

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
There is general agreement in the literature that some of the voice characteristics of deaf people differ considerably from those of speakers with normal hearing. Congenitally deaf speakers tend to have a higher fundamental frequency (F0) than speakers with normal hearing (1, 2). On the other hand, some investigators did not find a higher F0 in young hearing impaired children than they found in the controls (3).
Lack of auditory control also affects the control of voice intensity. Leder et al. (4) suggested that adventitious profound deafness was associated with a significantly increased voice-intensity level and greater fluctuations in intensity production.
Severe and profound hearing loss in young children results in poor speech perception and production skills. Multichannel cochlear implantation (CI) in these children permits significant improvement in both speech perception and production following implantation (5-8). The speech perceptual abilities and the speech intelligibility could be considered the most important primary outcome measures of CI. In particular, the speech intelligibility rating (SIR) was designed as a time-effective global outcome measure of speech production in real-life situations.
The aim of our study was to investigate the relationship between the acoustic analysis before CI and the speech intelligibility before and after CI.
MATERIALS AND METHODS
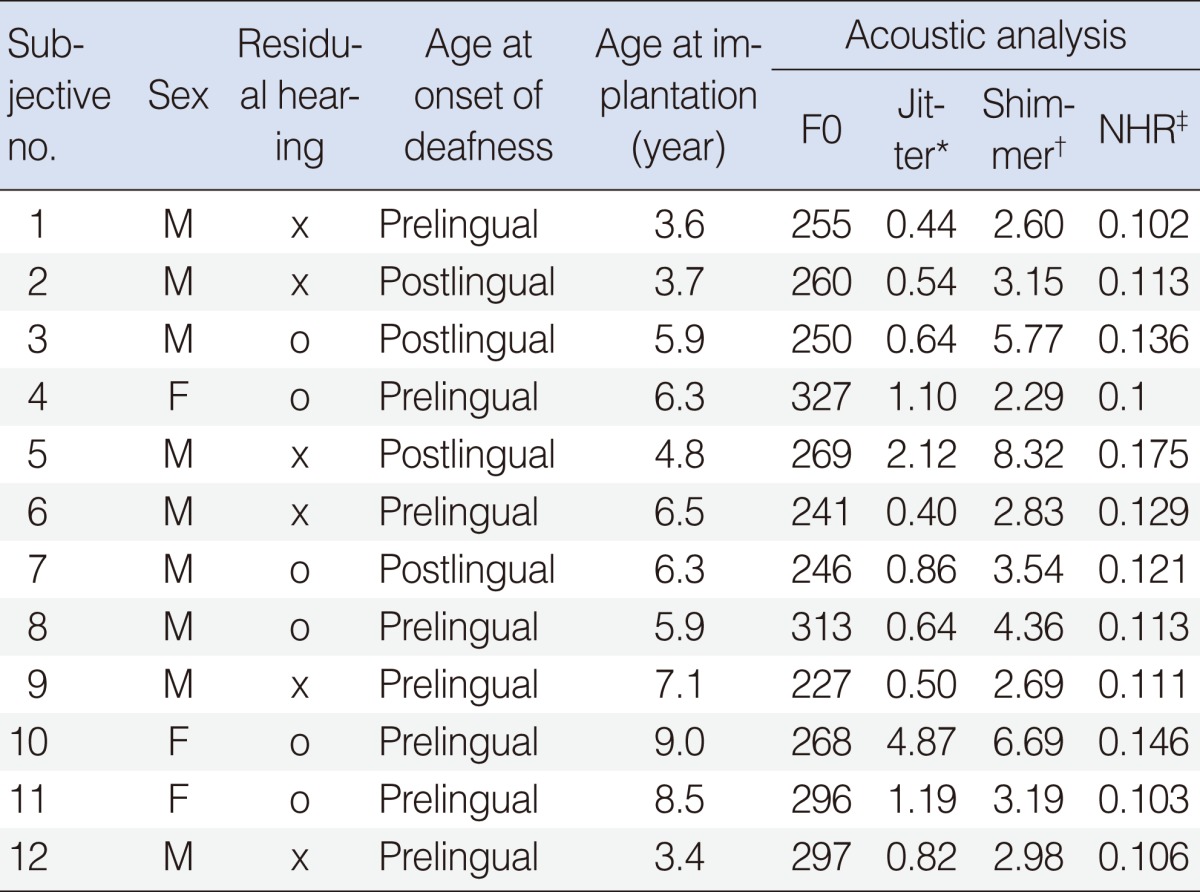
Twelve deafened children (9 boys, 3 girls) who were recipients of cochlear implants and subsequently followed up at Asan Medical Center, University of Ulsan College of Medicine (Seoul, Korea) were included in the study. The children who underwent CI were between the ages of 3.4-9.0 years (mean, 5.92 years; standard deviation, 1.81 years). Six children had residual hearing, but the remaining six children had no residual hearing. They were all implanted with a multi-channel CI. For all of the patients, an acoustic analysis of the sustained vowel 'a' was performed before CI. The F0, jitter, shimmer and noise-to-harmonic ratio (NHR) were obtained before implantation. SIR was performed for all patients prior to and 12 months after CI.
The voice samples of a sustained vowel 'a' at a habitual pitch and loudness, for a duration of 3s, were analysed with a Multi-Dimensional Voice Program (Kay Pentax, Lincoln Park, NJ, USA). The vowel 'a' was chosen because it can be produced even by young children and is mainly dependent on acoustic rather than orosensitive control. The average F0, jitter, shimmer, and NHR were determined for every voice sample. Jitter provides an evaluation of the very short-term variability of the pitch period. Shimmer provides an evaluation of the very short-term variability of the peak-to-peak amplitude (loudness) within the analyzed voice sample. NHR is an average ratio of the energy of the inharmonic components in the range 1,500 to 4,500 Hz to the harmonic components' energy in the range 70 to 4,500 Hz, and represents a general evaluation of noise presence in the analyzed signal. According to the recommendation of the European Laryngological Society, jitter and shimmer are used to estimate phonation quality.
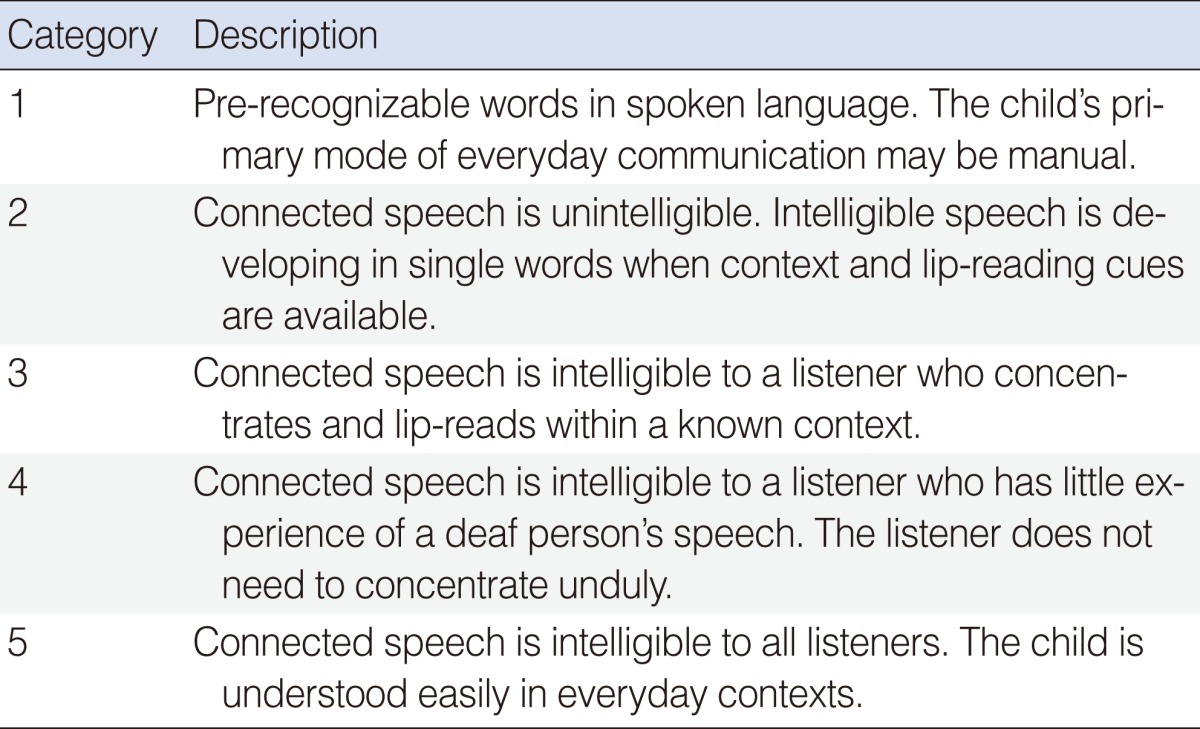
We analyzed the speech perception and speech intelligibility of implanted children. These children were followed up with regular 6 months intervals. In each visit, we performed a battery of speech perception and speech intelligibility to evaluate patient progress with the implant. Evaluation was conducted in a quiet room using live voice presented at about 60 dB sound pressure level (SPL). Speech perception was measured using the Categories of Auditory Performance (CAP) and monosyllabic word tests, where the latter included 2 lists of 25 monosyllabic words that can be scored as both words and phonemes percent correct. Speech intelligibility was measured using SIR, designed to evaluate the intelligibility of children with a cochlear implant. An experienced speech language pathologist classified global speech production according to one of five hierarchical categories for which the criteria are described in Table 1.
SIR was evaluated with the spontaneous speech prior to implantation and at 12 months after CI. Subjects were assessed in a quite room and the evaluations were performed by the same speech language pathologist at each assessment.
The results of the acoustic analyses and speech intelligibility before and after CI were compared for preoperative hearing. The results of the speech intelligibility were compared for the age of operation and preoperative acoustic analysis (F0, jitter, shimmer, NHR).
RESULTS
The absolute values of the fundamental frequency of the investigated children ranged between 241 and 327 Hz. The mean F0 for subjects was 270.8±30.9, while for boys the mean was 262±27.4 and for girls was 297±29.5 (Table 1).
In all patients, jitter score was 1.18±1.26 and shimmer value was 4.03±1.90. Both jitter and shimmer scores were elevated as compared to the normal range (1.1 and 3.8, respectively). All patients were found to have normal range NHR (normal range<0.2) (Table 2).
Six patients among the total 12 had residual hearing. But preoperative residual hearing had no influence on preoperative voice parameters. There were no significant differences observed in terms of fundamental frequency, jitter, shimmer, NHR among patients with residual hearing and without residual hearing on analysis using Mann-Whitney test (P=0.168, P=0.078, P=0.262, P=0.837).
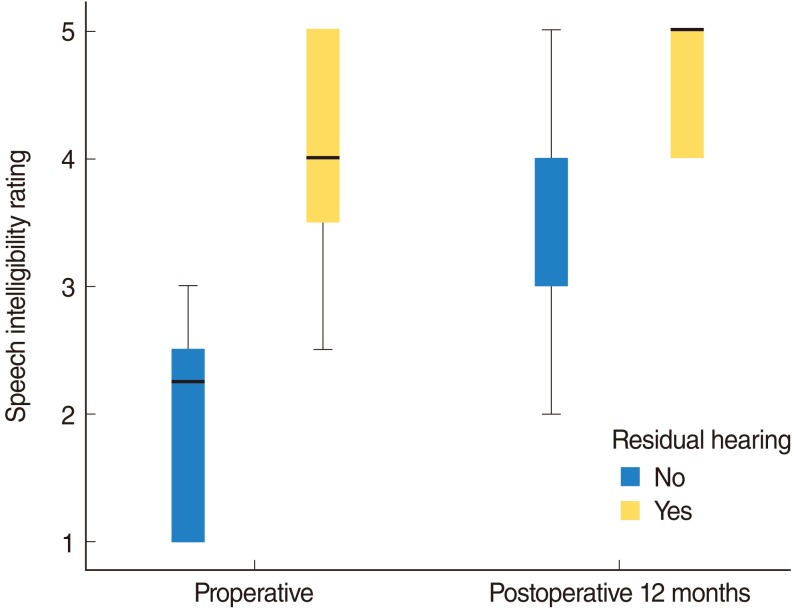
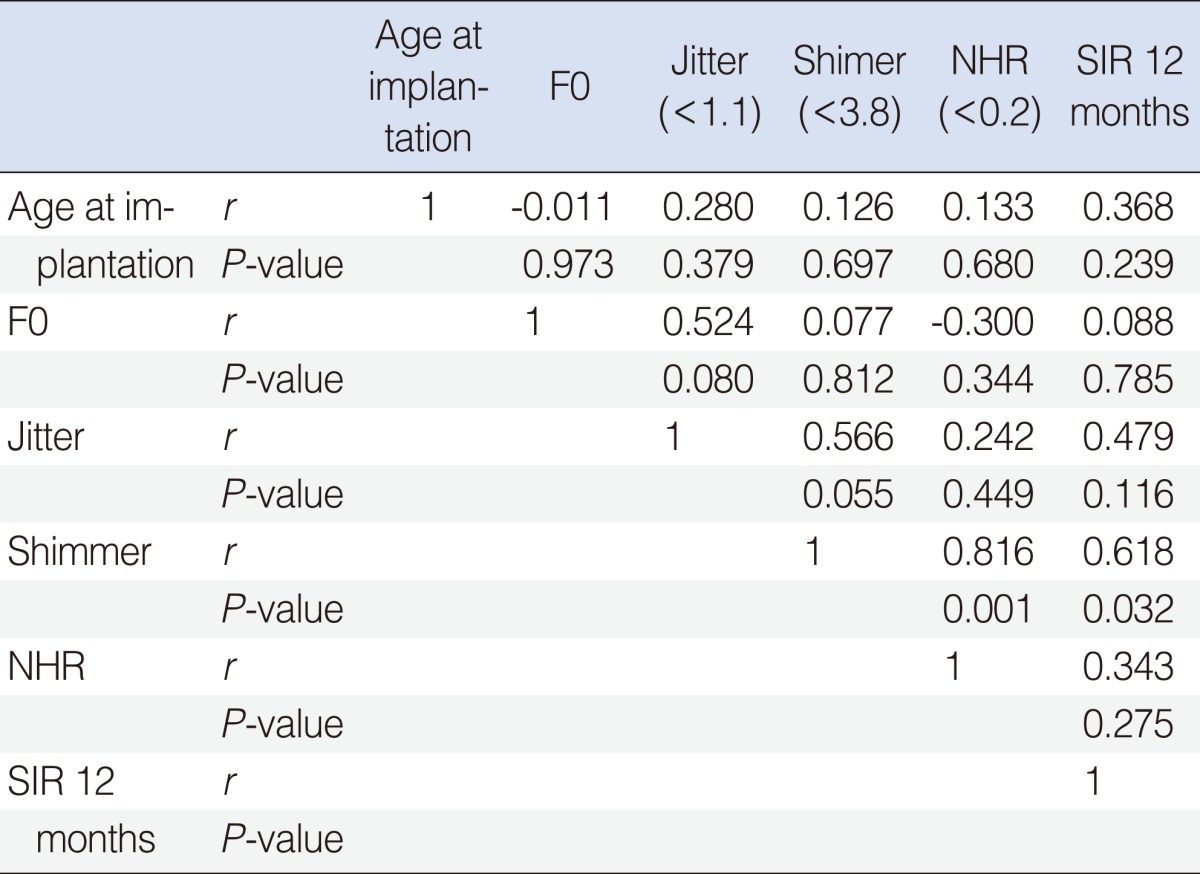
The children with residual hearing had a high grade of speech intelligibility before and after CI (Fig. 1). The mean preoperative SIR was measured to be 4 in children with residual hearing and significantly higher (P=0.004) than in children without residual hearing (SIR=2.25). The mean SIR 12 months after implantation was 5 in children with residual hearing and also significantly higher (P=0.028) in children without residual hearing (SIR=3). Among the preoperative voice parameters, shimmer had a positive correlation with speech intelligibility 12 months after surgery (r=0.618, P=0.032) (Table 3).
DISCUSSION
Our study is focuses on the relationship between acoustic analysis before CI and the speech intelligibility rating before and after CI. In previous studies, it has been demonstrated that changes in hearing may interfere with adequate use of the structures involved in speech and voice production due to lack of auditory feedback. The influence of CI on voice parameters has been studied and the performance of speech perception, speech intelligibility, and language development after CI was studied (9-12). However the relationship between voice analysis and speech performance in deaf patients has not been fully studied yet.
Previous studies proved that lack of auditory control affects the control of voice intensity. Profound hearing loss was associated with a significantly increased voice intensity level and greater fluctuations in intensity production. After implantation, however, the auditory control of voice and speech were possible resulting in voice and speech improvement (4). Other studies have shown that pitch and amplitude variability decrease after implantation by regaining hearing control over phonation. Jitter, which represents pitch control, decreased significantly, and shimmer, which represents intensity control, also decreased but not to significant level (13).
In this study, children with residual hearing had better speech intelligibility than children without residual hearing. The presence of pre-implantation oral language skills may be important for post-implantation success with prelingual deaf adults and children implanted beyond the sensitive period for language development (14-18). In particular, it has been observed that groups of patients whose pre-implantation speech was judged to be intelligible seemed to achieve greater post-implantation benefit than groups of patients with less intelligible speech. In prelingual deaf patients, the presence of intelligible speech may be a necessary condition for success with a CI.
Our study had several limitations. We did not include infant and young children because the examination for voice parameters was not possible in these ages. Another limitation of this study is that postoperative voice parameters were not examined. Despite these limitations, this study was useful in demonstrating that preoperative voice intensity and quality are predictors of speech intelligibility as cochlear implant outcome.
In conclusion, the children with residual hearing had high grade of speech intelligibility before and after CI. Shimmer on preoperative voice analyses had influence on speech intelligibility after CI. The preoperative voice intensity and quality can be a predictor of speech intelligibility as cochlear implant outcome.
 XML Download
XML Download