

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Human immunodeficiency virus (HIV)-associated facial lipoatrophy (FLA) is a common skin disease in patients with HIV that is related to the use of highly active antiretroviral therapy (HAART).1 It is characterized by volume loss of the face that primarily affects the contours of the cheeks, orbits, and temples. HIV-associated FLA can be a social stigma, and it negatively affects patients’ mental health, quality of life, social function, and compliance with HAART.23
The extended life expectancy of patients with HIV has increased the demand for cosmetic correction of HIV-associated FLA, and filler injections are frequently used for treatment as they improve facial volume. Biodegradable fillers including poly-L-lactic acid (PLLA) and calcium hydroxyapatite (CaHA) are Food and Drug Administration (FDA)-approved for the treatment of HIV-associated FLA, and several studies have been performed to elucidate the effect of other biodegradable and permanent soft tissue fillers.45 Since existing fillers show various degrees of therapeutic effects and maintenance without standardized guidance, it is necessary to develop a biocompatible, biodegradable filler that is safe and has a long-term volumizing effect. Therefore, the purpose of the present study was to investigate the efficacy and safety of hyaluronic acid filler mixed with micronized cross-linked acellular dermal matrix (HA/MADM) in treating HIV-associated FLA.
METHODS
Study design and population
We conducted a prospective, open-label pilot trial that evaluated the efficacy and safety of HA/MADM filler to treat HIV-associated FLA in 14 patients at Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. The study product (MegaNuovo®, L&C Bio, Inc., Seongnam, Korea) comprises micronized cross-linked acellular dermal matrix and hyaluronic acid (HA) mixed in a weight/volume ratio of 17:1. We included patients with HIV-associated FLA who had a Carruthers Lipoatrophy Severity Scale (CLSS) grade46 2 or greater for at least one side of the lesion and had not received facial augmentation, lifting, or other treatment of HIV-associated FLA within 2 years.
Treatment and follow-up
All patients were treated with HA/MADM filler and followed up from March 2020 to February 2021. Patients received injections by using the “smile-and-fill” and depot technique to reach the deep subcutaneous level.6 All injections were performed by the same plastic surgeon (S.Y.S) in an outpatient setting with an optional touch-up at the 4-week follow-up. In the case of bilateral asymmetry, different amounts of filler material were injected for symmetrical correction.
The study duration was 6 months and included five assessment visits: an initial visit at week 0 (baseline) and four follow-up visits at 1, 4, 12, and 24 weeks. A blinded board-certified dermatologist independently evaluated the CLSS grade by comparing digital photographs in a non-chronological order. A three-dimensional skin analysis camera system (Antera 3D®, Miravex, Dublin, Ireland) was used to perform a quantitative assessment of the depressed volume of lipoatrophy. Additionally, skin elasticity was measured using the Cutometer® Dual MPA580 (Courage+Khazaka electronic GmbH, Köln, Germany). We assessed the patient and physician satisfaction with treatment outcome using the Global Aesthetic Improvement Scale (GAIS)7 with five-point scores (1: worse, 2: no change, 3: improved, 4: much improved, and 5: very much improved). Safety assessments included complications assessed through physical examination and self-reporting of related adverse events.
Statistical analysis
Data are presented as numbers (percentages) or means ± SDs. Repeated measures analysis of variance (RM-ANOVA) and subsequent post-hoc analysis with the Wilcoxon signed rank test with the Bonferroni correction was performed to compare and incorporate parameters at each time point. All statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA).
RESULTS
In this prospective pilot study, 14 Korean patients with HIV-associated FLA were enrolled, and 13 completed the 6-month follow-up (one patient was lost to follow-up and retracted his consent). All patients were men, and the mean age at diagnosis was 51.5 ± 12.5 years. The mean duration on HAART was 155.5 ± 46.6 months, the mean CD4 cell count was 577.0 ± 340.4 cells/μL, and 12 (92.3%) patients had < 20 HIV RNA copies/mL. Baseline CLSS grades were evaluated by an independent assessor and were as follows: grade 1, three lesions (12%); grade 2, 14 lesions (56%); grade 3, seven lesions (28%); and grade 4, one lesion (4%). Twelve patients were injected with HA/MADM filler in both cheeks or infraorbital areas, and one patient received an injection in the forehead; thus, 25 sites of injection were noted for further analysis. The mean total volume of HA/MADM used was 1.20 ± 0.99 mL per lesion. Most patients were treated with a single injection of HA/MADM at the initial visit; only one patient received an additional touch-up injection at the 4-week follow up. Table 1 summarizes the patient characteristics and treatment details.
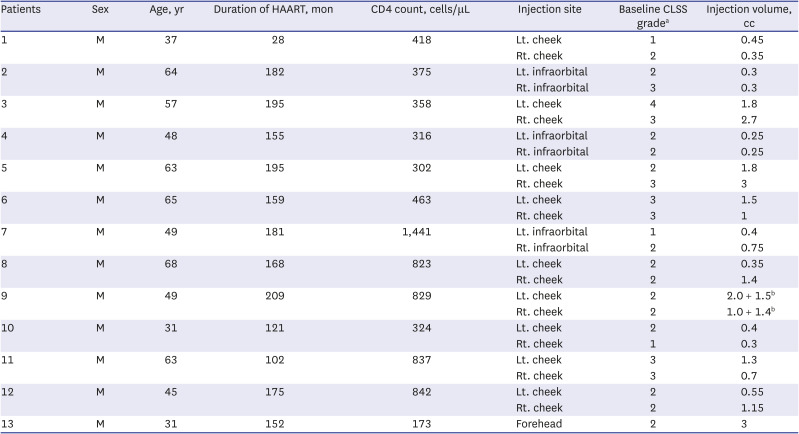
Table 1
Summary of patient characteristics and treatment details
HAART = highly active antiretroviral therapy, CLSS = Carruthers Lipoatrophy Severity Scale, M = male, F = female, Rt. = right, Lt. = left.
aScore ranged from 1 to 4, with higher scores indicating greater severity; bAn additional touch-up injection was performed after the 4-week follow up visit.
![]()
We evaluated the CLSS grade, depressed volume due to lipoatrophy, and skin elasticity of each lipoatrophy lesion from baseline to all time points of follow-up; the findings are summarized in Table 2. Compared to baseline, the average decreases of the CLSS grade were 1.12 points (50% improvement) after a 1-week follow-up visit and 0.96 points (42.9% improvement) after the 24-week visit. RM-ANOVA and subsequent post-hoc analysis revealed an overall significant improvement of the CLSS grade during the study period along with significant differences in the CLSS grade at all follow-up time points compared with pre-treatment (Fig. 1A).
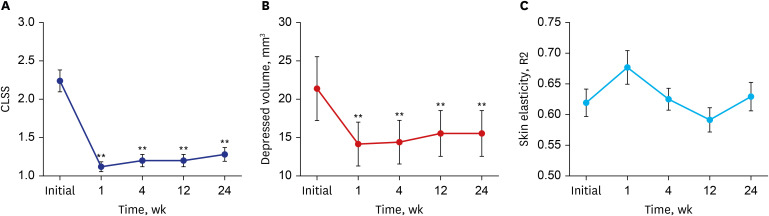
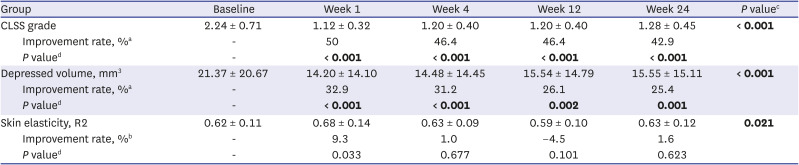
Fig. 1
Average (A) CLSS grade, (B) depressed volume measured using the Antera 3D® camera system, and (C) skin elasticity measured using the Cutometer® over the study period. Error bars depict the standard error of the mean.
CLSS = Carruthers Lipoatrophy Severity Scale, R2 = percentage of viscoelasticity.
**P < 0.01 in post-hoc analysis at each time point.
![]()
Table 2
Baseline and post-treatment CLSS grade, depressed volume due to lipoatrophy, and skin elasticity
Data are shown as mean ± SD. Statistically significant P values are in bold.
CLSS = Carruthers Lipoatrophy Severity Scale, R2 = percentage of viscoelasticity.
aDefined as (baseline measurement − follow-up measurement)/baseline measurement × 100%; bDefined as (follow-up measurement − baseline measurement)/baseline measurement × 100%; cRepeated measures analysis of variance, with the Greenhouse-Geisser correction. P < 0.05 was considered significant; dPost-hoc analysis of each time point with the Wilcoxon signed rank test with the Bonferroni correction, where P < 0.010 was considered significant.
![]()
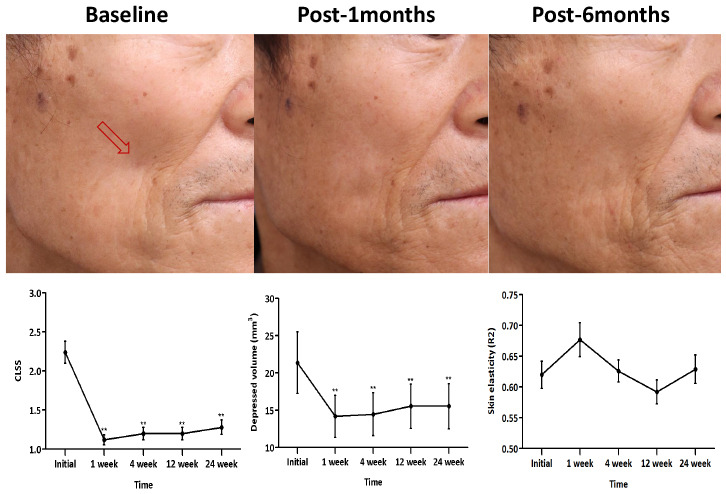
Quantitative skin analysis was performed by measuring the volume of depression and skin elasticity. Using the depression mode of Antera 3D®, we measured and visualized the depressed volume due to lipoatrophy, which was well correlated with that shown in the clinical photograph (Figs. 2 and 3). The average depressed volume was 21.37 ± 20.67 mm3 at the initial visit, and it decreased to 14.20 ± 14.10 mm3 after the 1-week follow-up visit (32.9% improvement). Similar to the CLSS grade, RM-ANOVA and subsequent post-hoc analysis of the depressed volume showed significant improvement during the overall study period (Fig. 1B). However, skin elasticity measured with the Cutometer® showed 9.3% improvement after the 1-week follow-up visit and 1.6% improvement after the 24-week visit. The analysis failed to show statistical significance at all follow-up time points compared with pre-treatment (Fig. 1C).
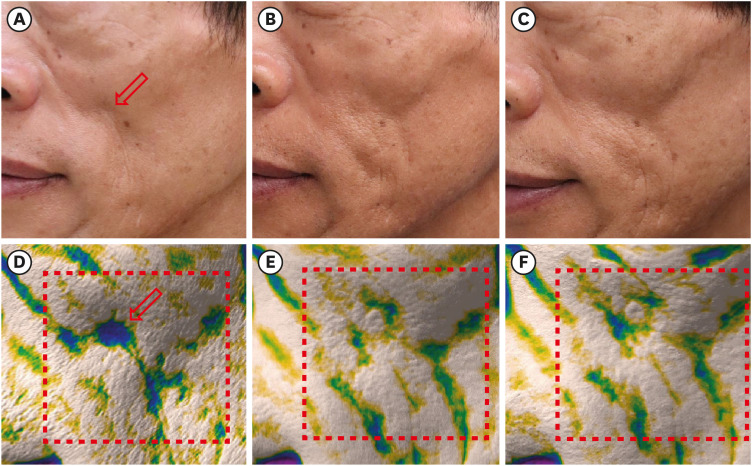
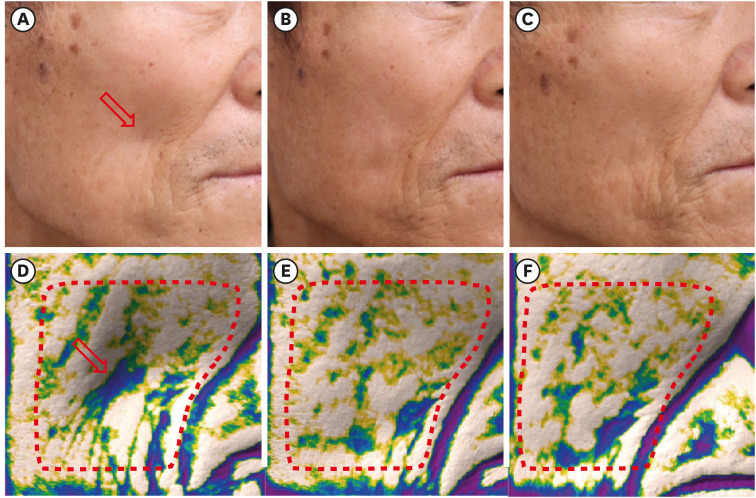
Fig. 2
Clinical photographs of patient number 3 (A) before the injection (baseline), (B) 1 month after the injection, and (C) at the 6-month follow-up visit. Images of the depression mode of the Antera 3D® camera system correspond well with the clinical photographs; (D) before the injection (baseline), (E) 1 month after the injection, and (F) at the 6-month follow-up visit. The depressed volume within the area surrounded by the red dotted line is quantitatively measured. The red arrow indicates the site of filler injection. The figures are published under agreement of the patient.
![]()
Fig. 3
Clinical photographs of patient number 5 (A) before the injection (baseline), (B) 1 month after the injection, and (C) at the 6-month follow-up visit. Images of the depression mode of the Antera 3D® camera system corresponds well with the clinical photographs; (D) before injection (baseline), (E) after 1-month, and (F) 6-month follow-up visit. The depressed volume within the area surrounded by the red dotted line is quantitatively measured. The red arrow indicates the site of filler injection. The figures are published under agreement of the patient.
![]()
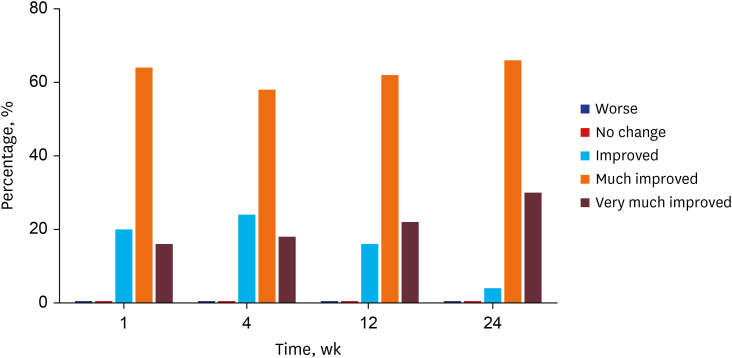
One week after the injection, 80% of patients and physicians rated the treatment outcome as much improved or very much improved based on the GAIS. The degree of satisfaction was gradually increased; almost all (96%) patients and physicians rated the treatment outcome as much improved or very much improved at the 24-week follow-up visit (Fig. 4). No patients or physicians rated the treatment outcome as no change or worse than before. No permanent or serious treatment-related adverse events were reported during the study period. Only one patient reported a subcutaneous nodule after the 1-week follow-up visit, but it spontaneously resolved by the next visit. None of the patients found exacerbations of HIV-related comorbidities throughout the study period. The mean CD4 cell count measured after the 24-week follow-up visit was unchanged compared to that of the initial visit (542.8 ± 217.4 cells/μL, P = 0.750).
DISCUSSION
In this prospective, open-label pilot study, significant decreases in the CLSS grade and volume of depression were noted with HA/MADM filler in patients with HIV-associated FLA. A single injection of HA/MADM was sufficient to maintain the volumizing effect throughout the study period. Compared to 1 week after the injection, improvement rates of the CLSS grade and depressed volume decreased by only 7.1% and 7.5% at the 24-week follow-up visit, respectively. In addition, the subjective satisfaction of patients and physicians remained high throughout the study period. However, the improvement effect of HA/MADM on skin elasticity was modest (less than 10%) and failed to demonstrate statistical significance. The filler material in the present study was safe; no subject reported any adverse events, except transient subcutaneous nodule formation in one patient.
Patients with HIV who develop persistent lipoatrophy may benefit from plastic surgery, autologous fat transfers, and dermal fillers including PLLA, CaHA, or HA.48 Among these options, the PLLA filler injection is considered to have the highest efficacy and is relatively safe.5 However, PLLA requires reconstitution before injection, multiple treatment sessions, and a vigorous manual massage after injection to avoid nodule formation.49 CaHA was the second FDA-approved filler agent for treating HIV-associated FLA, which may be ideally used deeply over bone for focal enhancement but may not be suitable for correcting volume loss of the midface.410 HA filler is considered another safe and effective treatment option because of the stability of HA material in vivo and theoretical reversibility with hyaluronidase.6711 However, HA could result in delayed onset nodules, foreign body granuloma, tissue necrosis due to vessel compression, and allergic reaction.612
HA/MADM was developed to complement HA filler, which is naturally not replaced by autologous tissue. The manufacturing process of HA/MADM involves cross-linking of the collagen matrix at the level of the peptides and collagen fibers by using electron beams, which gives the filler material augmented tensile strength and a stratified appearance with structural integrity.131415 HA/MADM contains the extracellular components necessary for cell integration and promotes long-term extracellular matrix remodelling through increased expressions of type I collagen, matrix metalloproteinases-1 (MMP-1), MMP-2, and transforming growth factor-ß for up to 6 months.13 HA/MADM can also promote adipocyte survival via increased vascular endothelial growth factor expression14 and showed higher volume retention than the fat graft in a mouse model.16 Considering the pathogenesis of HIV-associated FLA, including reduced adipogenesis and increased adipocyte apoptosis,5 HA/MADM may have an advantage over other filler materials by recovering the patient’s own adipose tissue. Limitations of our study include the relatively small sample size, absence of a control group, and lack of female patients. Moreover, this study's relatively short follow-up period limited the assessment of the long-term safety and efficacy of the HA/MADM filler. However, this study used a three-dimensional imaging device to measure volumetric changes and HA/MADM filler retention at each lesion and all time points. This may complement the efficacy evaluation and help assess the durability of this HA/MADM filler.
This study shows that the HA/MADM filler is a safe and effective treatment modality to correct HIV-associated FLA. A single injection of HA/MADM was sufficient to maintain correction for up to 6 months. Future randomized clinical trials with a large sample size and longer study period may confirm its long-term efficacy, durability, and safety. Furthermore, the authors expect that filler material composed of extracellular matrix components of human adipose tissue may exert a more long-term volumizing effect.
 XML Download
XML Download