

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
A number of cochlear implantation (CI) candidates have ear malformations, in particular an abnormal course of the facial nerve (FN). The course of the FN is very important for CI surgery; the more abnormal the course of the FN, the more difficult it is to perform CI surgery. However, it is extremely difficult for surgeons to understand the three-dimensional (3D) course of the FN prior to surgery through the use of two-dimensional (2D) computed tomography (CT) images.
In this study, we attempted to reconstruct a 3D image of temporal bone structures using CT imaging for a plan of CI surgery in a malformed ear and show the 3D images of the two cases.
Go to : 
MATERIALS AND METHODS
From 2010 to 2011, we prepared 3D images for 6 separate CI cases prior to surgery. These cases consisted of 5 patients (3 boys, 2 girls, ages 1-7 years), including one bilateral case. All of the patients had congenital malformations in the temporal bone structures, such as in the FN, cochlea, semicircular canal (SC), or stapes. We created 3D images using a method we developed that utilized a public personal computer.
First, we manually colored preoperative CT images, which were axial sections of the temporal bone scanned by a normal CT scanner (SOMATOM Definition; Siemens Medical, München, Germany) at a slice thickness of 0.5 mm using Photoshop CS extended. The extended version can import and edit DICOM files directly. The inner ear labyrinth, auditory ossicles, and FN were shaded in blue, red, and yellow, respectively, maintaining the shape of these structures. We had to paint every axial section of temporal bone CT images; there were about 30-40 slices. It took about two hours to accomplish the coloring process.
We then converted the colored 2D-CT images to 3D images using Delta Viewer (DV), a freeware for Macintosh available on the Internet (http://delta.math.sci.osaka-u.ac.jp/DeltaViewer/index.html). This 3D reconstruction can be done from CT images of any condition, such as the thickness of the slice of images, but the thinner the CT slices are, the more detailed and smoother the 3D images will be. This DV-3D rendering process was completed automatically within a few minutes. In this paper, we refer to the 3D images created using DV as DV-3D images.
Fig. 1 is a DV-3D image of the normal temporal bone structures. We can rotate DV-3D images freely using the DV application.
 | Fig. 1Example of Delta Viewer 3 dimensional image of normal temporal bone structures of left ear based on computed tomography image. Image (A) is antero-lateral inferior view, and image (B) is superior view. The bony labyrinth was shaded in blue and includes the cochlea (Co), vestibule (V), anterior semicircular canal (ASC), lateral semicircular canal (LSC), posterior semicircular canal (PSC), and round window (RW). The internal auditory canal (IAC) and facial nerve (FN) are shaded in yellow. The ossicles are shaded in red and include the malleus (M), incus (I), and stapes (S). The annulus tympanicus (AT) and vestibular aqueduct (VA) are shaded in green and purple, respectively.
|
Before each CI procedure, we discussed any problems anticipated based on the DV-3D images and planned the surgery with those who would be performing the procedure. We also brought either the printed images or the notebook PC to the operating room and compared the images with the surgical findings during the CI procedure (Fig. 2).
Go to :
RESULTS
Case 1. Left ear of a three-year-old boy
The patient presented with bilaterally malformed ossicles, SC hypoplasia, internal auditory canal stenosis, and an abnormal course of the FN. We had already performed CI surgery on the patient's right ear one year before. The outcome of his speech was not as good as that of a patient with a non-malformed ear. We then planned a second CI procedure on the patient's left ear. We expected that it was going to be difficult to perform cochlear fenestration because of the facial nerve abnormality, so we prepared DV-3D images of this case before the CI surgery.
The DV-3D images (Fig. 3) indicate that the cochlear turn is intact, the lateral SC is hypoplastic, the long crus of the incus and stapes is absent, the labyrinthine segment of the FN is more posteriorly placed, and the tympanic and mastoid segments are antero-inferiorly displaced and running more vertically than normal. Fig. 4 shows the structures pictured in the same position as we found them during surgery. These images show that the stapes are absent and that the FN runs antero-inferiorly onto the oval window.
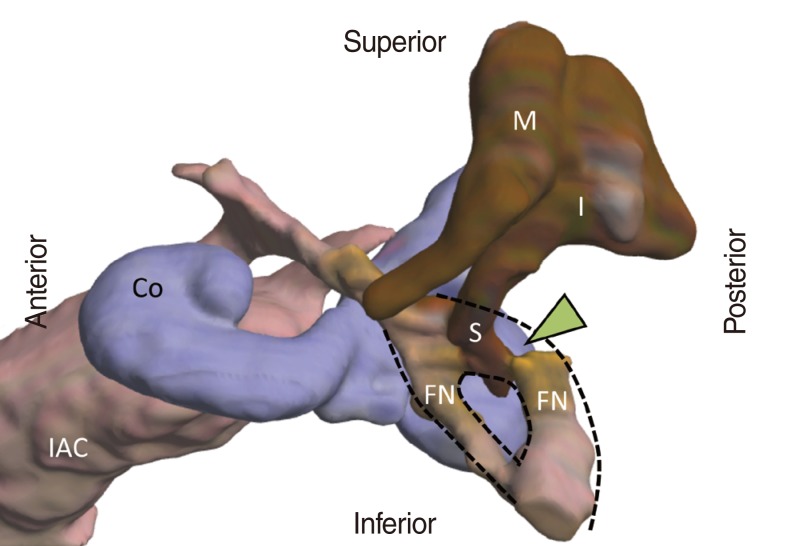
 | Fig. 3(A) Lateral view of the temporal bone structures of case 1. The lateral semicircular canal (LSC) is hypoplastic, and the crus of the incus (I) and stapes (S) are absent. The labyrinthine segment of the facial nerve (FN) and the geniculate ganglion are posteriorly displaced, and the tympanic and mastoid segments of the FN are antero-inferiorly displaced, running more vertically than normal control. The cochlea (Co), malleus (M), anterior semicircular canal (ASC), and posterior semicircular canal (PSC) are intact. (B) Lateral view of normal control. The green arrowhead shows the course of the FNs.
|
 | Fig. 4(A) The Delta Viewer 3 dimensional (DV-3D) image of case 1 in the same position during cochlear implantation surgery. (B) The DV-3D image of normal control in the same position as (A). Rectangle of dashed line shows the area of Fig. 5. Co, cochlea; ASC, anterior semicircular canal; PSC, posterior semicircular canal; LSC, lateral semicircular canal; FN, facial nerve; M, malleus; I,incus; S, stapes.
|
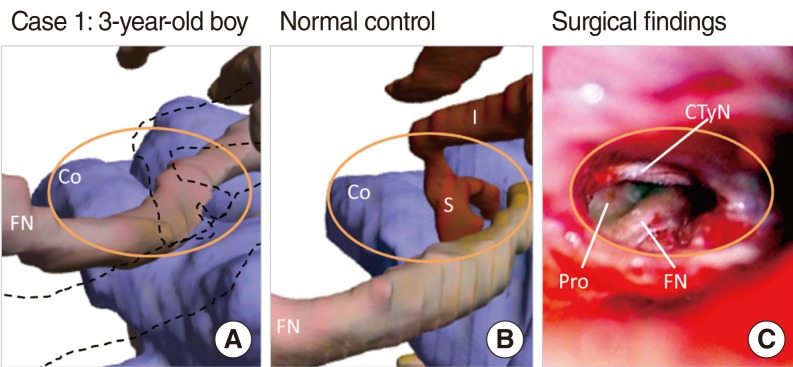
Fig. 5 shows the preoperative DV-3D image and the actual picture of the surgical findings. The space for cochlear fenestration was very narrow; however, we were able to insert an electrode based on the preoperative DV-3D image without any complications, such as FN palsy or stimulation. Fig. 6 shows an X-ray of the electrode: MED-EL, standard.

Case 2: Left ear of a seven-year-old boy
The patient presented with bilateral cochleo-vestibular malformations and abnormalities of the stapes and course of the FN. We had already performed CI surgery on the right ear one year before. We planned a second CI procedure on this patient's left ear for the same reason we performed surgery on the first patient.
The preoperative DV-3D images (Figs. 7, 8) indicate that the shape of the cochlea and the SC are hypoplastic, the stapes seem to be fused to the FN, and the course of the FN is abnormal, as in the previous case, with bifurcation. In addition, the round window niche is closed, so there is no landmark for cochlear fenestration. We were able to successfully perform the cochlear fenestration right next to the FN, which was detected using a FN monitor and referring to a DV-3D image of the nerve course. Fig. 9 shows an X-ray of the electrode: Cochlear, standard.
 | Fig. 7Antero-lateral view of the temporal bone structures of case 2. The shape of the cochlea (Co) and semicircular canals are hypoplastic. The labyrinthine segment of the facial nerve (FN) and geniculate ganglion are posteriorly displaced, the tympanic and mastoid segments of the FN are antero-inferiorly displaced with bifurcation, and the stapes is fused to the facial nerve (arrow head). IAC, internal auditory canal; M,malleus; I, incus; S, stapes.
|
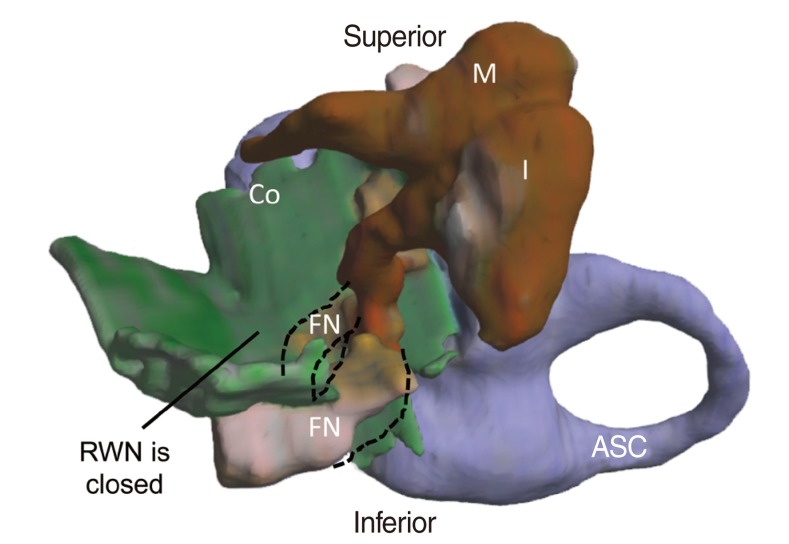 | Fig. 8The Delta Viewer 3 dimensional image of case 2 in the same position during cochlear implantation surgery. The surface of the tympanic cavity is displayed in green. The round window niche (RWN) is closed, so there was no landmark for cochlear fenestration. Co, cochlea; FN, facial nerve; ASC, anterior semicircular canal; M, malleus; I, incus.
|

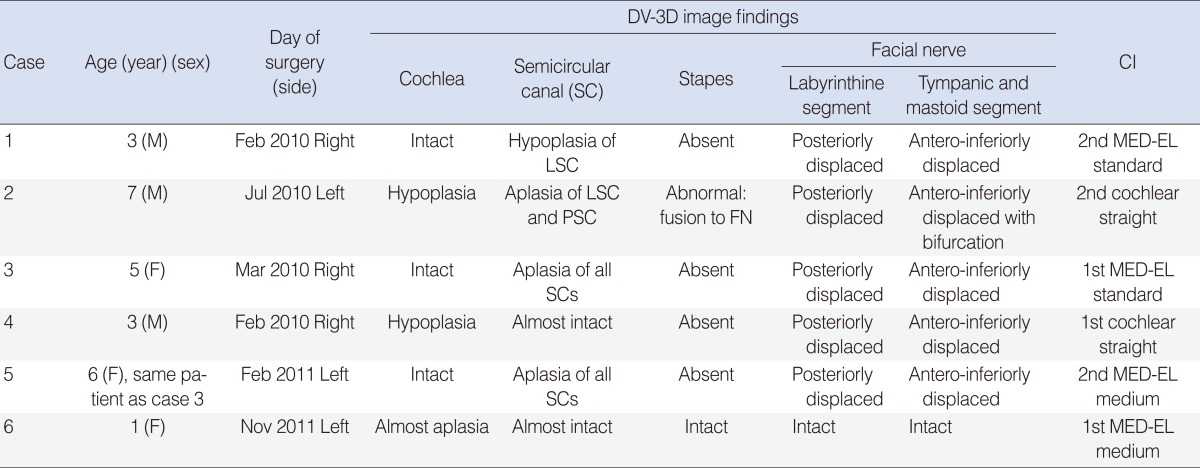
Table 1 consists of a list of the DV-3D images we prepared for 6 separate CI cases that involved ear malformation; in particular, an abnormal course of the FN. In all of the cases, we were able to successfully insert electrodes by referring to DV-3D images with no technical problems. Table 1 suggests that the anomaly of the stapes indicates an abnormal course of the FN.
Go to :
DISCUSSION
We prepared 3D images of patients' ear malformations prior to performing CI procedures on these patients. These 3D images contributed to the successful insertion of electrodes during surgery on these patients, each of whom had an abnormal course of the FN. There is no previous report on the clinical use of 3D imaging for preoperative planning of CI surgery.
We have been able to produce preoperative 3D images using a method we were able to develop at a low cost. Several software products are available that enable us to convert 2D medical images, such as those produced through CT or magnetic resonance imaging, to 3D. However, these imaging techniques are not suitable for creating 3D images of the temporal bone structures, because their resolution is so rough that they were developed generally for use on larger organs such as the lungs, large arteries, etc.
In very recent years, a high-performance multi-slice CT scanner and workstation have made it possible to generate detailed 3D images of the temporal bone structures for radiology diagnostics (1). Some previous articles have reported on the creation of 3D images based on a histological specimen for educational purposes (2-6).
A novelty of our method is that it enabled us to convert structures of different densities-bone structures, such as the ossicles, and soft tissue structures, such as the FN and cochlea-in the same manner on one 3D image. It is especially difficult to reconstruct a FN as a 3D image, because it is difficult to select the FN on a CT image. There is a previous report that investigated automatic FN selection through the use of special computer software; however, this method has not yet been put into use (7). There is room for further improvement in the accuracy of the DV-3D image; however, even now it is quite useful for planning a CI procedure and for avoiding surgical complications.
In this study, we suggest that an anomaly of the stapes indicates an abnormal course of the FN. It is well-established that an abnormal stapes has been associated with an anomalous course of the tympanic and mastoid segments of the facial nerve, because these are derivatives of the second branchial arch (8-10). As the labyrinthine segment of the FN is not derived from the second branchial arch but from the otic cupsule, the cause of the anomaly of this segment may not be discussed on the same basis as that of the other segments related to the second branchial arch.
Go to :
 XML Download
XML Download