

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Hearing-impaired individuals, especially with sensorineural hearing loss (HL), are known to have substantial difficulty in understanding speech in noisy environments based on the hearing threshold level and configuration. Directional (DIR) microphone feature of the digital hearing aid was designed to provide improvement in terms of signal to ratio (SNR) that can be a primary factor for speech intelligibility in background noise, which relatively enhances sensitivity of microphones to signals arriving from front direction than other directions [123].
Benefit from DIR processing can be calculated as the difference in speech recognition performance in background noise between the DIR and the omnidirectional (OMNI) modes of the same hearing aid. Many previous studies have reported the significant DIR benefits in laboratory settings by using modified Hearing In Noise Test (HINT) and Connected Speech Test (CST) [45679] even though the benefits in a real-world seems unclear due to situational variance of noise configuration [1011]. The range of mean DIR benefits measured in laboratory settings were approximately from 3 to 5 dB SNR which were significantly substantial since improvement in 1 dB SNR resulted in 10%-20% increment of speech intelligibility [12]. Researchers also informed preference for DIR mode over OMNI mode in laboratory studies [7]. In addition to the objective measurement, some researchers attempted to find out DIR processing has actual effects on everyday speech understanding in a real-world by subjective evaluation using questionnaires. However, recent studies did not show significant benefit of or preference for DIR processing [1113].
It has been reported that the magnitude of DIR benefit can be influenced by various environmental factors including visual cue, SNR, noise configuration, hearing aid vent size, or reverberation [137101415]. However, intersubject difference in DIR benefit was not explained by age [16], users' physical characteristics, hearing threshold [6], and configuration of HL [1417] in other studies. Furthermore, Keidser et al. [14] brought up a likelihood of the effect of cognitive performance on DIR benefit even though the effect was small in that study. Taken together, it seems unclear that there are definitive individual factors affecting the DIR benefit although it is important to predict the DIR benefit during counseling of hearing aids in a clinical setting. Therefore, the aims of this study were (1) to find and compare the effect of DIR processing of two different hearing aids via both subjective and objective methods, (2) to determine the association between the results of the subjective and objective evaluations, and (3) to find out individual predictive factors for the DIR benefit, including usage duration of hearing aid, word recognition score (WRS), and bilateral or unilateral hearing aid experience.
Go to : 
MATERIALS AND METHODS
Participants
Twenty-six hearing impaired listeners (10 males, 16 females) with sensorineural HL participated in this study, and they have used monaural or binaural hearing aids. The mean age was 45.2 years (SD, 18.3) ranged from 21 to 76 years. This study was approved by the Institutional Review Board of Samsung Medical Center (IRB No. SMC 2013-07-076), and each participant signed the written consent form after a full explanation for the study. All the experimental tests were administered at hearing research laboratory in tertiary hospital. The mean hearing thresholds at frequencies (0.5-8 kHz) for a test ear were plotted in Fig. 1. Pure tone average (PTA) across 0.5, 1, 2, and 4 kHz and WRS were 56.4 dB HL (SD, 7.0) and 72.6% (SD, 9.4%), respectively. Demographic information of the 26 hearing aid users is described in Table 1. Pure tone audiometry was conducted using a clinical audiometer (Orbiter922, GN Otometrics, Denmark) equipped with a headphone (TDH39, Telephonics, Farmingdale, NY, USA).
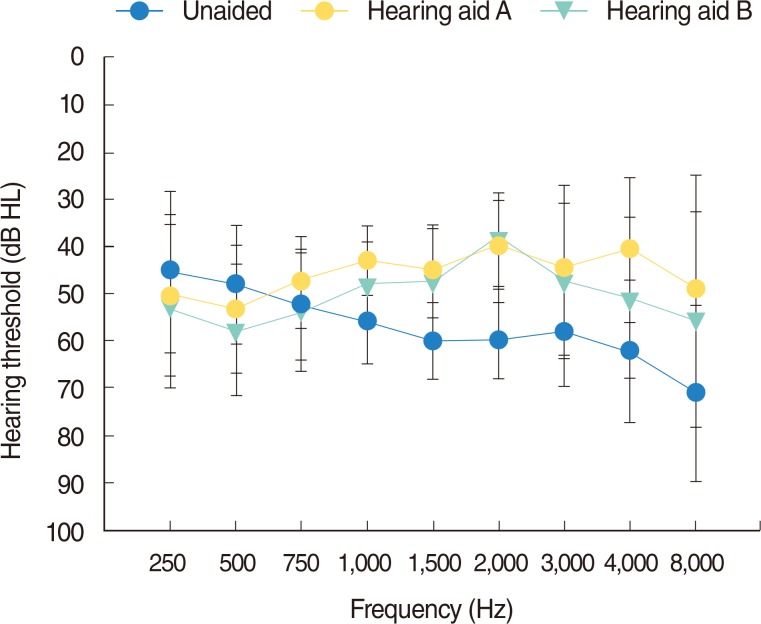 | Fig. 1Mean hearing thresholds for a test ear in unaided and aided condition, as a function of the given frequencies. The blue circles show unaided responses. The yellow circles and inverted green triangles describe A and B aided response. Error bars indicate ±1 SD about the mean across subjects. HL, hearing loss.
|
Table 1.
Demographic information of 26 hearing aid users
![]()
Procedures and equipment
Subjects were unilaterally fitted with two different manufacture's hearing aids (A and B) by an experienced audiologist. Both instruments were receiver in the canal (RIC) type with 16 channels, and earpieces of power dorm type were applied. As for a fitting formula, the National Acoustic Laboratories' nonlinear prescription, version two (NAL-NL2) [18] were adopted. All the functions of hearing aids were disabled other than feedback cancellation and microphone modes; OMNI or DIR mode. For estimation of amplification from each fitted hearing aid, aided warble tone thresholds were obtained and displayed in Fig. 1. Acclimatization period for the experimental hearing aids was not considered in this study.
In order to determine benefits from DIR microphone mode within a hearing aid (A) and compare performance of the DIR mode between hearing aids, subjective evaluation was performed via a questionnaire using a visual analogue scale (VAS) of zero to hundred. The target sentences in Korean standard sentence lists for adults [19] were presented at one meter distance from a front loudspeaker (0°) with 50 dB HL, while speech shaped noise was released at one meter distance from a rear loudspeaker (180°) with 40 dB HL. In the 10 dB SNR condition, Participants were asked to rate both the degree of speech quality (SQ) and discomfort in noise (DN), while comparing OMNI mode to DIR mode of hearing aid (A). DIR mode performance was also assessed between hearing aids. Each microphone mode and instrument was applied to the patients in a random order. In this questionnaire, higher scores mean better sound quality in SQ domain and strong DN in DN domain.
The participants also accomplished Korean HINT (K-HINT) [20], which was modified for this experiment to measure speech perception in only rear noise condition. The target sentences were presented from the front (0°) while speech shaped noise was released from the rear (180°). Presentation level of the noise was fixed at 65 dBA and the level of target sentences varied following adaptive procedure of original HINT [21]. Results of the modified K-HINT showed form of dB SNR; speech levels corresponding to 50% correct recognition of sentences in noise. The K-HINT was conducted three times including (1) OMNI mode, (2) OMNI mode plus noise reduction algorithm, and (3) DIR mode on each aided condition (hearing aid A and hearing aid B) in a random order. The test orders were counterbalanced across the participants.
This test battery was conducted on blocking the nontest ear's response by earplug. All hearing assessments and the subjective evaluation were conducted in a double-walled sound proof booth, and the K-HINT was measured in a semianechoic chamber.
Statistical analyses
All the statistical analyses were conducted using the PASW ver. 18.0 (SPSS Inc., Chicago, IL, USA), as follows: (1) paired t-test to compare difference in functional gains at given frequencies between hearing aids, (2) two-way analysis of variance (ANOVA) with repeated within-subject factors (instruments and DIR mode conditions) on K-HINT, including post hoc Bonferroni-adjusted multiple paired-comparison on DIR conditions and post hoc paired-sample t-tests in comparison of K-HINT results in each condition between hearing aids, (3) paired t-test to find effect of DIR mode either within or between hearing aids in each objective and subjective measurement, (4) independent samples t-test for group factor analysis (gender and bilateral hearing aid experience), and lastly (5) Pearson correlation coefficient analysis for factor analysis influencing DIR benefit.
Go to :
RESULTS
Functional gain
Functional gain means the gap between aided hearing threshold and unaided hearing threshold. Fig. 1 displays the aided hearing thresholds with each instrument. When wearing hearing aid A, functional gains at given frequencies (0.25, 0.5, 0.75, 1, 1.5, 2, 3, 4, 8 kHz) were -4.8, -5.3, 5.1, 12.5, 14.6, 20.0, 12.9, 21.5, and 21.7 dB HL while the functional gains were -6.9, -9.6, -0.8, 21.1, 12.1, 21.2, 10.4, 11.5, and 15.4 when wearing hearing aid B. There were significant gain differences (P<0.05) at all frequencies other than at 0.5 and 2 kHz.
Korean hearing in noise test
For hearing aid A, the K-HINT thresholds (dB SNR) in OMNI mode, OMNI mode plus noise reduction, and DIR mode were 5.4 (SD, 5.5), 5.0 (SD, 5.1), and 2.6 dB SNR (SD, 6.1) while the K-HINT results for hearing aid B were 3.9 (SD, 5.8), 3.9 (SD, 5.0), and 1.9 dB SNR (SD, 4.8), as described in Fig. 2. The amount of DIR benefit in both hearing aids was not statistically different. Two-way ANOVA with repeated measures was performed on K-HINT results with within-subject factors; (1) instrument and (2) DIR mode condition. Results showed that K-HINT performances were significantly affected by instrument [F(1, 25)=5.68, P<0.05] and DIR mode condition [F(1.59, 39.86)=21.30, P<0.01], but it appeared no interaction between the two factors. Results from Bonferroni-adjusted multiple paired-comparisons revealed that K-HINT performance was significantly improved (P<0.01) when switching OMNI mode to DIR mode even though the results were similar in both OMNI mode and OMNI mode plus noise reduction condition. The post hoc paired-sample t-tests indicated that hearing aid B brought significantly better SNRs (in OMNI mode) than hearing aid A on average, but it showed nonsignificant difference in DIR mode.
 | Fig. 2Signal to noise ratio (dB SNR) of Korean hearing-in-noise test as a function of each test condition measured in hearing aid A and hearing aid B. The conditions were classified under 4 heads; omnidirectional (OMNI) mode, OMNI mode plus noise reduction (NR), directional (DIR) mode, and benefit from switching OMNI mode to DIR mode. Error bars indicate ±1 SD about the mean across subjects.
|
The amount of SNR benefit from DIR mode was calculated by subtracting SNR in the Omni mode from the SNR in the DIR mode. The benefit of hearing aid A and B by using DIR mode were 2.78 (SD, 3.46) and 2.06 (SD, 2.52), which were statistically significant. Paired-sample t-tests showed no difference between SNRs in both hearing aids. In addition, as a subanalysis, such independent variables as gender and bilateral hearing aid experience did not brought any difference in the SNR benefit.
Subjective evaluation of DIR mode
The higher scores of subjective evaluation mean better SQ and strong DN. The SQ scores of each OMNI and DIR mode of hearing aid A were 76.89 (SD, 12.00) and 81.54 (SD, 11.70) and the DN scores were 48.27 (SD, 21.17) and 31.84 (SD, 21.06), which indicated that the DIR mode showed a significant benefit in both SQ (P<0.05) and DN (P<0.01). Additionally, 18 (69.2%) and 22 (84.6%) of total 26 listeners prefer DIR mode to OMNI mode on SQ and DN domain while using hearing aid A and B, respectively. In comparison of hearing aid A and B with a DIR mode, the SQ scores of each hearing aid A and B were 77.67 (SD, 17.76) and 79.27 (SD, 14.40), and their DN scores were 34.88 (SD, 19.42) and 34.92 (SD, 19.89), which resulted in nonsignificant differences in SQ and DN (P<0.05). These results were also reflected in similar preference of instrument where 12 subjects (46.2%) and 13 subjects (50.0%) preferred hearing aid A on SQ and DN whereas 11 subjects (42.3%) in both case preferred hearing aid B. Other remaining subjects rated the same scores on hearing aid A and B. Each mean score was plotted in Fig. 3. As a subanalysis, gender and bilateral hearing aid experience did not make any difference in the scores on SQ and DN.
 | Fig. 3Mean scores on speech quality and discomfort in noise in condition (A) and (B). The higher scores mean better speech quality and strong discomfort in noise. In condition (A) comparing an omnidirectional (OMNI) mode with a fixed directional (DIR) mode within hearing aid (HA) A, the blue bar indicates the mean scores using OMNI mode whereas the yellow bar appears the mean scores using the DIR mode. In condition (B) which makes a comparison of DIR mode between HA A and B, the score of HA A is expressed in the blue bar while that of HA B is showed as the yellow bar. Error bars indicate±1SD.
|
Factor analysis influencing DIR benefit
As shown in Table 2, all of factors including age, duration of hearing aid usage, PTA, SRT, and WRS did not significantly affect DIR benefits in the subjective evaluation for hearing aid A and K-HINT for both instruments. In addition, there was no significant association between the subjective DIR benefit by the questionnaire and the objective DIR benefit in K-HINT.
Table 2.
Pearson correlation coefficients, r-values between variables
PTA, pure tone average; SRT, speech reception threshold; WRS, word recognition score; SQ, speech quality; DN, discomfort in noise; OMNI, omni-directional; DIR, fixed directional; K-HINT, Korean hearing-in-noise test; HA, hearing aid; A-SQ, speech quality for HA A; A-DN, discomfort in noise for HA A.
![]()
Go to :
DISCUSSION
Hearing aids implemented with DIR microphones and noise reduction algorithms have become quite popular in recent years. Previous studies leaves little doubt that average hearing aid users show better performance when using hearing aids in DIR mode than OMNI mode in at least some listening conditions [2]. DIR advantage occurs because the DIR mode provides more output for sounds arriving from directly in front of the listener and less average output for sounds arriving from other directions. If the signal of interest is in front of the listener and noise surrounds the listener, then an improvement in SNR can be clearly obtained by using the DIR mode. In spite of generally positive findings from the previous studies, the DIR benefit varies greatly across the studies. Regarding word recognition, the DIR benefit ranged from approximately 0% to more than 70% [22].
In this study, both hearing aids showed similar results that there was no difference between OMNI mode and OMNI mode plus noise reduction algorithm, which is in line with previous results indicating no effect of noise reduction processing on speech intelligibility in noise [4232425]. Although, the noise reduction algorithm has been developed to improve physical SNR, it appears that the feature embedded in a hearing aid provides listening comfort rather than remarkable advantages in laboratory speech perception in noise test [1326]. In contrast to noise reduction features, DIR mode in both hearing aids significantly improved speech recognition performance in background noise (improvement of dB SNR in K-HINT) as compared to the OMNI mode, which is also consistent with previous studies. The mean benefits (about 2.45 dB SNR) from DIR processing of both hearing aids in this study were comparable to the results (3-5 dB SNR) of prior researches. Nevertheless, smaller value obtained in this study can be explained by the different study design. In this study, laboratory testing was performed with unilateral hearing aid fitting, and bilateral DIR benefit was not considered accordingly [27]. For hearing aid B with OMNI mode, the superiority in K-HINT results over that of hearing aid A with OMNI mode could be attributed to comfortable listening in noise due to lower gain at most frequencies than the gain of hearing aid A, as plotted in Fig. 1. However, it is hard in this study to reveal which hearing aid has an advanced DIR processing because the DIR benefit between the two hearing aids were not statistically different.
Besides evaluating objective benefit, subjective benefit can be assessed using structured questionnaires. In a previous study, Gnewikow et al. [11] used two conventional questionnaires; profile of hearing aid benefit and amplification in daily life after using each microphone processing scheme for one month in a real environment, but did not reveal the DIR benefit in real-world. No actual DIR benefit from various noise configurations in real environment could be reflected in the questionnaire results [1128]. In similar way, the simple questionnaire with VAS as a subjective and quantitative measurement was implemented in this laboratory study. In contrast to other studies, however, it showed significant improvement for DIR processing in both SQ and DN even though Chung [26] suggested disadvantage of DIR processing was higher internal circuit noise that could deteriorate sound quality. The reason for difference in results between current and previous study is thought to be attributed to different questionnaire form based on experimental condition and real-ear condition. While previous studies respectively implemented the questionnaire survey in order after using each microphone mode for some time, current study allowed subjects to compare them in real time and rate scores for each condition This quantitative questionnaire form without multiple choices led very higher preference (SQ, 69.2%; DN, 84.65%) of DIR mode over OMNI mode at 10 dB SNR condition at which some studies [710] reported about 40% of preference. Moreover, there were no significant differences in SQ and DN between hearing aid A and B with a DIR mode, which seemed to be concomitant with nonsignificant difference in the K-HINT. However, numerical scores of DIR benefit in SQ and DN seemed not to predict the amount of DIR benefit in K-HINT as there was no significant correlation between the results of each subjective and objective measurement.
All measured within-variables such as age, duration of hearing aid usage, PTA, SRT, and WRS were not correlated to DIR benefits in the subjective and objective evaluation. Furthermore, group-variables such as gender and bilateral hearing aid experience did not make any difference in DIR benefit in the both measurement. The reason for this negative results is likely to be either no consideration of acclimation period to the experimental hearing aid (RIC type) [29] in this study design. All participants other than three subjects usually used completely in the canal type. Nonetheless, since Dawes et al. [30] found no evidence for the effect of hearing aid acclimatization, impact of the acclimatization can be equivocal. Thus, as a result, our factor analysis results also supports findings in previous studies that factors influencing individual variation in perceptual DIR benefit were hard to explain.
In summary, unlike prior studies, DIR benefit was found not only in the objective measurement but also in the subjective measurement in this laboratory setting, but the subjective results was failed to have significant correlation with the DIR benefit obtained in K-HINT. Furthermore, any individual factors were not found to account for DIR benefit in both objective and subjective evaluation.
Go to :
 XML Download
XML Download