

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Molecule-based diagnosis has improved the clinical utility of allergy tests. Recently, the component-resolved allergen microarray chip technique was introduced to the molecule-based diagnostic allergology field. In contrast to the traditional specific IgE assays, this method does not use whole extracts from allergens but instead uses multiple purified natural and recombinant allergen components spotted onto a microarray plate [1]. The older specific IgE test can detect only one allergen even though a patient may be sensitized to multiple allergens. However, the microarray technique can be used to determine specific IgEs against multiple allergens simultaneously and even allow the determination of the IgMs and IgGs at the same time. It also explains the cross reactions between allergens by confirmation of the cross-reactive allergen [2].
The Immuno Solid-phase Allergen Chip (ImmunoCAP ISAC, Phadia, Uppsala, Sweden) is a commercially available microarray-based IgE detection chip. It allows for the measurement of specific IgE antibodies to 112 allergen components of 46 major allergens in a single measurement with a minimal amount of blood or serum (30 µL) for testing, and thus this technique offers opportunities to establish individual allergy profiles [3456]. The sequential screening of the components of one or more allergens with a library has been used to diagnose several food allergies [789]. This microarray allergen chip has recently been introduced into clinical allergologic research as this tool will hopefully be useful for the measurement of serum IgEs in allergic patients with atopic dermatitis [1011].
However, there have been few studies on the clinical utility of a microarray allergen chip test for allergic rhinitis patients. Therefore, the aim of this study was to evaluate the ImmunoCAP ISAC and compare it with the established method of ImmunoCAP IgE detection.
MATERIALS AND METHODS
Patients
One hundred sixty-eight allergic rhinitis patients were included in this study. All patients were adults over 18 years old. All the patients were diagnosed with allergic rhinitis by their clinical symptoms, physical examination and a positive skin prick test. The wheal reaction was greater than 3+. Ninety-five patients were allergic to house dust mites (Dermatophagoides farine [DF] and Dermatophagoides pteronyssinus [DP]), 23 were allergic to the fungus Alternaria alternata, 23 were allergic to birch, and 26 were allergic to mugwort. The mean age of the patients was 26.6±10.2 years old. The male to female ratio was 113:53. This study was approved by the Institutional Review Board of Gachon University Gil Medical Center.
Methods
Skin prick test
A skin prick test was performed (Allergen kit, Allergopharma, Reinbek, Germany). The allergic reaction was defined as positive when the weal reaction exceeded 3+.
Laboratory analysis: specific IgE and allergen microarray immunoassay
We analyzed the presence of specific IgEs using ImmunoCAP for house dust mites (DP and DF), A. alternata (m6), birch (Betula verrucosa) (t3), and mugwort (Artemisia vulgaris) (w6). A positive value was defined when the level of allergen-specific IgE was greater than 0.34 kU/L.
To define the allergen components, we used a microarray-based IgE detection chip, the Immuno Solid-phase Allergen Chip (ImmunoCap ISAC ver. CRD-50, VBC Genomics Bioscience Research GmbH, Vienna, Austria) according to the manufacturer's instructions [5]. This microarray chip allows the measurement of 112 allergen components of 46 allergens. Therefore, we selected the major components of house dust mites (nDer p 1, nDer p 2, nDer p 10, nDer f 1, and nDer f 2), birch (rBet v 1 and rBet v 4), mugwort (nArt v 1 and nArt v 3), and Alternaria (rAlta1 and rAlta6). A positive value was defined when the ISAC standardized units (ISU) were greater than 0.3.
The recommended method for the allergen microarray is as follows. The purified natural and recombinant allergen components were spotted on the allergen microarray chip. After incubation with 20-µL undiluted serum from allergic patients for 180 minutes at room temperature in the humid chamber, slides were rinsed and washed for 15 minutes in TBS-T (TBS-T buffer, 150 mM sodium chloride, 10 mM Tris base, and 0.5% Tween 20, pH 8.0), for 5 minutes in deionized water and dried. To detect bound IgE antibodies, allergen chips were incubated for 60 minutes at room temperature with 20 µL of a fluorescence-labelled antihuman IgE antibody. After a rinsing and washing procedure, the slides were dried completely. The slides were scanned with a laser scanner (LuxScan 10K, CapitalBio, Beijing, China). The analysis of the microarray image data was performed with ImmunoCAP ISAC Xplain (Phadia).
RESULTS
House dust mites
In cases of allergy to DP or DF, the sensitivity of the specific IgE to skin prick test was 80%, and that of the allergen microarray was 78.9%.
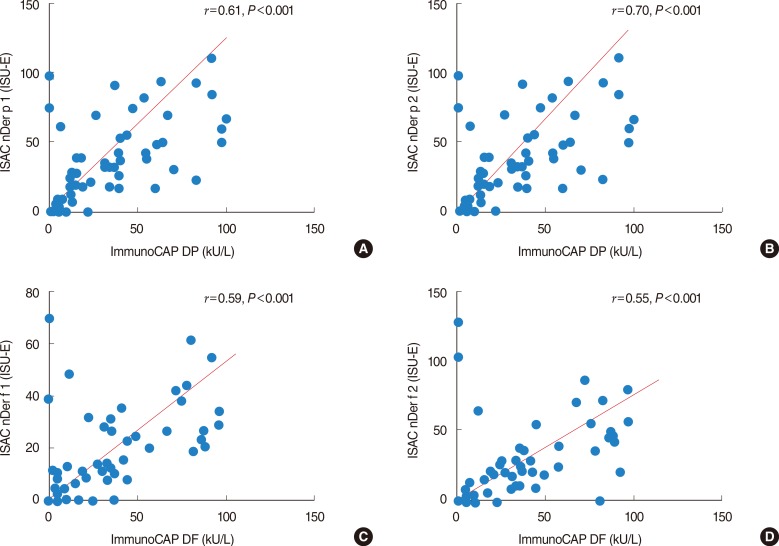
The agreement rate between the specific IgE and allergen microarray 98.6% (positive number in allergen microarray/positive number in specific IgE, 75/76). The Kappa value was 0.774 (Fig. 1A). The sample correlation coefficient for nDer p 1 was 0.61, and the P-value was <0.001 (Fig. 2A). The sample correlation coefficient for nDer p 2 was 0.70, and the P-value was <0.001 (Fig. 2B). The sample correlation coefficient for nDer f 1 was 0.59, and the P-value was <0.001 (Fig. 2C). The sample correlation coefficient for nDer f 2 was 0.55, and the P-value was <0.001 (Fig. 2D).
Fungus, birch, and mugwort
In cases of A. alternata (m6), the sensitivity of the specific IgE was 91.3%, and that of the allergen microarray was 76.9%. The agreement rate between the specific IgE and allergen microarray 47.6% (positive number in allergen microarray/positive number in specific IgE, 10/21). The Kappa value was 0.551 (Fig. 1B). In cases of birch (B. verrucosa) (t3), the sensitivity of the specific IgE was 86.9%, and that of the allergen microarray was 43.6%. The agreement rate between the specific IgE and allergen microarray 50% (positive number in allergen microarray/positive number in specific IgE, 10/20). The Kappa value was 0.511 (Fig. 1C). In cases of allergy to mugwort (Artemisia vulgaris) (w6), the sensitivity of the specific IgE was 92.3%, and that of the allergen microarray was 69.2%. The agreement rate between the specific IgE and allergen microarray 50% (positive number in allergen microarray/positive number in specific IgE, 18/24). The Kappa value was 0.670 (Fig. 1D).
DISCUSSION
The findings of this study demonstrate that the results of the ISAC were comparable with the results of the traditional ImmunoCap IgE detection for house dust mites. However, in cases of A. alternata, birch and mugwort, the ISAC was less sensitive than the allergen-specific IgE detection method.
Microarray testing for allergen-specific IgEs can be presumed to be the method of choice for a prospective component-resolved diagnosis of type I allergy [12]. There is still controversy about the sensitivity of this microarray method compared with traditional IgE tests. The ISAC is known to have higher variability when the serum IgE level is low. Variable results in the analysis of certain allergens and some limitations in the types of allergen sources have also been shown [13]. The microarray has a good dynamic range, similar to that of the CAP/RAST system. The microarray and UniCAP showed comparable analytical sensitivity, exceeding the skin test [12]. A comparison of these two tests revealed that they were equally relevant in the diagnosis of patients allergic to grass, birch and cats. However, the microarray is slightly less sensitive for the diagnosis of house dust mite-allergic patients and less sensitive in mugwort allergies [14]. The ISAC CRD103 and whole-allergen CAP showed similar high sensitivity and specificity in diagnosing grass and cypress pollen allergies [15]. A comparison of the ISAC with the ImmunoCAP 250 revealed that the concordance rate was 78.65% and that the concordance rate was 93.75% for negative results. No nonspecific binding was observed [16]. In the nDer p 1, nDer p 2, and nDer p 10 analyses, the ImmunoCAP and ISAC were concordant, but the quantitative correlation was poor [17]. There was no clinical implication for this difference. The reproducibility of the ISAC was good. The positive percent agreement varied between 75% and 100% for sIgE levels above 1 kUA/L [18]. Our results showed that the two tests have almost the same sensitivity for house dust mites. However, the ISAC sensitivity was very low for A. alternata, birch, and mugwort compared with the results of previous studies. We believe that the ImmunoCAP has included all the components of the allergen extracts; however, the ISAC has included some limited types of components from one allergen source. These allergen components might suggest a lower sensitivity in the ISAC compared with the ImmunoCAP.
In the ImmunoCAP ISAC tests, the IgE antibody levels are reported in 4 levels using the ISU-E, which contrasts with the kU/L measurements in the ImmunoCAP with 6 classes. This difference in the measurement units with the same IgE levels might influence the interpretation of a positive level between the two tests. A component-resolved allergy diagnosis with recombinant allergens reveals that the IgE reactivity profiles to individual birch pollen allergens vary among European populations [19]. Our results might distinguish the characteristics of the Korean people with this microarray chip test.
Recently, the WAO-ARIA-GALEN consensus document on molecule-based allergy (MA) diagnostics provided a practical guideline for MA diagnostics. One of the most important implications of an MA diagnosis is its ability to distinguish genuine sensitization from sensitization due to cross-reactivity [13].
In contrast, a microarray allergen chip can be the parameter that decides whether to start immunotherapy or to monitor the effects of immunotherapy. An MA diagnosis distinguishes the major allergens between ragweed and mugwort pollen allergies and has also shown extensive cross-reactivity for both groups. Therefore, it provides the major allergen information for the appropriate immunotherapy [20]. Some authors have reported that immunotherapy for house dust mite allergies seems less efficient than immunotherapy with pollen allergens and that the treatment for house dust mite allergies has a high rate of side-effects [2122]. The microarray allergen chip includes purified major allergens (i.e., nDer p 1, nDer p 2, nDer f 1, and nDer f 2), which are major components of the immunotherapy therapeutic allergen extracts [2324]. Therefore, using the microarray allergen chip, a clinician can identify the patients suitable for immunotherapy with a nDer p/nDer f extract. In cases of patients with broad-reactive components such as nDer p 10, the immunotherapy for house dust mite may have less effect on those patients [24]. In addition, the microarray allergen chip can be used to monitor the effects of immunotherapy. With a minimal amount of blood or serum, the changing levels of allergen-specific IgGs after immunotherapy can be evaluated. However, further large-scale studies are needed before the allergen microarray can be used in daily clinical practice.
In conclusion, the results of this study suggest that the allergen microarray is a reliable method to diagnose allergic rhinitis to DP and DF. Further study on the utility of the allergen microarray is needed.

 XML Download
XML Download