

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Malformations of the external ear are common birth defects, and congenital aural atresia (CAA) is often associated with auricular and middle ear deformities. The state of the auricle can be classified into 3 types, as described by Marx. The external auditory canal (EAC) anomaly varies from slightly narrow to complete atresia [12]. Congenital external auditory canal stenosis (EACS) is defined by Jahrsdoerfer et al. [2] as an EAC with a diameter of less than 4 mm [3]; it is typically regarded as incomplete atresia, and thus its temporal computed tomography (CT) imaging characteristics have been neglected. The surgical management for CAA/EACS is aimed at improving hearing and at establishing appropriate auditory canal status for the application of hearing aids. In clinical practice, we found that patients with EACS have better postoperative hearing improvement and fewer postoperative complications than those with CAA [3]. We speculate that an increasing number of patients with EACS will choose surgery to improve their hearing and life quality in future. By quantitatively analyzing the temporal CT imaging in patients with EACS, and comparing those with images from patients with CAA and normal canals, we further understand external and middle ear development to improve surgical candidacy selection and avoid unnecessary complications.
Generally, the most important information the otologist requires from CT includes the following: (1) the status of the ossicular chain; (2) the degree of development and pneumatization of the tympanic cavity; (3) the course of the facial nerve; and (4) the position of the tegmen mastoideum. This study will focus on the auricle and canal development as well as the above 4 parameters.
Go to : 
MATERIALS AND METHODS
Ethics statements
This study was reviewed and specifically approved by the Ethics Committee of the Eye & ENT Hospital of Fudan University. Informed consent was obtained from all participating subjects. The written informed consent was given by participants (adults) and next of kin/caregiver (children) for their clinical records to be used in this study.
Sample collection: patients and normal controls
This study was performed by retrospective analysis in departments of the Eye & ENT Hospital. A total of 71 patients with microtia combined with either unilateral or bilateral CAA/EACS, who partly accepted the staged reconstruction of the auricle or external ear meatus between December 2008 and December 2011, were selected for enrollment. Forty-six normal ears of the unilateral microtia with atresia or stenosis patients were included as controls. All control ears have normal auricles, normal external auditory canals, intact tympanic membranes, and normal pure tone audiometry results. None of the individuals had a known history of general otitis media or previous surgery. Their demographic characteristics are shown in Table 1.
HRCT imaging protocols
Spiral temporal bone HRCT scans (Siemens Sensation 10, Munich, Germany) were taken with a continuous 0.75-mm slice thickness, 0.25-mm interval of data set reestablishment, 140 κV, 100 mAS, and a 512×512 matrix. After the imaging data were stored as Digital Imaging and Communication in Medicine files, they were imported to a personal computer that ran Mimics 10.0 software (The Materialise Group, Leuven, Belgium). Each measurement was performed three times.
Parameters evaluation and measurement
Dimension 1: microtia classification by Marx
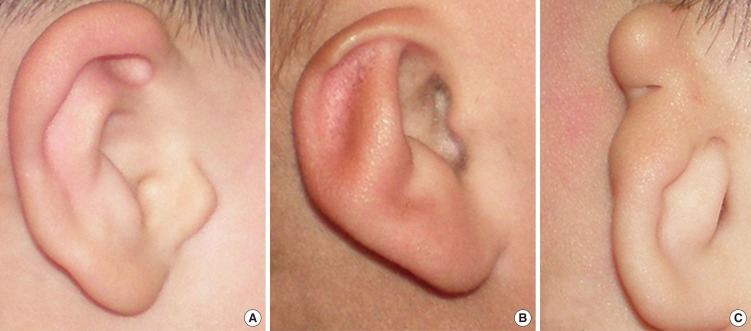
The severity of microtia is classified into grades I, II, and III according to the classification of Marx (Fig. 1). Grade I microtia exhibits only mild deformity, with the auricle being slightly smaller than normal, each part of which can be clearly distinguished. In grade II microtia, the size of the auricle is one half to two thirds of the normal size, and its structure is only partially retained. In grade III microtia, the auricle is severely malformed and usually exhibits a peanut shape. For each group, the auricle is classified according to the Marx classification.
Dimension 2: medial canal diameter
In the axial plane, the distance is measured from the vertical facial nerve (VFN) to the posterior aspect of the superior glenoid fossa (Fig. 2). To measure this dimension, one finds the axial image that captures the first complete cut of both the most superior aspect of the temporomandibular joint (TMJ) space and the VFN.

Dimension 3: vertical facial nerve anterior displacement
In the axial plane, we first located the foramen spinosum (FS) position due to its stability and drew a horizontal line through the middle point of the FS in Mimics software (Fig. 3). Then, we separately measured the distance from the starting and ending points of the VFN to the coronal plane where the horizontal line stays. The measurement data can show whether the VFN anteriorly displaces.
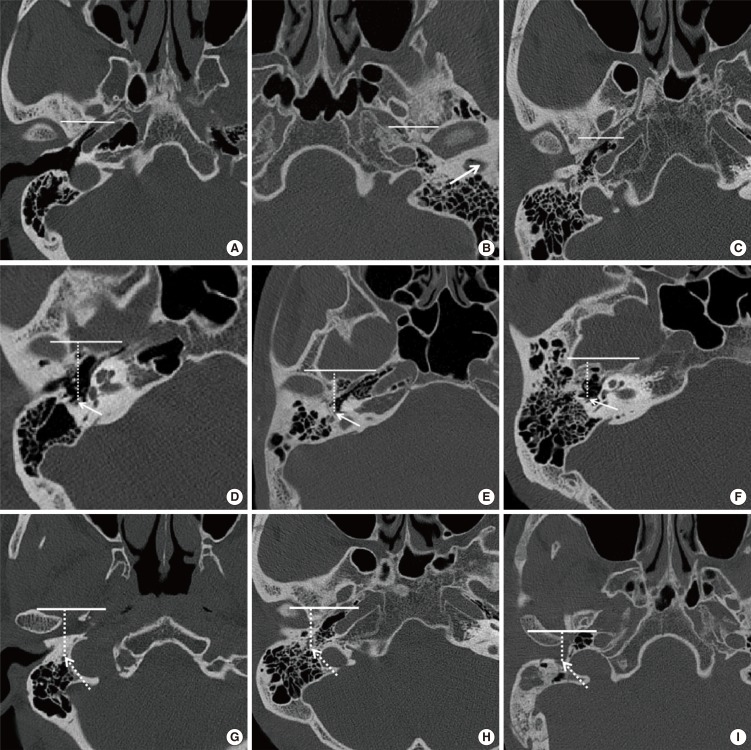 | Fig. 3Vertical facial nerve (VFN) position. The distance (dashed line) from the VFN to the coronal plane passing through the middle point of the foramen spinosum. Right normal ear (A, D, G), stenosis ear (B, E, H), right atresia ear (C, F, I). The line shows the horizontal line located in the coronal plane; the arrow shows stenosis of the canal in panel B and the starting point of the VFN in panels (D), (E), and (F); the dashed arrow shows the ending point of the VFN.
|
In aural atresia, the second genu is often located more anteriorly than usual, and the descending mastoid facial nerve will frequently curve anteriorly toward the area of the round window niche (Fig. 4) and the oval window niche.

In addition, in our study, we found the tympanic portion of the facial nerve (FN) displaced in the lateral wall of the tympanic cavity in one atresia case with the ossicular chain absent (Fig. 5).

Dimension 4: tegmen mastoideum position estimate
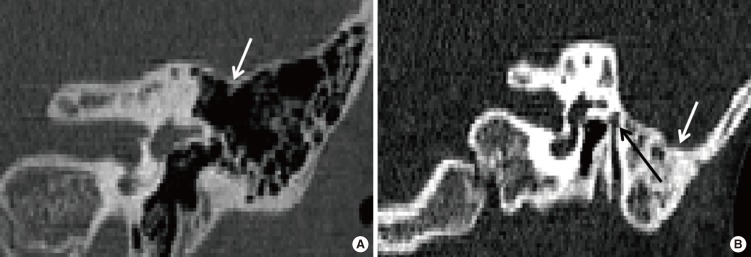
In a CT image, one determines this dimension by finding the coronal plane which captures the lateral semicircular canal (LSCC), oval window and tegmen mastoideum, and drawing the shortest line from the middle point of the LSCC caliber to the tangent through the lowest point of tegmen mastoideum. The tegmen mastoideum may be inferiorly displaced, sagging downward (Fig. 6B) or in a normal position (Fig. 6A). The distance was measured as inferiorly displaced if it was judged that the tegmen might obstruct or partially obstruct surgical access to the attic and/or middle ear during a lateral approach.
Dimension 5: tympanic cavity volume
In Mimics software, a 3-dimensional (3D) volume reconstruction of the phantom is created for each protocol using a lower threshold of -1,024 Hounsfield units (HU) and an arbitrary upper threshold of -221 HU. Threshold selection is critical to accurate volume measurement. Setting the threshold too high risks the inclusion of soft tissues with lower density, while setting the threshold too low excludes some air spaces. Air within the external auditory canal was visible on the 3D reconstruction and was excluded from the measured volume.
We defined the walls of the tympanic cavity on the axial planes as follows: the tympanic membrane (nonatretic ear) or the atresia plate (atretic ears) and its surrounding bony tissue were defined as the lateral wall, the medial bony wall of the tympanic cavity as the medial wall, the tegmen as the superior wall and the bony floor of the tympanic cavity as the inferior wall. We defined the anterior wall as the Eustachian tube opening and the carotid artery, and we defined the anterior border of the antrum as the posterior wall.
Dimension 6: malleus-incus complex or malleus-incus joint area
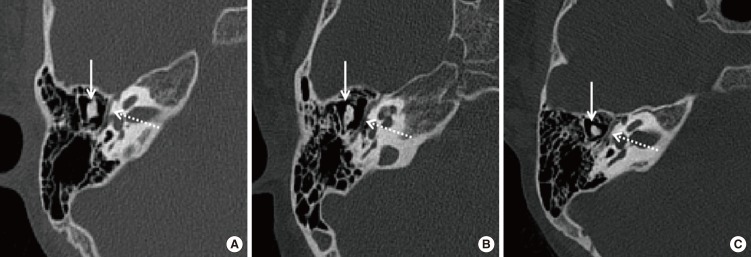
In the axial plane, the incudomalleolar ossicular status was evaluated and the maximum malleus-incus complex (MIC) or malleus-incus joint (MIJ) surface area was measured on the plane where the cochlea and the horizontal FN canal could be visual-ized (Fig. 7). The area directly indicated the MIC developing condition.
Statistical analysis
The following statistical methods were used for comparison. A one-way analysis of variance and the Bonferroni correction were used to compare those 6 parameters and age distribution. A chi-square test was used for microtia distribution in Marx classification. STATA ver. 10.0 (StataCorp LP., College Station, TX, USA) was used for the final comparative analysis. P<0.05 was considered statistically significant.
Go to :
RESULTS
There were no significant differences between the age distribution in the three groups (P>0.05). However, there were significant differences in three groups (P<0.05) regarding the medial canal diameter and the MIC or MIJ area. The microtia distributions in the Marx classification in these three groups were also significantly different (chi-square test, P<0.001). In the Marx classification, the auricle mainly manifested as III, II degree and normal auricle in the CAA, EACS, and normal groups, respectively. Eighty-six percent (31 of 35) of ears with major microtia (third-degree dysplasia) had an atresia; in 54.8% (23 of 42) of the minor microtic (first-degree or second-degree) ears, the bony or cartilaginous part of the EAC was stenotic. Measurement data also showed the potential medial canal diameter of the atresia group was obviously smaller than the stenosis group's (P<0.001). Although the VFN was more anteriorly displaced in starting point and ending point in patients with CAA than in those with EACS, the difference was not significant (P>0.05). For patients with CAA/EACS, their VFNs in starting point and ending point were more anteriorly displaced than in those with normal canals (P<0.05). The tegmen mastoid position differed slightly but not significantly (P>0.05) across the three groups. Moreover, the average tympanic cavity volume in the atresia group was 0.36 cm3, compared to 0.40 cm3 in the stenosis group and 0.57 cm3 in the normal group. The average MIC or MIJ area was 15.63 mm2 in the atresia group, compared to 20.20 mm2 in the stenosis group and 21.54 mm2 in the normal group (P<0.001).
Go to :
DISCUSSION
The prevalence of aural atresia or stenosis varies from 55% to 93% [4]. Generally, congenitally malformed canals can be classified into bony stenosis, membranous atresia and bony atresia. In the membranous type, there is a soft tissue plug at the position of the tympanic membrane, whereas bony stenosis is characterized by the presence of a bony plate at the level of the tympanic membrane [5]. This is the first report to compare the three groups' preoperative temporal CT imaging. Our results indicated that there indeed extensive anatomical variations between the three groups, and we discovered some results that contradict existing knowledge.
Microtia is usually accompanied by atresia or stenosis of the EAC. For the degree of microtia, various classifications have been made according to the severity of the existing malformation. The first classification was created by Marx in 1926. Different classification systems were described later by Jahrsdoerfer and Aguilar (1988), Altman (1955), Lapchenko (1967), Gill (1969), Rogers (1974), Tanzer (1977), and Tasse (2005) [6]. We used Marx grading to assess the auricle development in patients with congenital malformed canals. The study indicated the auricular development mainly manifested as degree III, II and normal in the atresia group, the stenosis group and the normal group, respectively (P<0.001) (Table 2). In addition, 86% (31 of 35) of ears with major microtia (third-degree dysplasia) had an atresia; in 54.8% (23 of 42) of the minor microtic (first-degree or second-degree) ears, the bony or cartilaginous part of the EAC was stenotic (Fig. 8). Compared with CAA ears, the auricle development was better in EACS ears. This finding can help otologists to predict the EAC development status from the auricle appearance in an outpatient before physical examination and further CT inspection.
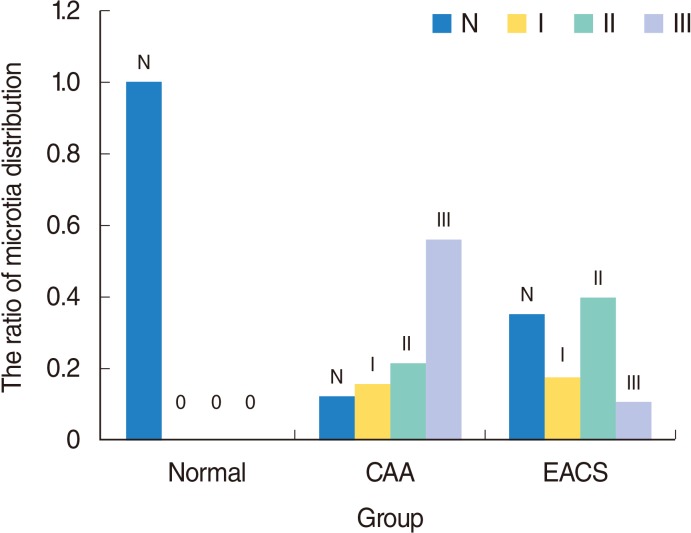 | Fig. 8The microtia distribution in Marx classification in the three groups. N represent normal auricle. Grades I, II, and III represent different deformity of auricle in Marx classification. CAA, congenital aural atresia; EACS, external auditory canal stenosis.
|
With external auditory canal atresia or stenosis, adjunct skull base structures tend to migrate toward to the area ordinarily occupied by the external canal. The TMJ is higher than usual and posteriorly displaced. The distance between the mastoid facial nerve and the TMJ is shortened [7]. Surgery for congenital CAA/EACS is one of the most challenging and difficult procedures in otology because this condition is often accompanied by various temporal bone anomalies, such as an aberrant FN [8910]. In aural atresia, the second genu is often located more anteriorly than usual, and the descending mastoid FN will frequently curve anteriorly toward the area of the TMJ [11], occasionally laterally displacing the lateral wall of the tympanic cavity (Fig. 5) [12]. Through statistical analysis, we see that for patients with CAA/EACS, the VFN starting point and ending point was more anteriorly displaced than in those with a normal canal (P<0.05). We also observed that the VFN is more anteriorly displaced in starting point and ending point in patients with CAA than in those with EACS, but this difference was not significant (P>0.05). Therefore, there is possibly a shorter distance to reach the facial canal in deformed ears during a canaloplasty or tympanoplasty compared with normal ears, and theoretically, the probability of an FN injury may be more and the operation may take more dangerous.
The medial canal diameter [13] is the distance from the VFN to the bony posterior wall of TMJ. The dimension is the shortest distance from the FN to the most posterior aspect of the TMJ and is an indicator of the medial diameter of the EAC, or its potential diameter in atretic and stenosis ears. It incorporates the key surgical anterior boundary, the TMJ, and posterior boundary, the FN. The average medial canal diameter was 6.98 mm in the atretic group, 9.18 mm in the stenosis group and 11.23 mm in the normal group (P<0.05). Jahrsdoerfer et al. [14] reported the average distance between the mandibular condyle and the anterior face of the mastoid bone was 11.58 mm on the atretic side, 13.02 mm on the stenosis side and 18.36 mm on the normal side. Lumbroso et al. [9] reported that 16% of temporal mandibular joints had posterior positions in sixty-seven cases of CAA/EACS. For patients with CAA/EACS, the temporal mandibular joint backward-shift is directly caused by abnormal EAC formation due to the temporal tympanic portion hypoplasia. TMJ backward-shift, together with VFN anterior displacement, leads to medial canal diameter that is smaller in patients with CAA than those with EACS. The distance from the VFN to the bony posterior wall of the TMJ is a safe surgical margin for canaloplasty; hence, there will be a much larger operation space in EACS patients than in those with CAA. Considered with the above finding that the VFN position was not statistically significant (P>0.05) between the CAA and EACS, we speculate that the TMJ backward-shift contributed more to the reduction of the medial canal diameter.
Whether for the general otitis media surgery or ear canaloplasty, the tegmen mastoideum is the safe operative superior margin. If the tegmen mastoideum is in a relatively inferior position, even associated with the low-lying middle cranial fossa [15], it may limit access to the attic and middle ear during a lateral approach; this may preclude atresiaplasty, or possibly make atresiaplasty difficult because the otologist tends to work parallel to the tegmen mastoideum during atresiaplasty [16]. Dedhia et al. [17] reported a qualitative anatomic analysis of 130 CT scans (98 children, 32 bilateral) of CAA/EACS; approximately 13% of the ears had mild inferior displacement of tegmen, and 4% had a significantly obstructing tegmen. We quantitatively analyzed the position change of the tegmen and its relationship with the LSCC in different developmental canals. A low-lying position of the tegmen seemed more prevalent in atretic group than in the stenosis and normal groups in clinical practice. However, we did not detect any significant differences between CAA ears and EACS ears, or CAA/EACS ears and normal ears (P>0.05) (Figs. 9, 10). This may be a false appearance due to the hypoplastic nature of the tympanic cavity and mastoid aeration in such patients. The finding implies there may be a low correlation between the tegmen and EAC development. Therefore, we can see the safe operative superior margin is not different in a lateral approach and its position difference can be ignored in cases of atresia, stenosis and normal canal patients.
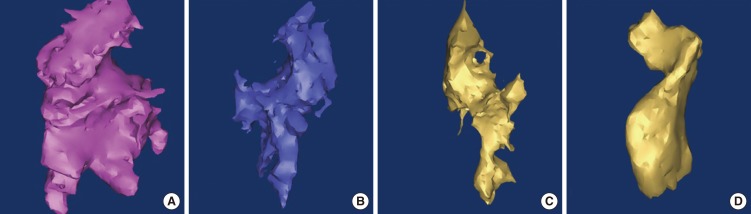 | Fig. 9Three-dimensional reconstruction tympanic cavity in left normal ear (A), in left stenosis ear (B), in left atresia ear (C, D).
|
 | Fig. 10Comparison results of different parameters. Data are the mean±SD. MCD, medial canal diameter; VFN-FS, distance from vertical facial nerve (VFN) to the coronal plane through the middle point of foramen spinosum; LSCC-TM, distance from the middle point of lateral semicircular canal caliber to the tangent through the lowest point of tegmen mastoideum; TCV, tympanic cavity volume; MIC, malleus-incus complex; CAA, congenital aural atresia; EACS, external auditory canal stenosis. *P<0.05, statistical significance in pair-wise comparison. †The starting point of VFN. ‡The ending point of VFN.
|
The size of the tympanic cavity is extremely important for tympanoplasty. First, underdevelopment of the tympanic cavity will pose additional difficulty [10] to the otologist by limiting the space of the surgical field [16]. Second, the tympanic cavity has a close relationship with hearing [13]; the lack of tympanic cavity aeration can be a sole anatomical factor predictive of a poor audiometric outcome [18]. Considering these 2 factors, we chose to measure the tympanic cavity volume. At present, there are two methods used in evaluating the tympanic cavity aeration. One method is measuring the width of the tympanic cavity, which is simple but not accurate [192021]. The other method is measuring the volume using three dimensional reconstructions [192021], which is more accurate. We chose the second method. The mean tympanic cavity volume was 0.36 cm3 in the atresia group, 0.40 cm3 in the stenosis group and 0.57 cm3 in the normal group (P<0.05). Ikui et al. [19] estimated normal tympanic cavity volumes to be 0.45 cm3 in infants and 0.61 cm3 in adults. Osborn et al. [22] reported the average tympanic cavity volume of the atretic ears (mean age, 4.7 years) was 0.34 cm3 compared to an average of 0.51 cm3 for the nonatretic ears. This result implies that the EACS ears have a more well pneumatized tympanic cavity than CAA ears, which supports our surgical outcome that EACS patients have better postoperative hearing improvement than CAA patients [22]. By considering the development of EAC status and tympanic cavity volume, the otologist may be able to better assess surgical candidacy.
Except for the stapes, the ossicular chain develops from Meckel's cartilage and Reichert's cartilage simultaneously, and the incus and malleus are generally involved together in aural atresia cases [10]. In CAA/EACS ears, ossicle anomalies include malleus-incus fusion [9] and partial or total absence of ossicles [2324]. In this study, MIC or MIJ area was measured in two dimensions to indicate the development status of ossicles. We did not measure the area of the stapes, for its display is not clear, but we confirmed its status in surgery for surgical patients. The average MIC/MIJ area was 15.63 mm2 in the atresia group, compared to 20.20 mm2 in the stenosis group and 21.54 mm2 in the normal group (P<0.001). The measurement demonstrates that MIC/MIJ development in EACS patients is better than in CAA patients, and in EACS/CAA patients the MIC/MIJ development is worse than in those with normal ears. MIC/MIJ hypoplasia or fusion obstructs the sound conduction, which leads to different degrees of hearing loss in CAA/EACS [25]. The incus and malleus were underdeveloped, and these have to be considered during reconstructive surgery, such as partial ossicular replacement prosthesis.
Based on the above discussion, we can see the significant temporal structural differences between the CAA and EACS groups. Congenital EACS, as a special canal status, should not merely be regarded as incomplete atresia but should be regarded as an independent disease. In addition, we find that there were no significant differences between CAA ears and EACS ears (P>0.05) for the position of the tegmen mastoideum and the VFN. We were not able to demonstrate correlations between anatomic findings and hearing outcomes because of the small number of atresiaplasty cases, variable times of audiologic testing, and missing data. More research needs to be performed in the future. Therefore, the study should be interpreted as purely anatomic, with the finding of the dramatic anatomic differences for the auricle, canal, FN, tympanic cavity and MIC in patients with CAA, EACS, and normal canals.
In conclusion, the mal-development of external auditory canal is significantly associated with the auricle, middle ear developmental anomalies. Compared with CAA ears, EACS have better development of the auricle, canal, tympanic cavity and MIC and relatively safer surgical operation except for the position of the tegmen mastoideum and the VFN.
Go to :
 XML Download
XML Download