

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Carbon dioxide (CO2) laser cordectomy is considered one of the modalities of choice for treatment of patients with early glottic carcinoma [123]. In addition to its comparable oncological results with radiotherapy and open surgical procedures, it offers several advantages including single session therapy, short hospital stay, reduced postoperative morbidity and favorable cost-effectiveness ratio [4567].
Complete eradication of the disease is the principal objective of treatment of malignant tumours of the larynx. However, preservation of laryngeal functions and trial to solve the problem of voice disorders that appear after treatment are other factors that should be considered [8].
Resection of laryngeal tissue, particularly at the level of glottis with the result of fibrous or partially or totally absent vocal cord(s) leads to the development of substitutive phonation mechanisms where some structures of the larynx adapt themselves for creation of voice and this adaptation is different depending on the performed surgical procedure [9].
The aim of this study is to detect how the larynx compensates for voice production after different types of CO2 laser cordectomy for early glottic carcinoma and to assess the vocal outcome.
Go to : 
MATERIALS AND METHODS
This retrospective study included selected 112 patients with dysplasia of the vocal fold or early glottic carcinoma (7 dysplasia, 11 Tis, 74 T1a, 18 T1b with anterior commissure involvement, and 2 transglottic carcinoma with ventricle involvement) who underwent endoscopic CO2 laser cordectomy following the classification proposed by the European Laryngological Society working committee [10] between May 2004 and October 2013 at Otorhinolaryngology Head and Neck Surgery Department, Zagazig University Hospitals. They were 106 males and 6 females with their ages ranging from 29-78 years (mean, 57 years) (Table 1). Patients were selected as being not treated with radiotherapy.
Table 1.
Demographic characteristics of included patients
![]()
Patients were subjected to examination after at least 6 months of surgery. This examination included the voice assessment protocol used in Zagazig University Hospital [11]. This protocol passes through the following levels.
Elementary diagnostic procedures: This includes the patient's interview, the preliminary auditory perceptual assessment (APA) of voice and careful laryngeal examination.
Clinical diagnostic aids: This includes augmentation and documentation of the glottic picture and high-fidelity voice recording. Augmentation of glottic picture was performed with video-stroboscopy using either the rigid oral 70° telescope or flexible nasofibroscope, connected to a camera in association with stroboscopic light. The way of laryngeal compensation for voice production is detected. Phonatory gap was measured subjectively in relation to expected length of the visible part of vocal fold. It was known to be 15 mm in males and 10 mm in females. It was measured at its widest point, regardless its shape. Phonatory gap was graded into (no gap), small gap (from 0.5 to <1 mm), moderate gap (from 1 to 3 mm) and large gap (>3 mm). Patients' voices were recorded with a high-fidelity frequency modulation audio tape system. The speech material recorded included reading a standardized text, counting task and sustained vowel prolongation including /α/, /i/, and /u/ vowels. The recordings were done in a sound-treated room to minimize environmental noise. The recorded materials for all patients were rated for APA by three experienced phoniatricians using a modified GRBAS (grade, roughness, breathiness, asthenia, strain) scale [12]. The APA sheet comprised a 4 point scale (0-3) for determining the items: overall grade of dysphonia, and character of voice including: strained, asthenic, breathy and rough (0 for normal, 1 for mild, 2 for moderate, and 3 for severe). Perceptual voice analysis was done for only 88 patients after exclusion of the voice samples of female patients to make the study population homogenous and the samples of 18 male patients due to bad quality (4 patients) or unavailability (14 patients).
Additional instrumental measures: In this level, acoustic analysis could not be done due to the great deviation of voice from normal in most of cases which was out of range of the device.
Statistical analysis
Scores of GRBAS scale domains of patients of different laryngeal compensation types are compared to those of control group using the Mann-Whitney test, assuming P<0.05 as the minimum significance value.
Go to :
RESULTS
Videolaryngostroboscopic examination of patients of the study which was done at least 6 months after surgery revealed that the larynx can compensate to produce voice after CO2 laser cordectomy through different 5 types (Figs. 1, 2, 3, 4, 5).
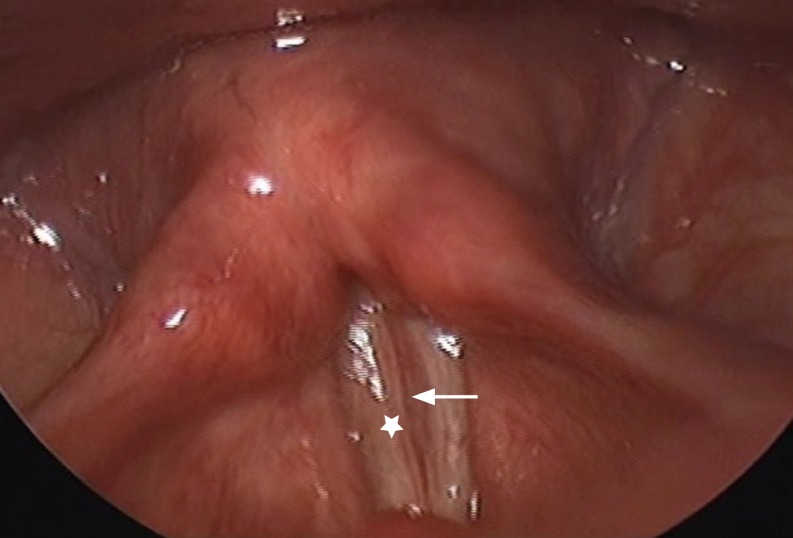 | Fig. 1Type I compensation. The main phonatory site is limited to the healthy true vocal fold (star) and the treated fold (arrow) which showed preserved but reduced and irregular mucosal vibration. No glottic gap is noticed.
|
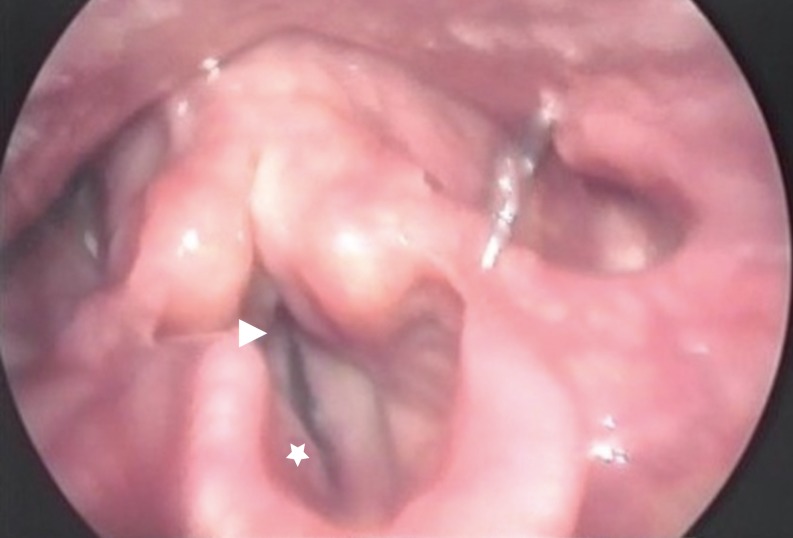
 | Fig. 2Type II compensation. The main phonatory site is limited to the healthy true vocal fold (star) and the treated fold (arrow) that lost its mucosal vibration. Moderate glottic gap is noticed.
|

Type I compensation: it was reported in 14 patients (12.5%), all of them were subjected to type I cordectomy. The main phonatory site of the larynx was limited to the healthy true vocal fold and the treated fold which showed preserved but reduced and irregular mucosal vibration (vocal fold to vocal fold compensation). Small phonatory gap was noticed in only one patient.
Type II compensation: it was detected in 59 patients (52.7%; 5 patients subjected to type I cordectomy, 16 patients subjected to type II cordectomy, 22 patients subjected to type III cordectomy, and 16 patients subjected to type IV cordectomy). The main phonatory site was limited to the healthy true vocal fold and the treated fold which showed absent mucosal vibration (vocal fold to vocal neofold compensation). Associated hyper adduction of the arytenoids together with mild vibration of both ventricular folds was noticed in 12 patients (20.3%) while only associated hyper adduction of the arytenoids was noticed in 3 patients (5.1%). Phonatory gap was noticed in 29 patients (small in 15 patients and moderate in 14 patients).
Type III compensation: it was found in 9 patients (8%), all of them were subjected to type IV cordectomy. The main phonatory site was limited to the healthy true vocal fold and the ventricular fold on the treated side (vocal cord to ventricular fold compensation). Associated hyper adduction of the arytenoids was noticed in 6 patients (66.7%). Phonatory gap was noticed in 4 patients (small in 2 patients and moderate in the other 2 patients).
Type IV compensation: it was found in 20 patients (17.9%; 4 patients subjected to type IV cordectomy and 16 patients subjected to type Va cordectomy). The main phonatory site was limited to both ventricular folds (ventricular compensation). Associated hyper adduction of the arytenoids was noticed in 16 patients (80%). Phonatory gap was noticed in 10 patients (small in 7 patients and moderate in the other 3 patients).
Type V compensation: it was detected in 10 patients (8.9%; 1 patient subjected to type IV cordectomy, 2 patients subjected to type Va cordectomy, and 7 patients subjected to type Vc cordectomy).The main phonatory site was limited to the hyper adducted and hypertrophied arytenoids (arytenoids compensation). Less marked vibration of the mucosa of both aryepiglottic folds was noticed in all patients. Phonatory gap was noticed in 10 patients (moderate in 5 patients and severe in the other 5 patients).
The supraglottic structures sharing in the phonatory compenpasation showed a mucosal wave with an irregular and asymmetric pattern of vibration. The type(s) of laryngeal compensation for voice production seen after each type of CO2 laser cordectomy are shown in Table 2 and the measured phonatory gap in different types of compensation are shown in Table 3.
Table 2.
Relation between types of compensation and types of cordectomy
|
Type of compensation |
Type of cordectomy |
||
|---|---|---|---|
| Type | No. (%)* | Type | No. (%)† |
| I | 14 (12.5) | I | 14 (100) |
| II | 59 (52.7) | I | 5 (8.5) |
| II | 16 (27.1) | ||
| III | 22 (37.3) | ||
| IV | 16 (27.1) | ||
| III | 9 (8.0) | IV | 9 (100) |
| IV | 20 (17.9) | IV | 4 (20.0) |
| Va | 16 (80.0) | ||
| V | 10 (8.9) | IV | 1 (10.0) |
| Va | 2 (20.0) | ||
| Vc | 7 (70.0) | ||
![]()
Table 3.
The phonatory gap in different types of laryngeal compensation
![]()
Perceptual voice analysis
Regarding the overall grade of voice, dysphonia was found in 81 patients (92%) with all of the remaining 7 patients (8%) with no dysphonia belonging to type I compensation. Dysphonia varied in its severity among the 5 types of compensation where it was found to be moderate to severe in 0%, 64%, and 89% of patients of types I, II, and III compensation respectively and in all patients of types IV and V compensation. Roughness was the commonest feature of voice produced through type I compensation (46%) and rated as mild (mean, 0.462) while the least common feature was breathiness that was noticed in only 1 patient (7.7%) and was also mild (mean, 0.077). Voice produced through type II compensation was noticed to be more commonly and more severely impaired for all voice characters than voice produced through type I compensation and roughness was also the most common feature (92%) and rated as moderate (mean, 1.74) but asthenia was the least common change (48%) and rated as mild (mean, 0.64). More common and more severe impairment was noticed in voice produced through type III compensation than in voice produced through type II compensation and roughness, noticed in all patients, was also the common characteristic change and rated as moderate to severe (mean, 2.222) while breathiness was the least common (55.5%) and rated as mild (mean, 0.778). Voice produced by type IV compensation showed higher percentage and more severity of impairment than in type III with roughness and strain found to be the most common features being noticed in all patients compensated by this type and rated as moderate to severe (mean, 2.667) and mild to moderate (mean, 1.333) respectively while breathiness was the least common change (58.3%) and rated as mild (mean, 0.75). In contrary to voice character changes in the first 4 types of compensation, the dominant features of voice produced through type V compensation were breathiness and asthenia being noticed in all patients and both were rated as moderate to severe (mean, 2.5) while roughness and strain were less common and noticed in 2 patients (50%) and both were mild (means, 0.5 and 0.75, respectively).
The degree of severity of each domain change in different types of laryngeal compensation is shown in Table 4. Voice character changes were found to be significant in all types of compensation except for breathiness, asthenia and strain in type I compensation patients.
Table 4.
Scores of GRBAS scale in different types of laryngeal compensation
![]()
Go to :
DISCUSSION
After CO2 laser cordectomy the vocal folds are left with an area of tissue loss which varies according to the type of cordectomy. In order to phonate after CO2 laser cordectomy the larynx has to compensate for this tissue loss. In our study there were noticed 5 different types of natural laryngeal compensation for voice production after CO2 laser cordectomy.
Laryngeal compensation mechanisms for voice production were found to be related to the extent of tissue resection but there was no single type of compensation for each type of cordectomy where type I, type IV, and type V cordectomies were found to be followed by different types of phonatory compensation.
In a review of the literature, voice production mechanisms after endoscopic CO2 laser cordectomy have not been well defined and sporadically reported by few authors. Haddad et al. [13] found that 6 out of 8 patients undergoing types I and II cordectomy showed complete glottic closure and a preserved glottic mucosal wave was seen in 7 patients of this group and was combined with supraglottic vibration in 3 patients. Only one patient showed supraglottic vibration together with laryngeal vestibule hyper constriction. On the other hand, more than half of patients undergoing types III and IV cordectomy showed incomplete glottic closure, absent glottic mucosal vibration and an increased trend to have laryngeal hyperconstriction as a compensating mechanism. Similar findings were reported by Sjogren et al. [14] in patients undergoing types I and II cordectomy where around 60% of those patients had incomplete glottic closure, reduced mucosal wave and signs of ventricular compensatory activity. Krengli et al. [15] have reported that a satisfactory well shaped fibrotic neocord with phonatory compensation in the form of cord to neocord was observed in patients who underwent type III cordectomy while an insufficient neocord with phonatory compensation in the form of vibration of the ventricular bands or arytenoid hyper adduction was evident in patients treated with type IV cordectomy. Motta et al. [16] have described five types of laryngeal compensation after CO2 laser cordectomy based only on the anatomical site of the phonatory neoglottis and these types of compensation are glottal, limited to the healthy vocal fold and the opposite neofold; inferior mixed, limited to the true vocal fold on one side and the false fold on the opposite side; vestibular, limited to the two false vocal folds; superior mixed, limited to the false vocal fold on one side and the aryepiglottic fold on the opposite side; and lastly aditus laryngis, limited to the two aryepiglottic folds. In our study a more detailed description of the laryngeal compensation mechanisms has been mentioned based on the anatomical phonatory site and the condition of the mucosal wave of the treated cord together with mentioning the phonatory gap in the 5 defined compensation types.
As the quality of voice after cordectomy is mainly affected by the vibrating parts of the larynx that compensate for its creation, perceptual voice analysis in the present study was done in correlation with the type of natural phonatory compensation rather than the type of cordectomy and this is supported by the finding that there was no single type of compensation following each type of cordectomy. In our study we could not define a laryngeal compensation type producing voice comparable to that of control subjects in all its characters in terms of auditory perception as voice characters changes were found to be statistically significant in all types of compensation except for breathiness, asthenia and strain in type I compensation which were found to be statistically insignificant when compared with control group and this indicates that voice produced by this type of compensation is the least impaired one in our study.
Most patients of the present study had dysphonia and its degree was progressively increased from mild in type I compensation to severe in type V compensation. This is comparable to the finding of Haddad et al. [13] who have reported that the quality of voice of patients with treated glottic tumors will never be the same as before the disease due to reduced ability for vibration at the site of the resected tissue.
The progressively increased percentage and severity of voice characters impairment in the first 4 types of compensation may be explained by the progressive deviation of laryngeal compensation mechanisms from the normal mechanism of voice production together with the noticed mildly progressive increase of the phonatory gap size through the 4 types. In contrary to voice character changes in the first 4 types of compensation, the dominant features of voice produced through type V compensation were breathiness and asthenia being noticed in all patients and both were rated as moderate to severe (mean, 2.5) while roughness and strain were less common and noticed in 2 patients (50%) and both were mild (means, 0.5 and 0.75, respectively). The noticed differences in the nature of impairment of the produced voice between the first 4 types of compensation and the last type may be explained by the bigger phonatory gap in type V compensation especially at the anterior part of the phonatory site between both aryepiglottic folds resulting in the production of a breathy and weak rather than rough and strained voice. To our knowledge, there is no similar study in the literature comparing the different types of laryngeal compensation after CO2 laser cordectomy in term of auditory perception using GRBAS scale using such large cohort of patients. Therefore, this study gives new and clinically relevant insights into phonatory mechanisms following transoral laser surgery for glottic carcinomas.
Our study specifies the area of compensation of the larynx after different types of CO2 laser cordectomy. It had shown that supraglottic structures especially the ventricular folds and the arytenoids share as important compensatory sites for voice production either unilaterally or bilaterally after types IV and V cordectomies reflecting the importance of their preservation during these extensive types of cordectomies unless their resection is oncologically indicated.
The present study showed also that a single type of cordectomy may be followed by different types of compensations which indicate that the degree of tissue resection may not be the only factor that determines the type of compensation and other factors are to be addressed. Patients included in our study did not receive voice therapy after cordectomy and so further studies are needed to assess the role of voice therapy and its effect on compensation in such patients.
In conclusion, the larynx can compensate after CO2 laser cordectomy for voice production by different 5 mechanisms producing voice of different characters and different degrees of impairment. None of the compensation types produced voice comparable to normal voice. The supraglottic structures especially the ventricular folds and the arytenoids are to be preserved during CO2 laser cordectomy when possible.
Go to :
 XML Download
XML Download