

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Otitis media (OM) is an infectious disease that frequently affects all age brackets, including children and adults [1]. The morbidity and complication rates of OM have been increasing in developing countries due to poor medical environments for early treatment, resulting in reductions in quality of life [2,3]. Appropriate early treatment, including the use of appropriate antibiotics, is essential, requiring information on bacteriology and antibiotic sensitivity. Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis are the bacterial species isolated most frequently from children with acute OM (AOM) and OM with effusion (OME) [4,5]. However, the dominant bacterial species in other types of OM and in other age brackets have not been definitively identified. The emergence of antibiotic resistant bacteria, including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin resistant-Enterococcus (VRE), vancomycin-resistant Staphylococcus aureus (VRSA), and quinolone resistant Pseudomonas, has caused a significant change in the distribution of the dominant bacteria in patients with OM [6,7,8].
To assess changes in the distribution of bacteria isolated in hospitals over the past 10 years from patients with OM and changes in their sensitivity to antibiotics, we divided patients with OM into the four subtypes most frequently encountered in clinical practices: AOM, OME, chronic OM (COM), and cholesteatomatous OM (CSOM). We attempted to culture bacteria from exudates and aural discharges (or otorrhea) of these patients and tested the antibiotic sensitivity of these bacteria. We compared these findings in pediatric and adult patients with OM and in patients with the four subtypes of OM.
MATERIALS AND METHODS
Patients
This study involved 2,833 patients who had undergone pus culture at five tertiary hospitals from January 2001 to December 2010, and who were diagnosed with AOM, OME, COM, or CSOM. Patients with AOM, COM, or CSOM had concurrent symptoms, such as a mucoidal or purulent aural discharge. COM was differentiated from CSOM based on the otoscopic appearance of the tympanic membrane, temporal bone computed tomography (TBCT) findings, the presence of cholesteatoma during surgery, and biopsy results. Aural discharge was collected from the patients, followed by bacterial culture and antibiotic sensitivity tests.
The 2,833 patients had an age distribution of 0-91 years (mean, 32.3±22.0 years) and consisted of 1,425 males and 1,408 females. Most of the patients did not receive antibiotic treatment for one month or longer before visiting the outpatient department, although some patients had previously been treated with topical antibiotics at local primary clinics. We excluded results from cases where contamination occurred during sample collection, as well as from patients with conditions that may have affected the bacteriologic environment of the middle ear, including patients receiving topical drugs or systemic antibiotics after a diagnosis of OM, patients who were receiving antibiotics for diseases other than OM, patients who were receiving steroids, and patients who were receiving chemotherapy or radiotherapy due to a malignant tumor or other reasons. This retrospective study was approved by the Institutional Review Board of Kyung Hee Medical Center (KMC IRB 1227-04).
Sample collection, bacterial culture test and antibiotic sensitivity test
Aural discharge samples were collected from 2,429 patients with AOM, COM, and CSOM during their first visit to the outpatient department. Effusion samples from 404 patients with OME were collected during surgery to insert a tympanostomy tube after making a radial shaped incision in the anterior inferior quadrant of the tympanic membrane. After cleaning the external auditory canal, the aural discharge was collected using a sterilized cotton swab while using a sterilized otoscope to prevent contact with the external auditory canal. The samples were placed in transport medium and transferred to the microbiology test laboratory. Each sample was inoculated into blood agar medium and thioglycollate liquid medium and cultured for 24 hours at 35℃. Bacteria were identified by Gram staining and biochemical tests. Fungi cultured in the blood agar medium were identified by culture on Sabouraud agar.
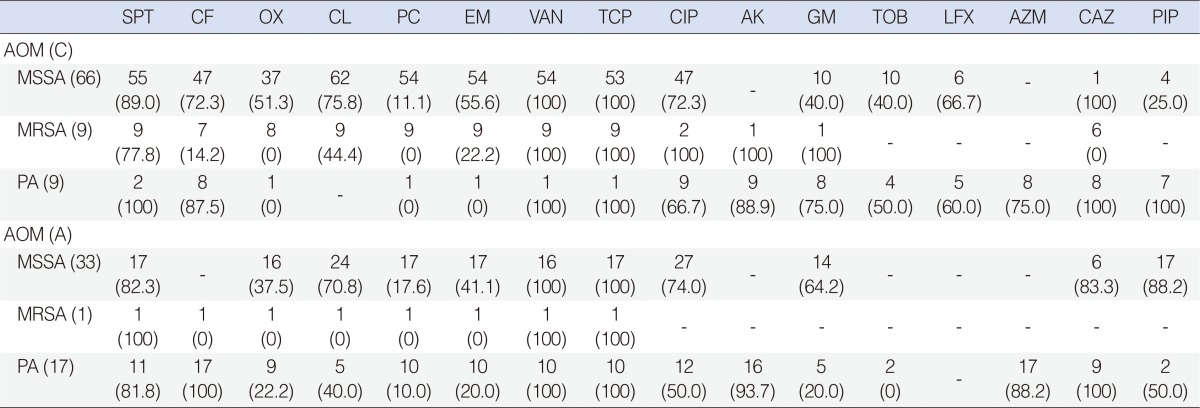
Antibiotic sensitivity was assayed by a microdilution method to determine the minimal inhibitory concentration (MIC; 4 hospitals) or by the Kirby-Bauer disc diffusion method (1 hospital). Colonies with MICs greater than 4 µg/mL, and with a diameter less than 10.0 mm in the vicinity of oxacillin discs (1.0 µg), were classified as MRSA, whereas colonies with MICs less than 4 µg/mL or with a diameter greater than 10.0 mm were considered methicillin-sensitive Staphylococcus aureus (MSSA). Antibiotic sensitivity testing was performed according to the guidelines of the National Committee for Clinical Laboratory Standards (NCCLS). Gram-positive bacteria were tested for their susceptibility to sulfamethoxazole/trimethoprim (SPT, co-trimoxazole), cephalothin (CF), oxacillin (OX), clindamycin (CL), penicillin (PC), erythromycin (EM), vancomycin (VAN), and teicoplanin (TCP), whereas Gram-negative bacteria were tested for their susceptibility to ciprofloxacin (CIP), amikacin (AK), gentamicin (GM), tobramycin (TOB), levofloxacin (LFX), and septrin (SPT). In addition, strains of Pseudomonas were tested for their susceptibility to CIP, AK, GM, TOB, LFX, aztreonam (AZM), ceftazidime (CAZ), and piperacillin (PIP).
Statistical analysis
The distribution of microorganisms present in patients with the 4 subtypes of OM and in children and adults was analyzed using the chi-square test. All statistical analyses were performed using SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA). A P-value <0.05 was considered statistically significant.
RESULTS
Types and frequencies of cultured bacteria in patients with the four OM subtypes
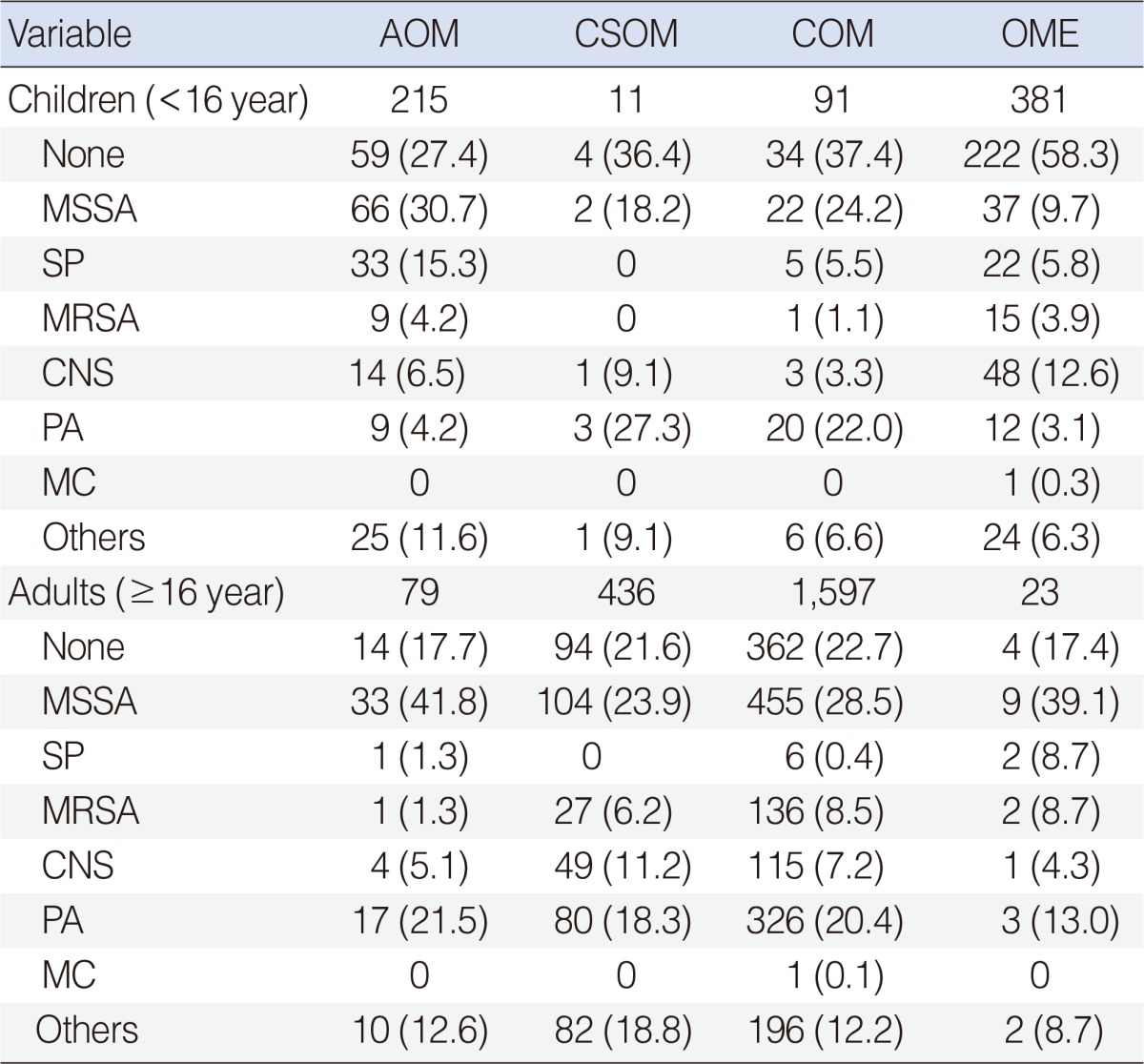
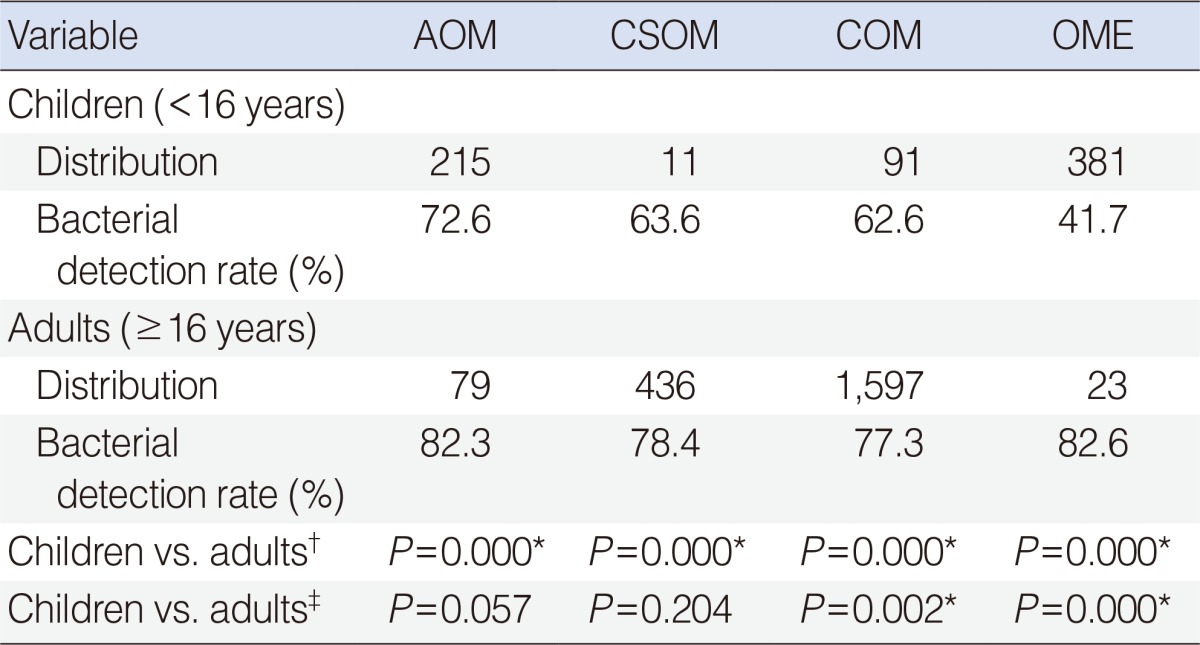
The total of 2,833 patients consisted of 698 pediatric patients aged<16 years and 2,135 adult patients aged≥16 years (Table 1). The 698 pediatric patients included 215 with AOM (30.8%), 381 with OME (54.6%), 91 with COM (13.0%), and 11 with CSOM (1.6%). In comparison, the 2,135 adult patients included 1,597 with COM (74.8%), 436 with CSOM (20.4%), 79 with AOM (3.7%), and 23 with OME (1.1%). Thus, AOM and OME were predominant in the pediatric group, whereas COM and CSOM were predominant in the adult group. The difference in microorganism distribution for each of the 4 subtypes between children and adults was statistically significant (P=0.000) (Table 2).
In the pediatric group, the rates of bacterial isolation were 72.6% in patients with AOM, 63.6% in patients with CSOM, 62.6% in patients with COM, and 41.7% in patients with OME. In these four subgroups of adult patients, the rates of bacterial isolation were 82.3%, 78.4%, 77.3%, and 82.6%, respectively. The differences in bacterial isolation rate for patients with OME and CSOM differed significantly between children and adults (P=0.000 each) (Table 2).
The most frequently identified bacterial species in both adults and children was MSSA. Although the frequency of the identified bacteria varied depending on OM subtype, the species most frequently isolated were MSSA, Streptococcus pneumoniae (SP), MRSA, coagulase negative Staphylococcus (CNS), and Pseudomonas aeruginosa (PA). MSSA (30.7%) and SP (15.3%) were the predominant species identified in pediatric patients with AOM, CNS (12.6%) and MSSA (9.7%) in pediatric patients with OME, MSSA (28.5%) and PA (20.4%) in pediatric patients with COM, and MSSA (23.9%) and PA (18.3%) in pediatric patients with CSOM. In comparison, MSSA (41.8%) and PA (21.5%) were the most frequently identified species in adult patients with AOM, MSSA (39.1%) and PA (13.0%) in adult patients with OME, MSSA (28.5%) and PA (20.4%) in adult patients with COM, and MSSA (23.9%) and PA (18.3%) in adult patients with CSOM.
In addition, 59 other bacterial species were identified, mainly in adults with COM. None of these species was isolated from two or more patients. Fungi were isolated from two patients, with both being Candida species.
Antibiotic sensitivity tests in adult and children
We found that bacteria isolated from children were sensitive to a mean 12.8±2.3 antibiotics, whereas those isolated from adults were sensitive to a mean 10.3±1.4 (P=0.002), with bacteria in these groups having >80% sensitivity to a mean 6.4±3.6 and 4.7±1.9 antibiotics, respectively (P=0.001).
Acute otitis media
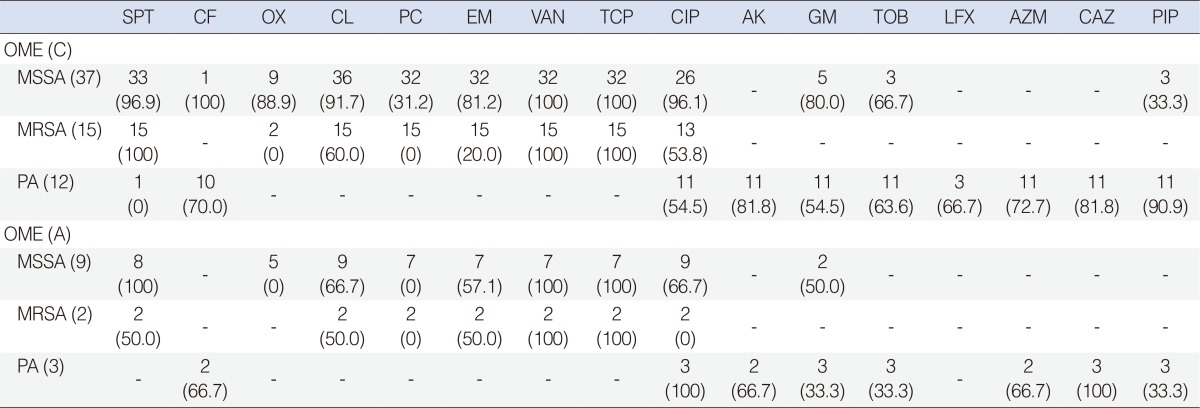
MSSA isolated from both children and adults showed 100% sensitivity to VAN and TCP and >80% sensitivity to SPT, but <20% sensitivity to PC, whereas MSSA isolated from adults had higher sensitivity to PIP than MSSA isolated from children. MRSA isolated from children showed 100% sensitivity to VAN, TCP, and SPT, and to quinolones such as CIP, AK, and GM. PA isolated from children showed 100% sensitivity to VAN, TCP, SPT, CAZ, and PIP, and high sensitivity to CF and AK, whereas PA isolated from adults showed 100% sensitivity to VAN, TCP, CAZ, and CFP, and high sensitivity to SPT, AK, and AZM. Both groups had low response to OX, PC, and EM (Table 3).
Otitis media with effusion
MSSA isolated from both groups showed 100% sensitivity to VAN and TCP. MSSA isolated from children had 100% sensitivity to CF and high sensitivity to SPT, OX, CL, EM, and GM, whereas MSSA isolated from adults had 0% sensitivity to OX and PC, and lower sensitivity to other antibiotics than MSSA isolated from pediatric patients. MRSA isolated from both groups showed 100% sensitivity to VAN and TCP, and MRSA isolated from pediatric patients had 100% sensitivity to SPT. Isolated PA had lower antibiotic sensitivity than other bacterial species. PA isolated from pediatric patients had high sensitivity to AK, CAZ, and PIP, whereas PA isolated from adults showed 100% sensitivity to CIP and CAZ (Table 4).
Chronic otitis media
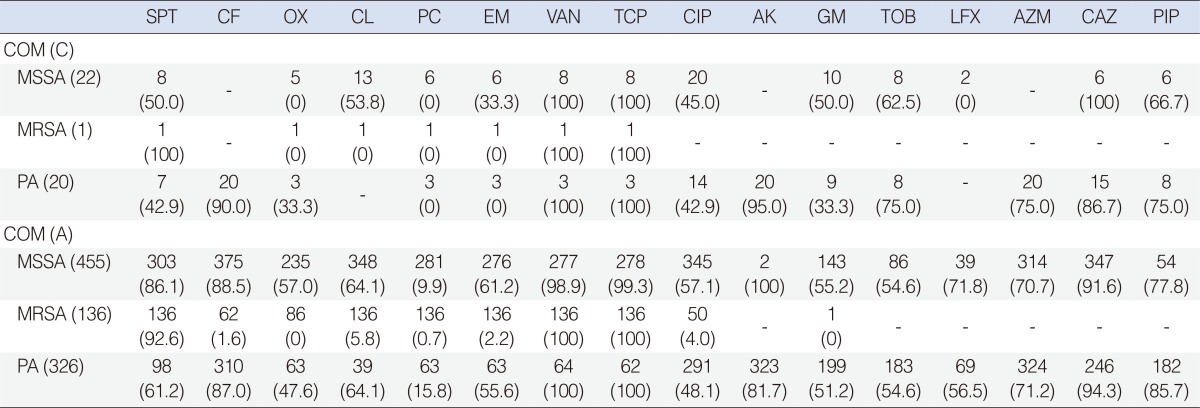
MSSA isolated from children and adults showed 0% sensitivity to OX and PC. MSSA isolated from children showed 100% sensitivity to VAN and TCP, whereas MSSA isolated from adults had high, but less than 100%, sensitivity to SPT, CF, VAN, TCP, and CAZ. MRSA isolated from children showed 100% sensitivity to SPT, VAN, and TCP, whereas MRSA isolated from adults showed 100% sensitivity to VAN and CIP and high sensitivity to SPT, but low (≤6%) sensitivity to other antibiotics. PA isolated from children had 100% sensitivity to VAN and TCP, and high sensitivity to CF, AK, and CAZ. PA from adults showed similar results, but had higher sensitivity to PIP than PA isolated from children (Table 5).
Cholesteatomatous otitis media
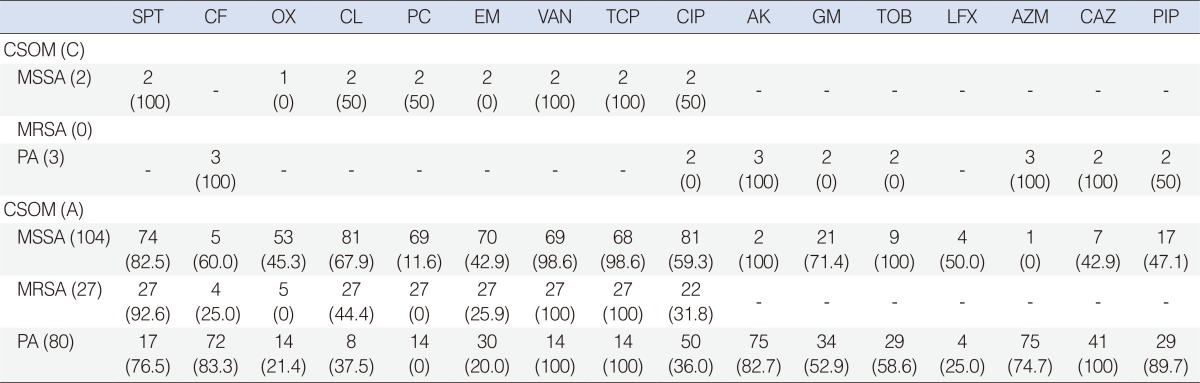
MSSA was isolated from two children with CSOM and PA from 3, but none was positive for MRSA. MSSA isolated from children had 100% sensitivity to SPT, VAN, and TCP, whereas MSSA isolated from adults had high, but less than 100%, sensitivity to these three antibiotics. MRSA isolated from adults had 100% sensitivity to VAN and TCP and high sensitivity to SPT, but no sensitivity to OX and PC. PA isolated from patients in the pediatric group showed 100% sensitivity to CF, AK, AZM, and CAZ, whereas PA isolated from adults had 100% sensitivity to VAN, TCP, and CAZ and high sensitivity to CF, AK, and PIP, but low or no sensitivity to OX and PC (Table 6).
Changes in the distribution and antibiotic sensitivity of MSSA, MRSA, and PA in children and adults from 2001 to 2010
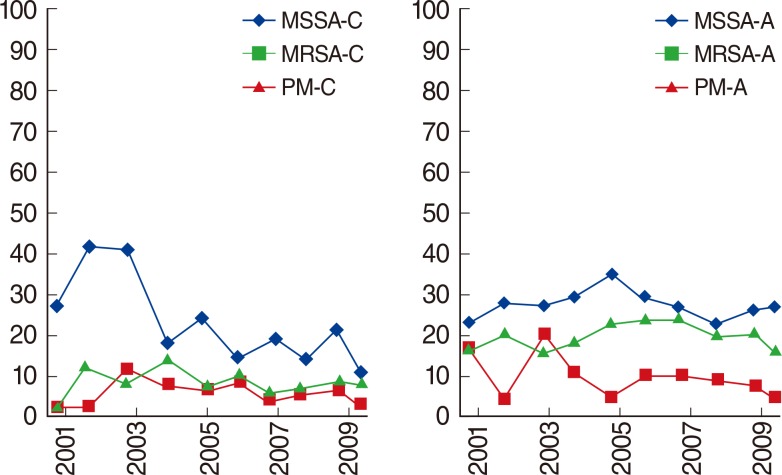
We also assessed changes in the distribution of the three major bacteria over the past 10 years in pediatric and adult patients, regardless of OM subtype. In pediatric patients, MSSA had the highest frequency (approximately 39.5%) in such patients from 2000 to 2003, decreasing thereafter at rates of 6%-9% every 2 years, with a frequency in 2010 of 8.3%. MRSA had a frequency of 9% in 2003, decreasing steadily thereafter. PA had a frequency of 11.6% in 2004, also decreasing thereafter. In 2010, however, the overall frequency of PA was 5.6%, higher than that of MRSA.
In adults, the frequency of MSSA steadily increased from 2001 to 2005, being 34.2% in 2005. Its frequency subsequently decreased, to 23.5% in 2008, but has remained unchanged since. The frequency of MRSA was 15.6% in 2001, increasing to 18.9% in 2003 and steadily decreasing thereafter, to 3.2% in 2010. The frequency of PA was approximately 22% from 2005 to 2007, thereafter maintaining a mean frequency of approximately 15% (Fig. 1).
DISCUSSION
Bacterial infection is among the most important etiological characteristic of OM, making the appropriate choice of antibiotics the most critical step in OM treatment in both children and adults. Most recent studies on bacteria in aural discharge fluid have involved patients with chronic suppurative OM or OME [6,7,8], with the results utilized in choosing antibiotics. As hospital environments have changed, however, bacterial pathogenicity has increased, including increases in the number of multidrug-resistant bacteria. Guidelines on antibiotic treatment of OM should therefore be continuously updated, based on the identification and antibiotic resistance of bacteria. We therefore assessed the identity and antibiotic resistance of bacteria isolated over a 10 year period from children and adults with the four subtypes of OM most frequently seen in clinical practices, AOM, OME, COM, and CSOM.
We divided our subjects into pediatric and adult groups based on an age of 16 years, when adolescent growth and development have ceased [9]. Consistent with previous reports, we found that AOM and OME were more frequent in pediatric than in adult patients, whereas COM and CSOM were more frequent in adults [10,11]. We therefore analyzed the major pathogenic bacteria in each subtype of OM, the sensitivity of these bacteria to antibiotics, and their changes in frequency from 2001 to 2010 in children and adults. We also separately assessed the major pathogenic bacteria, MSSA, MRSA, and PA, the latter two of which have developed resistance to antibiotics.
AOM was more frequently observed in pediatric than in adult patients with aural discharge due to differences in immunologic function and the anatomic structure of the Eustachian tubes. MSSA was the predominant species isolated from both groups, and the rates of isolation of SP and CNS were higher in children than in adults. CNS species, including S. capitis, S. epidermis, S. haemolyticus, and S. auricularis, were the most frequently isolated Gram-positive staphylococci observed in the normal flora of the external auditory canal [12]. Thus, the high frequency of CNS in pediatric patients with AOM was likely due to the unexpected contamination of aural discharge samples during collection, despite efforts to minimize contamination by using a sterilized otoscope after cleaning the external auditory canal. We also found that PA was the second most frequent bacterial species isolated from adults with AOM. This was likely due to an increase in antibiotic resistant bacteria.
Bacteria and viruses are frequently isolated from the exudates of patients with OME. Since most patients with OME have a previous history of AOM, OME is considered an extension of AOM. In pediatric patients, aural discharges were more likely serous or mucoidal exudates, with fewer bacteria, than purulent exudates. Moreover, viruses were more likely responsible for OME in the pediatric group. CNS strains were the most frequently isolated organisms in the pediatric group, for reasons similar to those in patients with AOM, followed by MSSA. All strains of MSSA and MRSA isolated from both pediatric and adult patients were sensitive to VAN and TCP. MSSA isolated from pediatric patients with OME had greater sensitivity to OX, CL, and EM than strains isolated from pediatric patients with AOM, whereas PA strains isolated from both groups of pediatric patients had high, but similar, sensitivity to CAZ and PIP.
COM, defined as non-cholesteatomatous OM, can occur when inflammation of the middle ear cavity progresses to chronic status via recurrent OM or OME. COM may be caused by poor treatment of patients with AOM or recurrent inflammation. Several recent studies have assessed bacteria in patients with COM and CSOM [7,13]. We and others have found that MSSA was isolated more frequently than PA [14]. Although the numbers of pediatric and adult patients differed significantly (91 vs. 1,597), MSSA was dominant in both groups, followed by PA. The higher frequency of MSSA in patients with COM was likely due to the appropriate use of antibiotics and the efficient prevention of pathogenic infection. Over time, the no growth rate increased in the pediatric group and the frequency of PA isolation decreased in the adult group. The three major bacteria in adults and children with COM had 100% or high sensitivity to VAN and TCP. In adults, isolated MSSA and MRSA were highly sensitive to SPT, whereas, in both groups, PA had low sensitivity to all quinolone-class antibiotics except for AK.
CSOM occurs when keratinized squamous epithelium invades the middle ear cavity and destroys adjacent bone tissue, causing inflammation [15,16]. We found that both pediatric and adult patients with CSOM had acquired cholesteatoma, the most common type in both groups. Bacteria were isolated from 11 pediatric patients with CSOM, including PA from three patients and MSSA from 2. Although the isolation rate was 63.6%, the results of antibiotic sensitivity tests were not significant due to the small number of patients. Thus, larger-scaled studies of pediatric patients with CSOM are required. The distribution of bacteria in adults with CSOM and the antibiotic sensitivity of these bacteria were generally similar to results observed in adults with COM. Our finding of a higher frequency of MSSA than of PA was likely due to longer treatment times, repeated treatments, and increased cognition about individual hygiene. Our findings indicate that surgical removal of lesions and prevention of recurrence by the use of appropriate antibiotics are required for patients with COM and CSOM.
Due to significant differences in populations with the different types of OM, we assessed changes over time in the bacterial distribution of the three major types of bacteria in the entire cohort of patients with OM. We found that MSSA frequency was high in the early 2000s in pediatric patients, most of whom had AOM and OME, but decreased steadily thereafter. The frequencies of MRSA and PA showed mean distributions of 5%-10%, but no rapid change over 10 years. The higher frequency of MSSA in the pediatric group in the early 2000s was likely due to these patients visiting the authors' hospital after their status became more severe, as a result of poor recognition by patients and doctors or insufficient treatment of infantile OM in local primary clinics. The diagnostic rate of MSSA in the authors' hospital has decreased since 2004, when detailed guidelines on the treatment of infantile OM were published [17]. In adults, most of whom had COM and CSOM, the frequency of MSSA was higher than that of PA. Although their 10-year frequencies did not change markedly, the frequency of MRSA increased rapidly in the early 2000s, peaking at 18.9% in 2003, but gradually decreased thereafter.
Several studies have analyzed the bacteriology of om, but most focused on COM and CSOM in adults, especially regarding associated nosocomial infections such as MRSA and PA [7,13]. Although comparisons of these studies showed that the frequency of MRSA tended to increase, being 0.8% in 1979 [18], 4.7% in 1987 [19], 17.9% in 1995 [20], and 18.8% in 1997 [21], we observed that the frequency was maximal in 2003, at 18.9%, thereafter decreasing until 2010. The frequency of PA, reported to be 18.4% [19], showed a tendency to increase until 2001. After that, it remained steady, increased to 22% from 2005 to 2007, and then decreased and leveled off at 15%. We found that MSSA and SP accounted for the majority of bacteria isolated from patients with AOM and OME, both of which are common diseases in children, and that bacteria isolated from pediatric patients were more sensitive to antibiotics than bacteria isolated from adults. Indeed, MSSA and PA accounted for the majority of bacteria isolated from patients with COM and CSOM, both of which are common diseases in adults. The frequency of MRSA was significantly higher in adults than in children. Moreover, high percentages of bacteria isolated from adult patients were sensitive only to SPT, VAN, and TCP.
The present study had limitations. First, all cultures were not taken in the same environment, which may have led to differences in contamination rate. Second, although samples were collected during the first visit to the outpatient department, some patients may have been prescribed antibiotics and/or otic drops at primary clinics before visiting the tertiary hospital. However, because pus cultures were not performed at primary clinics for all patients, we were unable to determine patient status at first diagnosis of OM. Moreover, since this was a retrospective chart review, we analyzed only bacteriology and antibiotic sensitivity in patients with OM who had undergone pus culture from January 2001 to December 2010. A future study comparing bacteriology of patients with and without previous antibiotic treatment is warranted.
The recent overuse and misuse of antibiotics has caused alterations in major bacterial strains and their sensitivity to antibiotics, making this condition more difficult to treat. Care should therefore be taken when considering the use of antibiotics in these patients to decrease the incidence of antibiotic-resistant microorganisms although most patients with OM with or without otorrhea prefer oral to topical antibiotics, and doctors customarily prescribe oral antibiotics. Because patients with otorrhea respond well to ototopical treatments and aural dressing, most do not require systemic therapy. Periodic bacteriological examination of patients with OM, and pretreatment antibiotic sensitivity tests, may help select appropriate antibiotics for treatment [7,22].
In conclusion, analysis of patients treated over a recent 10-year period showed that MSSA were the bacteria most frequently isolated from the aural discharge of children and adults with OM, regardless of OM type, with bacteria in both children and adults highly sensitive to VAN, TCP, and SPT. Bacteria isolated from children were susceptible to many more antibiotics and showed higher antibiotic sensitivity than bacteria isolated from adults.
 XML Download
XML Download