

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
A canal wall down (CWD) tympanomastoidectomy is thought to be an effective procedure in treatment of chronic middle ear disease, however, it has disadvantages regarding cavity problems such as continuous ear drainage (range, 20% to 60%) [1], accumulation of keratin debris, frequent vertigo attacks following temperature or pressure change, and difficulty in fitting a hearing aid. In addition, the final hearing gained after staged ossiculoplasies in patients who have undergone CWD is usually 5-10 dB worse than the patients who have undergone canal wall up (CWU) tympanomastoidectomy due to its ineffective sound transmission [2,3].
Various techniques of mastoid obliteration or canal wall reconstruction have been reported to overcome cavity problems. Several kinds of muscular flap [4,5], fat [6], cortical bone pate [7], hydroxylappatite [8], β-tricalcium phosphate and polyphosphate [9], demineralized bone matrix [10,11] and silicone blocks [12] are used. However, all of these techniques have its advantages and disadvantages. Bone pate is restricted by its insufficient amount in material and it is vulnerability to infection [13,14]. Fat and muscular flaps have unpredictable absorption rate over the time [6]. Synthetic materials are limited by the need for vascularized flap coverage, infection, incomplete osteointergration, and late extrusion [15]. Black [13] reported that autologous cartilage is excellent material for canal reconstruction and mastoid obliteration. However, he reported that inadequate amount for filler work from the ear locality and complication risk from the costal supplies limited its appeal as filler [13].
Autologous costal cartilage has been widely used in otolaryngologic surgery. It is an excellent source of grafting material for the rhinoplasty [16], auricular reconstruction [17], and laryngotracheal reconstructions [18]. However, as Black [13] mentioned, conventional costal cartilage harvest techniques which were commonly used in those procedures can cause complications such as pneumothorax, chest wall deformity, seroma formation, persistent pain, infection, and keloid formation [16,19]. In addition, donor-site morbidities after costal cartilage harvest make it an invasive procedure and limit its usage.
To use the costal cartilage as a mastoid obliteration material, surgeons should overcome the morbidity of costal cartilage harvest procedure. So, we present a minimally invasive costal cartilage harvest technique to address the complications associated with costal cartilage harvest. A minimally invasive costal cartilage harvest procedure preserves the all perichondria and harvest only required amount for mastoid obliteration. In addition, there is remnant cartilage which can gives the structural stability to costal cartilage.
The purpose of this study is to evaluate the donor site morbidity of newly developed costal cartilage harvest technique and to see whether the morbidity of this technique can be accepted by surgeon and the patient or not. It is an important first step whether costal cartilage can be used, as an alternative material for mastoid obliteration and reconstruction of posterior ear canal wall or not.
Go to : 
MATERIALS AND METHODS
Patients
A retrospective review of patient records was performed for a consecutive series of 151 patients who underwent CWD mastoidectomy and mastoid obliteration using costal cartilage in the treatment of chronic otitis media. The study was approved by the Institutional Review Board at Chonnam National University Hospital (No. CNUH-2013-120).
Surgical technique for costal cartilage harvest and mastoid obliteration
Autologous costal cartilage harvest procedure and tympanomastoidectomy were carried out simultaneously. Right costal cartilages were preferred to differentiate postoperative pains from potential angina symptoms. A 1.5- to 4-cm-sized incision was made over the seventh costal cartilage just inferior to the inframammary crease (Fig. 1A). Subcutaneous and fascial layers were dissected down to the level of external oblique muscles. The muscle fibers were bluntly divided to identify the costal cartilage. The overlying perichondrium was incised longitudinally along the midline of costal cartilage axis. Using a newly devised cartilage gouge (Fig. 1B), a portion of upper central costal cartilage was harvested. Cartilage and perichondrium of lateral and inferior locations was left intact. The competency of pleura was evaluated by the absence of air bubbles from a pool of normal saline in the donor site. Upon hemostasis, the donor site was closed by layers, including the perichondrial layer (Fig. 1C). The harvested cartilage was ground with a bone mill (Quentin Bone mill, Quentin Dental products, Leimen, Germany) (Fig. 1D) and were set aside in physiologic saline solution. After CWD mastoidectomy (Fig. 1E), the disease-free mastoidectomized cavity was obliterated with the prepared autologous costal cartilage (Fig. 1F) and fibrin-based adhesive (Greenplast, Green Cross, Seoul, Korea). The retroauricular wound was closed in the standard fashion.
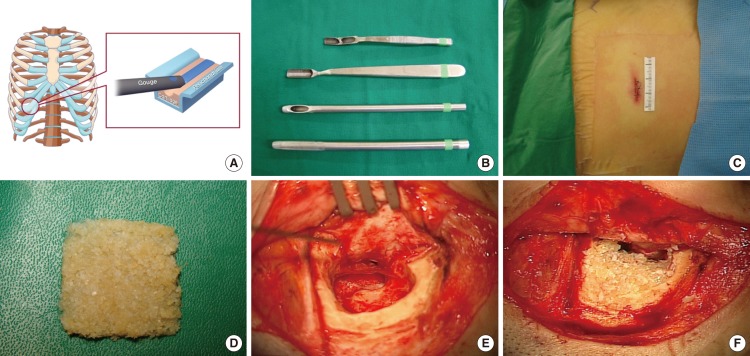 | Fig. 1Mastoid obliteration with chopped costal cartilage. (A) Costal cartilage was harvested from the 7th rib. Note that perichondrial layers of lower and inferior portions are preserved. (B) Newly devised instruments for costal cartilage harvest. (C) Immediate postoperative photograph of costal cartilage harvest site demonstrates a 1.5-cm incision upon closure. (D) Costal cartilage is prepared by a bone mill. (E) A mastoidectomized cavity before mastoid obliteration. (F) An intraoperative photograph shows a mastoidectomized cavity obliterated with chopped costal cartilage.
|
Donor site morbidity evaluation
The overall perception and attitude to the costal cartilage harvest technique was evaluated first. Additionally, donor site morbidity was checked in the framework of postoperative pain, patient-centric cosmetic concern, scar evaluation, and of other complications. The retroauricular skin incision sites were compared with costal cartilage harvest incision sites.
Pain
Postoperative pain was assessed by a questionnaire, which included a 10-cm visual analogue scale (VAS Pain) (Table 1). A score of 10 indicated the worst pain conceivable, and a score 0 indicated no pain. Out of the 151 patients, 52 male and 83 female patients (n=135) with ages ranging from 22 to 80 years answered the questionnaire. Patients evaluated pain on postoperative days 1, 2, 3, 7, 30, 60, and 180. In addition to VAS Pain score, the duration of physical suffering were also asked in the questionnaire.
Table 1.
Pain and scar assessment scales and scores used in the study
| Scale | Score range | Description | Chest score* | Ear score† | P-value |
|---|---|---|---|---|---|
| Visual analogue scale | |||||
| Pain | 0–10 | 0, no pain; 10, worst pain | 0.80±1.25 | 1.48±1.86 | <0.001 |
| Cosmetic | 0–10 | 0, best; 10, worst | 0.62±1.22 | 0.68±1.28 | 0.421 |
| Patient and observer scar assessment scale | |||||
| POSAS | 11–110 | 11 to 110, ‘excellent’ to ‘poor’ | 23.17±12.47 | 19.43±6.81 | 0.055 |
| PSAS | 6–60 | 11.07±8.07 | 8.23±4.20 | 0.017 | |
| Pain | 1–10 | 1, no complaints; 10, worst imaginable | 1.23±0.57 | 1.20±0.55 | 0.655 |
| Itching | 1–10 | 1, no complaints; 10, worst imaginable | 1.37±0.76 | 1.40±0.72 | 0.794 |
| Color | 1–10 | 1, as normal skin; 10, very different | 2.77±2.47 | 1.50±1.16 | 0.003 |
| Stiffness | 1–10 | 1, as normal skin; 10, very different | 1.90±2.06 | 1.53±1.19 | 0.233 |
| Thickness | 1–10 | 1, as normal skin; 10, very different | 2.20±2.46 | 1.33±0.84 | 0.028 |
| Irregular | 1–10 | 1, as normal skin; 10, very different | 1.60±1.19 | 1.26±0.64 | 0.175 |
| OSAS | 5–50 | 12.10±4.80 | 11.20±3.27 | 0.273 | |
| Vascularization | 1–10 | 1, normal skin; 10, worst scar imaginable | 3.23±1.07 | 3.40±1.00 | 0.349 |
| Pigmentation | 1–10 | 1, normal skin; 10, worst scar imaginable | 2.83±0.60 | 2.90±1.03 | 0.819 |
| Thickness | 1–10 | 2.36±1.96 | 1.90±1.34 | 0.306 | |
| Relief | 1–10 | 1.77±1.50 | 1.43±0.86 | 0.168 | |
| Pliability | 1–10 | 1.90±1.21 | 1.57±0.90 | 0.210 | |
| Mexameter | |||||
| Erythema | 0–999 | A higher value representing more melanin or erythema | 421±99.2 | 437±99.9 | 0.150 |
| Pigmentation | 0–999 | A higher value representing more melanin or erythema | 178±54.0 | 185±92.8 | 0.860 |
![]()
Scar
Similarly to the pain assessment, cosmetic concerns were assessed on 10-cm VAS within the same questionnaire (VAS cosmetic). A score of 10 indicated the poorest cosmetic outcome conceivable, and a score 0 indicated no cosmetic problem. VAS Cosmetic score of costal cartilage harvest sites were compared to that of the retroauricular skin incision site.
Additionally, the incisional scars were assessed according to the modified Vancouver Scar Scale (VSS) [20] and the Patient and Observer Scar Assessment Scale (POSAS) [21]. The VSS encapsulated multiple factors, including pain, clicking sound, scar length, depth, and scar consistency and provided a numerical reflection of donor-site quality (Table 2). A score of 10 indicated an excellent donor site, and a score of 0 indicated the worst possible scar.
Table 2.
The variables and scores of Modified Vancouver Scar Scale in the study population at the postoperative 6 months
![]()
The POSAS were evaluated for 30 patients at 6 months post operation. It consists of two numeric scales: the Patients Scar Assessment Scale (patients scale, PSAS) which is to be completed by the patient, and the Observer Scar Assessment Scale (observer scale, OSAS) which is to be completed by the physician (Table 1) [21]. A score of 11 indicated a normal skin, and score 110 indicated the worst scar imaginable. The POSAS scores were compared between the costal cartilage harvest site and the retroauricular skin incision site.
In addition to VAS and POSAS assessments, a skin color meter (Mexameter MX18, CK electronic, Cologne, Germany) was used for objective scar evaluation. Erythema and pigmentation levels were assessed for 30 patients 6 months post operation (Table 1).
Donor site complication
Surgical complications of costal cartilage harvest were evaluated during the follow-up period in terms of contour deformity, pneumothorax, seroma formation, keloid formation and surgical site infection.
Statistical analysis
Statistical analyses were performed using PASW ver. 18.0 (SPSS Inc., Chicago, IL, USA). Continuous variables were presented as mean±SD. The paired t-test was used to compare normally distributed data, and the Wilcoxon signed-rank test was used otherwise. Two-sided P-values of less than 0.05 indicated statistical significance.
Go to :
RESULTS
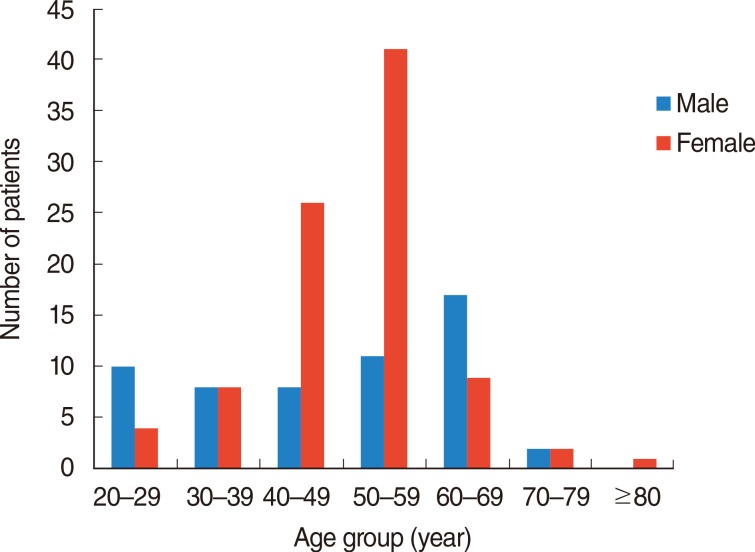
Of the 155 patients, 135 completed the questionnaire for pain and cosmetic concern (53 males and 83 females). The mean age was 48.6±13.7 years (range, 22 to 80 years) (Fig. 2). Additionally, the number of patients who had been assessed with VSS, POSAS, and Mexameter was 51, 30 and 30, respectively.
Overall perceptions and attitudes to the procedure
One hundred and ten patients (85.3%) responded that costal cartilage harvest procedure was an acceptable method, while 19 patients (14.7%) considered the procedure as uncomfortable. One hundred and nine out of 133 patients (82.0%) answered to reuse the costal cartilage if they have to redo the ear surgery. One hundred and twenty-four out of 133 patients (93.2%) answer to donate their cartilage to the child for homologous graft, if their child need CWD and mastoid obliteration.
Pain
None of the patients in this study required patient-controlled analgesia (PCA) for postoperative pain management. VAS pain score for the costal cartilage harvest site was 3.0±2.5 on postoperative day 1 and dropped gradually during the follow-up period. At 6 months post operation, the mean VAS pain score for costal cartilage harvest site was 0.9±1.3 (Fig. 3). The pain at the costal cartilage harvest site using the minimally-invasive technique was significantly less than that at the retroauricular skin incision site at 6 months (Table 1). The mean duration of noticeable postoperative pain was 5.3±9.46 days. At 1 month post operation, only three out of the 133 patients experienced physical suffering. At 2 months, none of the patient reported physical suffering.
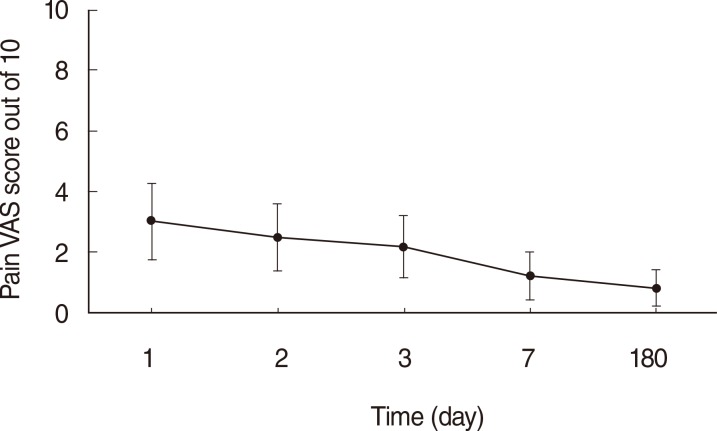 | Fig. 3Visual analogue scale (VAS) pain score of the study patients. The VAS pain score gradually decreased to 0.9 by 180 days after operation. A score of 10 indicates the worst pain imaginable, and a score of 0 indicates no pain. Solid line indicates mean VAS pain score. Error bar indicates standard deviation.
|
Scar
The length of incision was from 1.5 to 4 cm, and the mean scar length was 2.5 cm. This incision provided accesses adequate enough for 3 to 5 cm3 of costal cartilage harvest volume. The volume of costal cartilage needed to obliterate the mastoidectomized cavity ranged from 1.2 to 4 cm3.
On the questionnaire regarding cosmetic concern at 6 months post operation, the mean VAS cosmetic scores were 0.6 and 0.7 for costal cartilage harvest site and retroauricular skin incision site, respectively. There were no statistically significant differences between these two sites (Table 1). Of the 100 patients who responded to this portion of the questionnaire, VAS cosmetic score greater than 3 for five patients, all of whom were female patients.
The VSS score on postoperative day 1 was 8.3±1.2, and this gradually increased to 9.5±1.0 by 6 months post operation. All of the patients gave highest score for four out of the total 7 variables (depth, contour change, tenderness, clicking) (Table 2). Out of the 51 patients, 39 patients had scored 10 of 10, which represented the best result imaginable. There was no patient who scored 5 or less on this scale.
The mean POSAS score was 23.17±12.47. The mean OSAS score was 12.10±4.80, with a mean PSAS score of 11.07±8.07 at 6 months post operation. The POSAS (P=0.063) and OSAS (P=0.230) values were not significantly different between the two sites. However, the PSAS scores were significantly different between the two incision sites (P=0.035) (Table 1).
The mean erythema values, as measured by mexameter, were 422 and 437 for costal cartilage harvest site and retroauricular skin incision site, respectively (P=0.401). The mean pigmentation were 179 and 186 for costal cartilage harvest site and retroauricular skin incision site, respectively (P=0.683). The erythema and pigmentation levels were not significantly different between the donor and recipient sites (Table 1).
Donor site complication
Out of 151 patients, three patients experienced wound dehiscence, which was managed with wound dressing. None of the patients reported clicking sound or contour deformity on their chest. There was no case of hematoma. One patient did develop keloid formation. Otherwise, there were no major complications, such as pneumothorax, atelectasis, chest wall deformity, or massive bleeding.
Go to :
DISCUSSION
Overall perceptions and attitudes to the procedure
To see the overall perceptions and attitudes to the procedure, we had asked 3 simple questions. "What is your overall perception to costal cartilage harvest procedure? Is this relatively comfort as a procedure?" "If you have to redo the ear surgery, are you willing to use the rib cartilage for mastoid obliteration again?" "If your child needs CWD and mastoid obliteration surgery are you willing to donate your rib cartilage for homologous graft?" Majorities of the patients satisfied with these procedures. However this study was done to Korean with chronic otitis media. Korean tends to sufficiently dressed than the Westerner due to their cultural characteristic, and most of the patients' ages tend to be above the marriageable age. The patients seemed to have relatively less cosmetic burden to the chest scar.
Pain
Pain is the most common complication after a costal cartilage harvest procedure [22,23]. The VAS is a simple and often used method for evaluating variations in pain intensity. It is superior to fixed interval scales, relative pain scales, and verbal reports of pain, and its usefulness in pain evaluation has been validated by several studies [24,25,26].
Postoperative pain has been reported to peak at 7 days after the conventional costal cartilage harvest technique [19]. In this study, most patients reported that postoperative pain slightly affected their daily activity in the first two postoperative days, while none of the patients required PCA. Postoperative pain was most severe on day 1, at 2.9 out of the 10 VAS scale, and decreased rapidly after day 2 (Fig. 3). On postoperative day 7, most patients reported no significant pain which interfered with daily activities. This may be due to the preservation of perichodrial layer and the use of minimally-invasive technique.
In the study of postoperative pain after conventional harvest method, notwithstanding the use of bupivacaine infusion, the mean VAS pain score was 3 in the immediate postoperative period, which increased to 7 by day 7. Out of 39 patients in the study, six experienced persistent pain at the 3-month point [19].
The present study, the mean duration of noticeable pain was 5.3 days, after which patients usually regarded the pain as minor or nonexistence. At the time 2 months post operation, no patients had reported noticeable pain. Compared to the pain studied after the conventional method [19], our technique causes less postoperative pain with shorter pain duration.
Scar
The mean incision length from this study was one-third that of conventional costal cartilage harvest method [19]. Contour deformity or depth changes were uncommon, considering the smaller incisions, minimal invasive maneuvers, and preservation of perichondrial layer. The mean VAS Cosmetic score was 0.6 for the costal incision site, which was less than that for the retroauricular skin incision site.
Adding to the VAS cosmetic score, the VSS and POSAS scales were used for scar assessment. Several versions of VSS exist and this study adopted the version which was modified by Uppal et al. [19]. The VSS encapsulates multiple factors, including length, depth, and consistency of the scar, to numerically reflect the quality of incisional scar at the donor site (Table 1). In this study, the VSS score was 8.3±1.2 on postoperative day 1 and gradually increased to 9.5±1.0 by 24 weeks post operation. As a score of 10 indicates an excellent donor site while a score of 0 indicates the worst possible, the 24-week score represented extremely satisfactory donor site outcomes (Fig. 4). Although a direct comparison is not possible, the VSS scores were reported to be 2 and 8.5 on days 1 and 90 post operation in the study on conventional costal cartilage harvest technique [19]. These findings suggest that the minimally-invasive technique presented has resulted in more acceptable scars than that after the conventional harvest procedure.
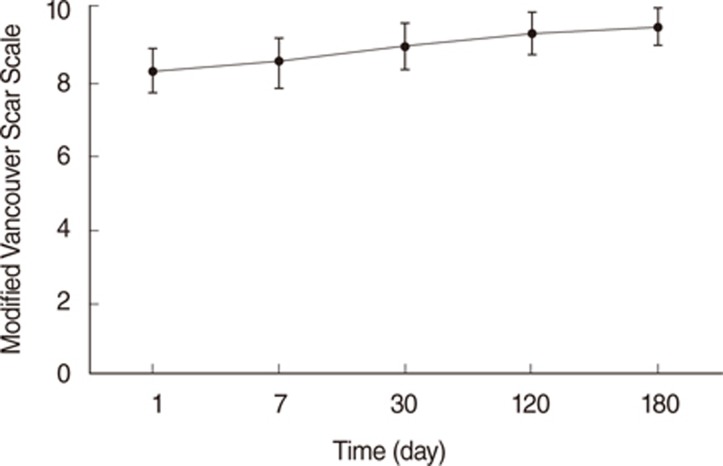 | Fig. 4Modified Vancouver Scar Scale (VSS) score of the study patients. A VSS score of 10 indicates an excellent donor site, and a score of 0 indicates the worst donor site possible. The VSS score improved over the follow-up period and is relatively close to the highest (optimal) score by 180 days post operation. Solid line indicates mean score. Error bar indicates standard deviation.
|
The POSAS was known to be a more useful subjective tool than VSS for linear scar evaluation [23]. In this study, the mean POSAS scores was 23.17 out of 110 total, with a mean OSAS score of 12.10 out of 50 total and a mean PSAS score of 11.07 out of 60 total. As the smallest possible score of 11 indicates a normal skin and the maximum score 110 indicates the worst scar imaginable, the findings of our study represents high level of cosmetic satisfaction from patients who underwent the minimally-invasive harvest technique.
The Mexameter is narrow-band spectrophotometry device and measures the extent of vascularization and pigmentation based on the differences in light absorption of red and green light by hemoglobin and melanin, respectively. In this study, the Mexameter was used for two purposes. First, for the sake of objectivity in scoring, the authors score the vascularity and pigmentation of OSAS according to Mexameter value. Second, the Mexameter values were compared between the costal cartilage harvest site and the retroauricular skin incision site, which revealed no significant difference across the two surgical incisions.
A direct comparison of morbidities between the minimally-invasive and conventional costal cartilage harvest techniques would have been ideal. However, the authors of the study believe that to perform conventional costal cartilage harvest techniques is perhaps unethical, considering the clinical experiences with the minimally invasive technique. To overcome this limitation, we have adopted various kinds of scar evaluation scales, such as VAS, VSS, POSAS, and Mexameter assessments. In addition to various scar scales, we have compared the costal cartilage harvest site to the retroauricular skin incision site.
VAS pain, VAS cosmetic, Mexameter assessments, POSAS and OSAS scores were not significantly different between the two sites. However, the PSAS score of costal cartilage harvest site was significantly lower than that of retroauricular skin incision site. We have wondered why some patients scored the costal cartilage harvest site lower, even though they had answered that the overall cosmetic burden of costal cartilage harvest site was less than that of retroauricular skin incision site. We speculate that this discrepancy arises from the difference in a patient's ability to make first-hand observations of the costal cartilage harvest site, where a close observation of the retroauricular site is difficult. Similar values which were evaluated by observer (OSAS) had no statistically significant difference.
Surgical complication
The postoperative complications after the minimally-invasive was less than that reported for conventional costal cartilage harvest. Additionally, there were no major complications to report, due to the minimal invasiveness of the operation.
In conclusion, the minimally-invasive chopped costal cartilage harvest technique resulted in acceptable pain, cosmetic concern, and postoperative complications for most patients. We believe that costal cartilage is an acceptable donor for mastoid obliteration in CWD mastoidectomy, especially in the context of the extremely low donor site morbidity of the minimally-invasive technique presented in the study.
Go to :
 XML Download
XML Download