

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
The prevalence of obesity worldwide has more than doubled since the 1980s. In 2005, it was estimated that 1.06 billion people aged ≥15 years were overweight and that about 40 million people were obese. It has been projected that, by 2015, 2-3 billion people will be overweight and over 70 million will be obese [1].
Obesity has been found to correlate with cardiovascular disease (CVD), cancer, diabetes, kidney disease, and other conditions, as well as with a higher mortality rate [2]. Several studies have shown associations between obesity and otolaryngologic diseases. For example, a study performed to verify the relationship between otitis media with effusion (OME) in children and obesity found out that the mean body mass index (BMI) was higher in pediatric patients with than without OME [3].
Obesity is characterized by low-grade systemic inflammation, with higher expression of inflammatory markers such as C-reactive protein (CRP) and interleukin (IL) 6 in obese than in underweight individuals. Systemic inflammation in obesity has been found to be associated with the increased incidence of CVD and type 2 diabetes mellitus (DM), especially in abdominally obese people [4]. Despite many investigations on inflammatory diseases and obesity, no studies to date have assessed the association between obesity and leading inflammatory diseases in otorhinolaryngology, including chronic otitis media (COM), chronic rhinosinusitis, and chronic tonsillitis. This study was therefore designed to identify the relationship between obesity and these representative otorhinolaryngologic diseases.
MATERIALS AND METHODS
This study involved patients, aged ≥20 years, who underwent surgery for COM (n=128), chronic rhinosinusitis (n=184), or chronic tonsillitis (n=162) in the Department of Otorhinolaryngology of Kyung Hee University Medical Center from 2010 to 2012. Surgery was implemented after confirming inflammatory lesions on temporal bone computed tomography (CT) in patients with COM and paranasal sinus CT in patients with rhinosinusitis and after confirming recurrent tonsillitis in patients with chronic tonsillitis. Surgical treatment included tympanoplasty and mastoidectomy in patients with COM, endoscopic sinus surgery in patients with chronic rhinosinusitis, and tonsillectomy in patients with chronic tonsillitis. The control group consisted of 111 patients aged ≥20 years, with no history of otitis media, rhinosinusitis, or tonsillitis; these patients had dizziness, tinnitus, voice change, abnormalities in both smell and taste sensitivity, or other symptoms during physical examination. Subjects suspected of having systemic diseases, head and neck anomalies, allergic rhinitis, nasal polyps, cholesteatoma, malignancies, or congenital or acquired immunodeficiencies were excluded.
BMI (calculated as weight in kilograms divided by height in meters squared) is the most commonly used criterion for the assessment of obesity. Based on the standards of the World Health Organization (WHO) for the Asia-Pacific region (WHO, Asia-Pacific Perspective, 2000), underweight was defined as a BMI≤18.5 kg/m2, normal as a BMI>18.5 kg/m2 but ≤22.9 kg/m2, overweight as a BMI>23.0 kg/m2 but ≤24.9 kg/m2, and obese as a BMI>25.0 kg/m2 [5]. Mean BMIs and the percentages of overweight and obese patients in each of the experimental groups were compared with the control group. Correlations between BMI and disease duration were assessed in the COM, rhinosinusitis, and tonsillitis groups.
All statistical analyses were performed using PASW Statistics ver. 18.0 (SPSS Inc., Chicago, IL, USA). The Mann-Whitney test, Fisher exact test, chi-square test, correlation analysis, and other statistical analyses were performed, as indicated. Differences were considered statistically significant at P<0.05.
RESULTS
Mean age and sex ratio were similar in the groups of patients with COM, chronic rhinosinusitis, and chronic tonsillitis and in the control group with no history of otolaryngologic inflammatory diseases. The percentages of patients with a history of hypertension and a history of diabetes also did not differ among these four groups (P>0.05) (Table 1).
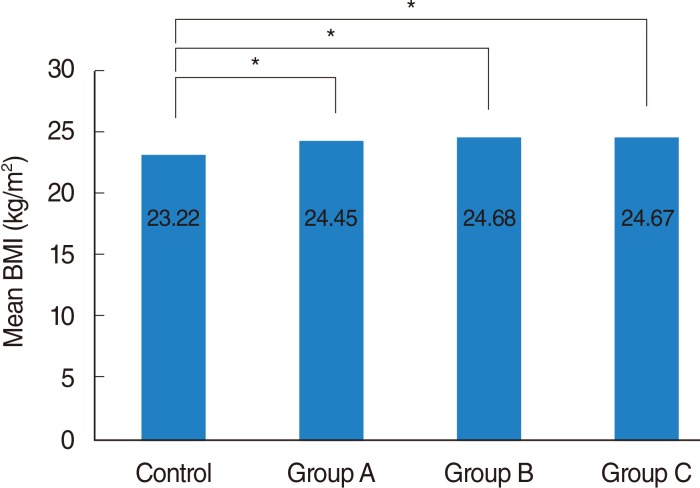
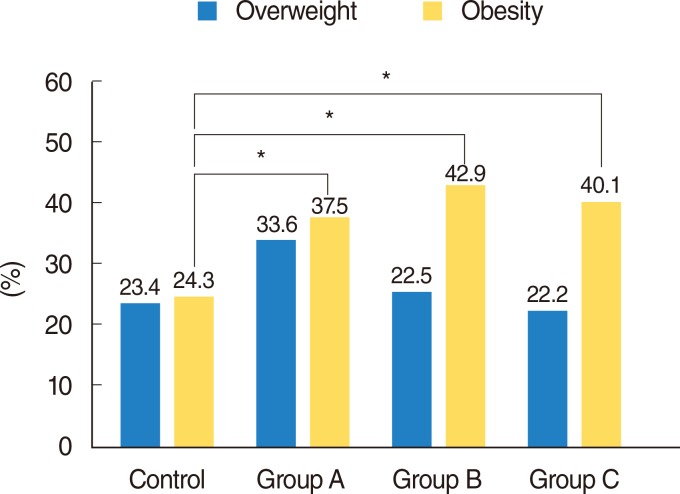
Mean BMI was significantly higher in patients with COM (24.45±2.72 kg/m2), chronic rhinosinusitis (24.68±3.25 kg/m2), and chronic tonsillitis (24.67±3.82 kg/m2) compared with the control group (23.22±3.01 kg/m2, P<0.05 each) (Fig. 1). Relative to the control group, in which 24.3% of patients were obese, the percentages of obese patients were significantly higher in the COM (37.5%, P=0.036), chronic rhinosinusitis (42.9%, P=0.002) and chronic tonsillitis (40.1%, P=0.009) groups (Fig. 2), but the percentages of overweight patients did not differ significantly in each group relative to the control group (Fig. 2).
Average duration of disease was 6.10±5.52 years in the COM group, 6.57±8.28 years in the chronic rhinosinusitis group, and 7.15±7.66 years in the chronic tonsillitis group. When the correlation between disease duration and BMI was analyzed in each group, a significant association was observed in patients with chronic tonsillitis (correlation coefficient=0.231, P<0.05), but not in the other two groups (Table 2).
DISCUSSION
The prevalence of obesity, a risk factor for various diseases, has increased worldwide. Chronic low grade inflammation may interact with obesity and metabolic complications, and obesity and inflammation have been associated with type 2 DM, CVD, hypertension, stroke, gallbladder disease, some cancers, osteoarthritis, psychosocial problems, and others [6]. The concentrations of inflammatory markers, including CRP and IL-6, are higher in overweight than in underweight individuals, and systemic inflammation has been associated with the incidence of CVD and type 2 DM, especially in individuals with abdominal obesity [4]. Recent studies on obesity have focused on adipose tissues as active secretory organs that exchange signals with other organs [7]. The adipokines leptin and adiponectin are proteins released by adipocytes in adipose tissue. Other cytokines secreted by adipose tissue include IL-6, tumor necrosis factor (TNF)-α, white adipose tissue-derived IL-1 receptor antagonist, IL-18, IL-8, monocyte chemoattractant protein-1, and macrophage inflammatory protein-1 [89]. The concentrations of IL-6 and TNF-α are higher in the serum and adipose tissue of subjects with than without obesity [10].
The increase in inflammation-related substances in obese individuals has suggested an association between chronic inflammatory diseases and obesity. The primary chronic inflammatory diseases in otolaryngology are COM, chronic rhinosinusitis, and chronic tonsillitis. To date, however, no studies had examined the relationship between these diseases and obesity in adults. This study was therefore designed to analyze the association between obesity and the leading chronic inflammatory diseases in otolaryngology.
A previous study found that mean BMI was significantly higher in children with (22.0±3.4 kg/m2) than without (16.3±2.4 kg/m2) OME, indicating an association between obesity and pediatric OME [3]. Although the exact cause of this association has not yet been clarified, changes in obesity-related cytokine concentration, accumulation of adipose tissue around E-tubes, and changes in the sense of taste in patients with OME may be responsible [11].
Another otolaryngologic disease, obstructive sleep apnea syndrome (OSAS), has been associated with obesity, along with other risk factors, such as male sex, age, and genetic factors [12]. OSAS in obese individuals is thought to be caused by the increased collapsibility of pharyngeal structures during air movements, changes in chest wall dynamics, and respiratory muscle compliance and function [13].
According to the relationship between asthma and obesity [14], the severity of asthma, as measured by daily symptoms, missed workdays and the use of rescue bronchodilators, is higher in obese than in nonobese patients [15]. Along with mechanical causes of asthma, an increase in BMI may increase the occurrence of associated conditions, including gastroesophageal reflux disorder, sleep-disordered breathing, type II DM, and hypertension. In addition, the incidence of asthma could be influenced by airway inflammation, which occurs in patients with low grade proinflammation, such as that occurring during obesity [16]. However, the effect of obesity-related systemic inflammation on the incidence of asthma remains unclear.
COM is characterized by irreversible inflammatory changes within the mastoid of the middle ear, although the exact cause of the progression from acute to chronic infection has not yet been determined. A study of children with OME found that mean BMI was higher in subjects with than without OME. The risk of COM is higher in pediatric patients with a history of OME. We found that mean BMI and the percentage of obese individuals were significantly higher in the COM than in the control group, similar to findings in pediatric patients with OME. Among the cytokines expressed in patients with COM are TNF-α, fibroblast growth factors, and bone morphologeneitc proteins, which act on tissue remodeling, as well as IL-1α, IL-1β, IL-2, and IL-6, which are associated with inflammatory cell proliferation in otitis media [17]. Obesity-associated alterations in cytokine expression may affect the expression of cytokines associated with otitis media.
The two hypotheses thought to explain the pathogenesis of chronic rhinosinusitis are the staphylococcal superantigen hypothesis and the immune barrier hypothesis. The latter, in particular, may explain various defects observed in mechanical (epithelial) and immunologic (innate and adaptive) barriers [18]. Signal transducer and activator of transcription 3, a transcriptional mediator of the IL-6 family of cytokines, plays a crucial role in host defenses. Defects in this process in chronic rhinosinusitis may result in excess inflammatory responses [19], possibly due to changes in expression of obesity-related cytokines. Inflammation occurring during upper respiratory infections may be similar to that observed in relapsed chronic tonsillitis, with the latter associated with changes in obesity-associated cytokine expression.
In conclusion, mean BMIs and the percentages of obese patients were significantly higher in groups of patients with common otorhinolaryngologic inflammatory diseases, including COM, chronic rhinosinusitis, and chronic tonsillitis, than in control patients. Further research is needed to assess the relationships between obesity and other chronic Ear-Nose-Throat diseases, as well as the mechanisms relating obesity with these diseases.
 XML Download
XML Download