharacteristics
The participants’ baseline demographic and clinical characteristics are shown in Table 1. In terms of the chronotype based on the quartiles of the CSM score, 21%, 54% and 25% of the subjects were classified as morning, intermediate, and evening chronotypes, respectively.

Table 1
Characteristics of participants according to CIPN
Values are presented as mean ± standard deviation or median [interquartile range] or number (%).
CIPN = chemotherapy-induced peripheral neuropathy, BMI = body mass index, BCS = breast-conserving surgery, TM = total mastectomy, PSQI = Pittsburgh Sleep Quality Index, HADS = Hospital Anxiety and Depression Scale (HADS-D and HADS-A: subscales for depression and anxiety, respectively).
![]()
The characteristics of the groups with and without CIPN are also presented in Table 1. There was a significant difference between the chronotypes of participants with and without CIPN, and the morning chronotype ratio was lower and the other chronotype ratios were higher in the group manifesting CIPN (P = 0.013). Sleep quality at the baseline was also poorer in participants with CIPN than in those without CIPN (P = 0.048).
Predictive factors for CIPN
Univariate analyses showed that CIPN was significantly less in the morning chronotype (odds ratio [OR], 0.08; confidence interval [CI], 0.01–0.63; P = 0.016) than in other chronotypes, and higher education (OR, 4.58; CI, 1.29–16.27; P = 0.019) was significantly associated with CIPN (Table 2).
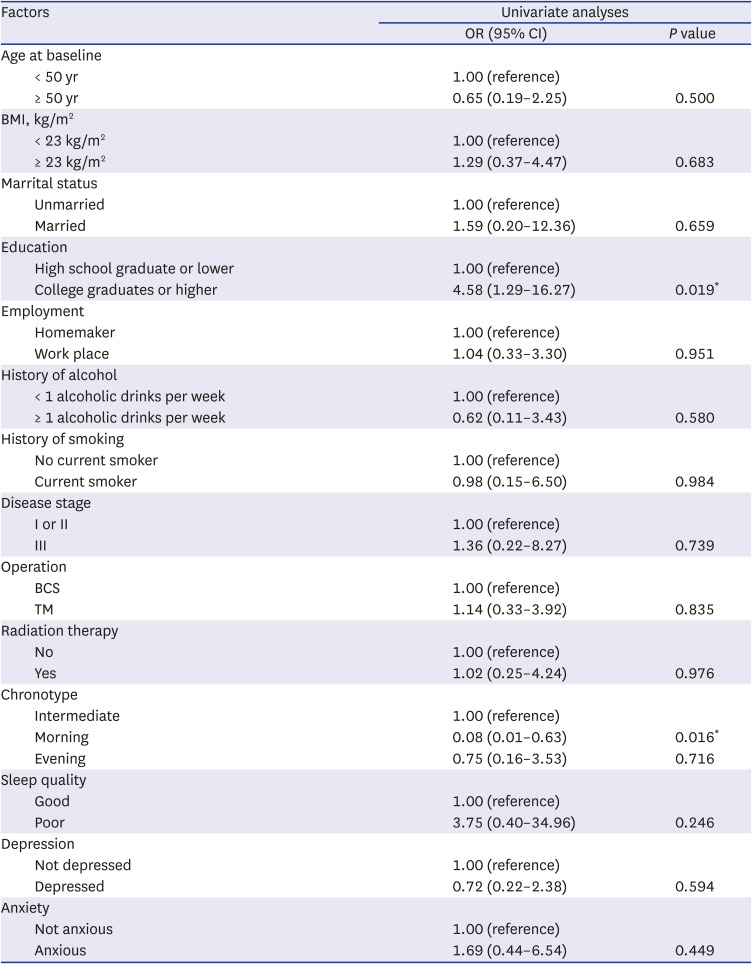
Table 2
Univariate analyses of predictors for CIPN
CIPN = chemotherapy-induced peripheral neuropathy, OR = odds ratio, CI = confidence interval, BMI = body mass index, BCS = breast-conserving surgery, TM = total mastectomy.
![]()
Three models were built for the multivariate logistic regression analyses. Model 1 included demographic factors (age, BMI, and education) as covariates of chronotype. Model 2 was analyzed with additional clinical variables (type of operation, alcohol use, and smoking) along with those analyzed in model 1. Model 3 included psychiatric variables (sleep quality, depression, and anxiety) in addition to those analyzed in model 2. In all the models chronotype was significantly correlated with CIPN occurrence, and morning chronotype was a significant protective factor against the development of CIPN (model 1: OR, 0.12; CI, 0.02–0.85; P = 0.034/model 2: OR, 0.09; CI, 0.01–0.74; P = 0.025/model 3: OR, 0.06; CI, 0.01–0.74; P = 0.028) (Table 3).
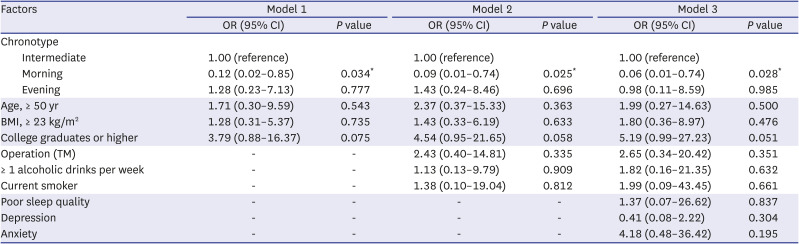
Table 3
Multivariate analyses of predictors for CIPN
CIPN = chemotherapy-induced peripheral neuropathy, OR = odds ratio, CI = confidence interval, BMI = body mass index, TM = total mastectomy.
![]()
Go to :
DISCUSSION
This study investigated the association between chronotype and occurrence of CIPN in breast cancer patients receiving adjuvant chemotherapy using docetaxel. Morning chronotype was a protective factor against CIPN. To our knowledge, this longitudinal observational study is the first to examine the association between chronotype and CIPN.
Docetaxel belongs to the taxane family of drugs and is known as a potent inducer of CIPN.20 Taxane-induced peripheral neuropathy (TIPN) is known to be associated with increased risk of falls and sleep disorders as well as decreased subjective QoL.21 Several studies identified predictive factors for TIPN. Obesity and age have been suggested as risk factors; however, it is difficult to predict patients who develop TIPN. This study has implications for identifying the morning chronotype as a protective factor for TIPN.
The study findings are based on the relationship between pharmacology of docetaxel and chronobiology. Docetaxel inhibits the division of rapidly growing cells via microtubule stabilization. Cell cycle and circadian rhythm are linked.22 From an evolutionary point of view, DNA replication occurs at night, to avoid DNA damage by sunlight, and mitosis occurs throughout the day.23 We have described the individual differences in endogenous circadian rhythm as a chronotype. Thus, we can infer that the occurrence of TIPN is associated with chronotype. Norma et al.24 analyzed the degree of apoptosis in duodenal cells after administering colchicine, a microtubule stabilizing agent, to several groups of mice at different times. They reported a nearly two-fold higher degree of apoptosis in the group that received colchicine at 8AM compared with the other groups. The occurrence of CIPN also could depend on the administration time and chronotype, due to the similar mechanism with colchicine.
Another mechanism of TIPN involves increased neuroinflammation in the spinal cord and dorsal root ganglia.20 Several studies show that the immune system is regulated by circadian rhythm, disruption of which induces inflammation. Adams et al.25 reported that circadian rhythm disruption increases the secretion of IL-6, a proinflammatory cytokine, and activates inflammation. The secretion of IL-6 has been reported to exhibit circadian rhythm in patients with rheumatoid arthritis, with elevated levels in the morning.26 Adams et al.25 suggested that circadian rhythm disruption interferes with rhythmicity of IL-6 secretion, which elevates IL-6 level and exacerbates inflammation. As the evening and intermediate chronotypes are vulnerable to circadian rhythm disruption compared to the morning chronotype, we can appreciate this study showing that morning chronotype is protective against CIPN.
This study has several strengths. First, this study was the first to investigate the association between psychiatric factors and the occurrence of CIPN. Lee et al.7 reported that pretreatment anxiety was associated with persistence of CIPN, but did not reveal the relationship between anxiety and incidence of CIPN. Second, we designed the present study as a prospective longitudinal study, to avoid recall bias, which generally occurs when analyzing psychiatric factors.
This study has several limitations. First, we did not use a physiological tool to measure peripheral neuropathy, which is the main outcome of the current study, and based on a self-reported scale. Second, the follow-up period was 4 weeks after the completion of chemotherapy, which is relatively short. CIPN is a clinically significant issue because it often does not improve and becomes chronic even after many years. Follow-up data for several years after completion of chemotherapy can be used to analyze the factors associated with chronic CIPN. Third, several previous studies have reported circadian rhythmicity in the symptoms of peripheral neuropathy,2728 which may have contributed to the association of chronotype with CIPN. In our study, the analysis related above could not be performed because the information on severity of CIPN by time of day was not collected. Fourth, it is possible that chemotherapy, including docetaxel, changed the participants’ chronotype by inducing sleep phase advance or delay. In this study, the chronotype was measured only before chemotherapy, so we could not determine the change in chronotype. Fifth, this study analyzed the relationship between docetaxel-induced peripheral neuropathy and chronotype. However, chemotherapeutic agents that can induce CIPN primarily include platinum-based drugs, taxanes, ixabepilone and thalidomide.29 Therefore, the generalizability of our findings may be limited.
CIPN is a major complication that chronically reduces QoL after chemotherapy in breast cancer patients. We recommend a further long-term follow-up study to investigate the predictive factors for chronic CIPN. We also suggest measurement of biomarkers, such as cytokines, in addition to self-reported scales, to identify the mechanisms of the risk factors associated with CIPN. Further studies are needed to corroborate these findings to enhance the possibility of personalized medicine using chemotherapy based on chronotype to improve the risk/benefit ratio of treatment.
Go to :
 XML Download
XML Download