

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Vocal fold vibration is the source of voice production, which is directly driven by the biomechanical properties of the layered vocal fold lamina propria. Scarring disrupts this layered structure and causes significant change in vocal fold tissue biomechanics, resulting in a range of voice problems that often significantly compromise patient quality of life [1].
Mesenchymal stem cells (MSCs), vitamin A, corticosteroids, mitomycin-C (MMC), hyaluronic acid (HA)-based biomaterials, decellularized scaffold materials, and hepatocyte growth factor (HGF) have been used [1]. Despite several advantages, the high cost and foreign body or infectious/immune reactions to foreign materials have always been discussed. Because of such problems, the necessity for inexpensive autologous materials, as well as for a treatment that will not require repeat procedures, have been increasingly recognized.
Platelet-rich plasma (PRP) is a platelet concentrate that has been widely used in a variety of clinical applications. A number of studies show that PRP enhances and accelerates both soft tissue and hard tissue healing [2,3]. The effectiveness of PRP is based on its high level of growth factors such as platelet derived growth factor (PDGF), transforming growth factor-β (TGF-β), epidermal growth factor (EGF), vascular endothelial growth factor (VEGF), and insulin-like growth factor (IGF), etc. These growth factors are important in modulating mesenchymal cell recruitment, proliferation, and extracellular matrix (ECM) synthesis during the healing process [4,5].
In the current study, the role of PRP in the prevention of vocal fold scarring was examined using a rabbit model to observe the histological effects in vivo of a new injection material for vocal fold diseases, an approach that could be readily translated to clinical practice.
Go to : 
MATERIALS AND METHODS
Preparation of autologous PRP
Twelve adult New Zealand White rabbits weighing 4,000-4,500 grams each were used. All rabbits were male and treated in accordance with the guidelines of the Korea Food and Drug Administration Guide for the Care and Use of Laboratory Animals, and the animal use protocol was approved by the Institutional Animal Care and Use Committee of Gyeongsang National University. All animals received general anesthesia using a combination of midazolam 1 mg/kg intramuscular (Roche, Basel, Switzerland) and ketamine 70 mg/kg intramuscular (Fada, Buenos Aires, Argentina). Under strict aseptic conditions, an 8.7 mL blood sample was drawn from the auricular artery of each rabbit with a 21 G needle. A 10 mL syringe preloaded with 1.3 mL of anticoagulant citrate dextrose solution was used to avoid coagulation. One millimeter of each sample was set apart for cell counting. All blood draws were performed by one investigator (SHW).
Each blood sample was centrifuged for 15 minutes at 72 g at 4℃, resulting in the three following layers: the inferior layer composed of red cells, the intermediate layer composed of white cells, and the superior layer made up of plasma. The 6 mL plasma layer was centrifuged for another 5 minutes at 1,006 g in order to obtain a two-part plasma sample: the upper part consisting of 5.5 mL of platelet-poor plasma (PPP) and the lower part consisting of 0.5 mL of PRP. The PPP was first aspirated to avoid its mixing with the PRP. The PRP was then gently aspirated with another pipette and placed in a sterile tube. The platelet count was carried out in the whole blood and in the PRP sample with a Neubauer camera using the Brecher and Cronkite direct manual method [6,7] (Fig. 1).
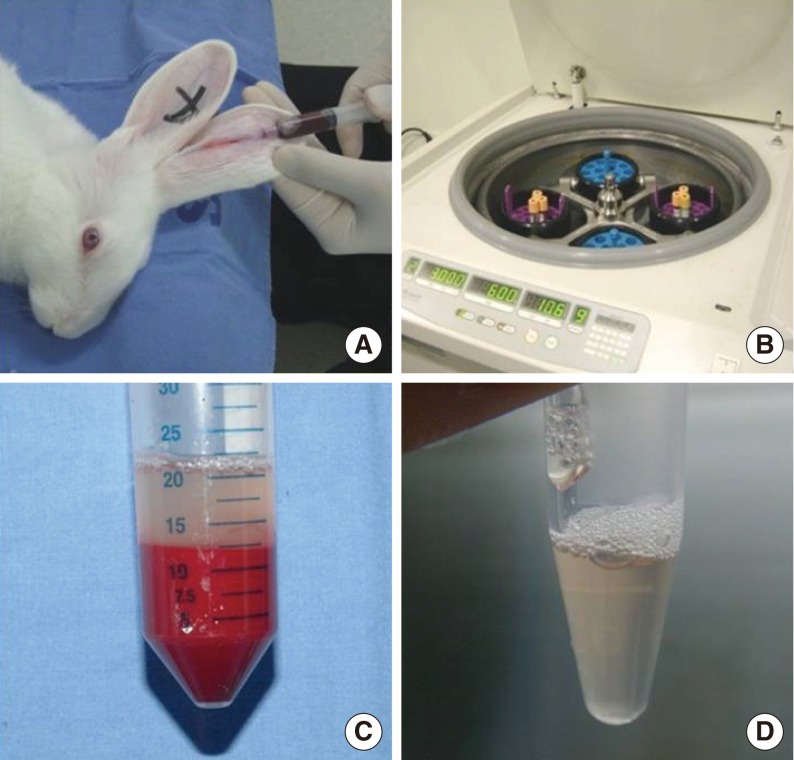 | Fig. 1Preparation of autologous platelet-rich plasma (PRP). (A) Blood samples from auricular artery of each rabbit were collected. (B, C) Each blood sample was centrifuged resulting in the three following layers. (D) The PRP was then gently aspirated with another pipette and placed in a sterile tube.
|
Morphologic and histological examination
To analyze the morphologic and histological change, vocal folds were obtained from animals. The animals were sacrificed by administration of a high dose of pentobarbital sodium.
Morphologic examination of rabbit vocal folds was performed using a nasal speculum (7 cm, KASCO, Sialkot, Pakistan) and a direct endoscope (0°, 2 mm, 4 mm, Karl Storz, Tuttlingen, Germany). Once visualized, a CO2 laser (15 W, 1 second; NIIC R204, Tokyo, Japan) was used to perform uniform bilateral vocal fold stripping at the posterior part of the vocal fold.
Immediately after laser scarring, the prepared PRP was injected into the right vocal fold (PRP-injected side) and normal saline was injected into the left vocal fold (normal saline-injected side). The method of injection was a 1 mL syringe with a 25 G spinal needle (length, 9 cm) and the injected volume was 0.5 mL on either side.
Endoscopic examination was performed using a nasal speculum and direct endoscope to assess the morphologic changes of the vocal folds at 2, 4, and 12 weeks after injection (Fig. 2). Morphological changes observed, including surface irregularities, granulation tissue formation, and atrophic change were investigated and graded by a two otolaryngologists, and were recorded on a subjective scale of 0-3, ranging from absent to severe (0, absent; 1, mild; 2, moderate; 3, intense). The analyses were performed on both normal saline-injected sites and PRP-injected sites. Images were captured with an endoscope and graded later.
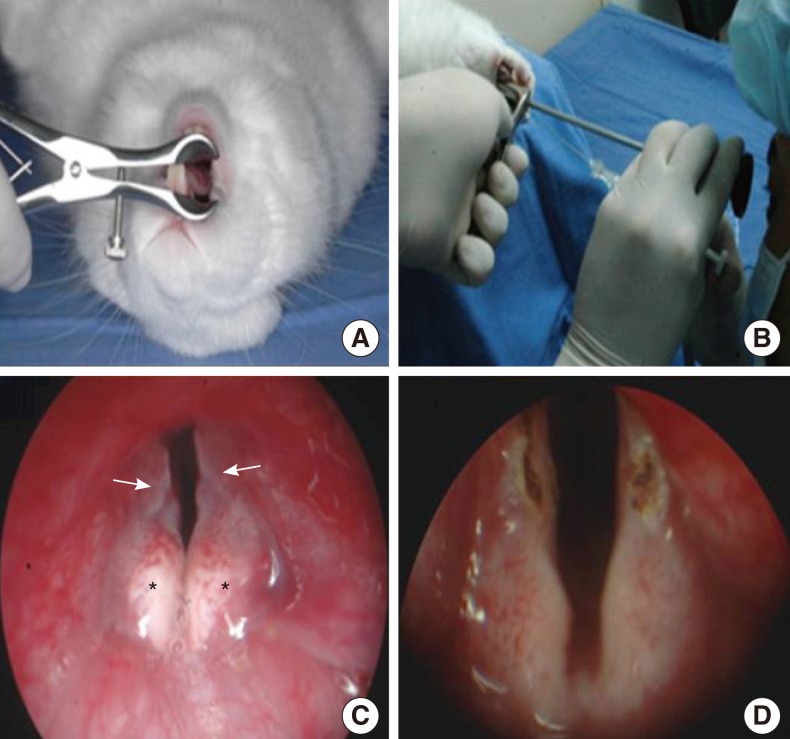 | Fig. 2(A, B) Morphologic examination was performed using a nasal speculum and a direct endoscope. (C) Normal vocal folds of rabbit (arrow, vocal fold; *, arytenoid). (D) Vocal fold mucosa was injured bilaterally using a CO2 laser, and injected with platelet-rich plasma in right and injected with normal saline in left vocal fold.
|
Histopathological analyses of the specimens were done 12 weeks later the animals were euthanized and the tissues were stained using H&E for assessing inflammatory reaction and inflammatory cell infiltration, and masson trichrome (MT) for assessing collagen deposition. The slides were viewed with a Nikon Eclipse E800 microscope (Nikon, Tokyo, Japan). Collagen was examined at original magnification ×40 in the lamina propria. Histological analysis was blindly checked and graded from 0 to 3 by two pathologists (0, absent; 1, mild; 2, moderate; 3, intense).
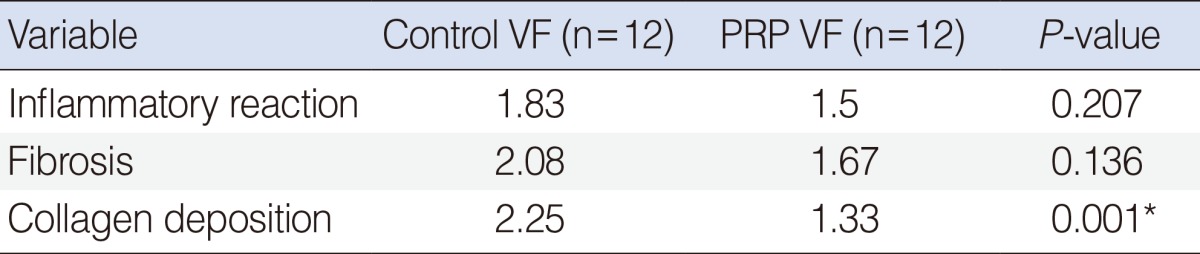
The analyses were performed on both normal saline-injected sites and PRP-injected sites, and statistical comparisons were performed between both sides using a McNemar test. A P-value<0.05 was considered statistically significant. For reliability of measurements, 10% of these slides were selected at random and measurements were repeated.
Western blot assay of growth factors
To analyze the relative expression of growth factors, vocal cords were obtained from two animals 14 days after surgery. The right vocal fold (PRP-injected side, treatment group) was dissected and the previous wound was located. The vocal fold fragments (5 mm square in size) were removed for western blot assay. After that the left vocal fold (normal saline-injected side, control group) was dissected using the same method.
The vocal folds were lysed in a lysis buffer (50 mM Tris [pH 7.5], 100 mM NaCl, 1 mM EDTA, 1% NP-40, 10% glycerol, leupeptin [50 lg/mL], aprotinin [50 lg/mL], 0.2 M PMSF, 1 mM Na3VO4, and 1 mM NaF) and incubated for 10 minutes on ice. Tissue lysates were collected and centrifuged for 10 minutes at 4℃ at 13,200 rpm. Protein concentration in tissue lysates was determined by a Quant-iT assay kit (Molecular Probes, Eugene, OR, USA). An equal amount (10 mg) of protein for each sample was resolved with 10% sodium dodecyl sulfate-polyacrylamide gel electrophoresis and transferred to nitrocellulose membranes (Amersham Pharmacia Biotech, Buckinghamshire, UK). The membranes were blocked with 1% skim milk in Tris-buffered saline containing 0.1% Tween-20 (TBST), and sequentially incubated with specific antibodies for PDGF (1:1,000), EGF (1:1,000), VEGF (1:1,000), TGF-β (1:1,000), and glyceraldehyde 3-phosphate dehydrogenase (1:2,000; Santa Cruz Biotechnology Inc., Santa Cruz, CA, USA). The membranes were washed with TBST and processed using horseradish peroxidase-conjugated anti-rabbit antibodies. The antibodies were purchased from Abcam (Austin, TX, USA). Densitometry was performed using the ImageJ 1.38 (Windows version of NIH Image, http://rsb.info.nih.gov/nih-image/) software.
Go to :
RESULTS
Concentration of platelets in PRP compared to serum
PRP was prepared in approximately 40 minutes. The concentration of platelets was found to be increased in the PRP compared to serum. In the PRP, the mean platelet concentration was 1,315,000 platelets/mm3 (range, 923,000 to 1,860,000 platelets/mm3; SD, 221,730 platelets/mm3) from an original blood concentration of 310,133 platelets/mm3 (range, 240,000 to 428,000 platelets/mm3; SD, 45,233 platelets/mm3).
Morphological analysis
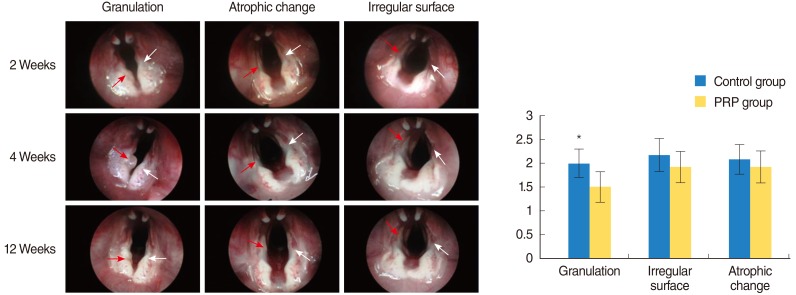
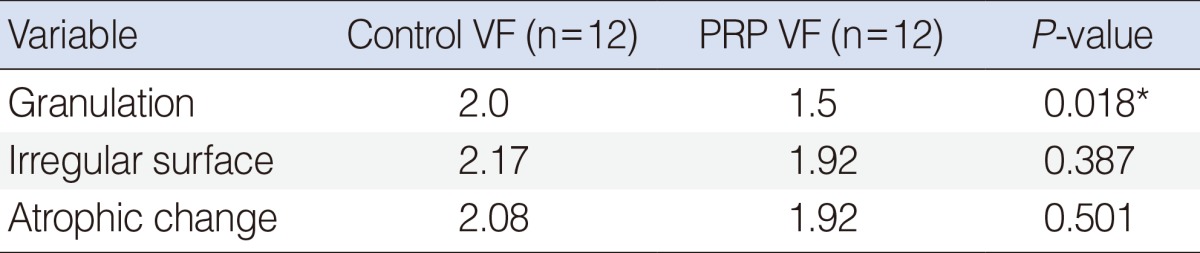
As compared with the normal saline-injected vocal fold, the PRP-injected vocal fold showed a decrease in granulation tissue throughout the entirety of the injured vocal folds by visual inspection at the time of endoscopy (Table 1), but the difference in irregular surface and atrophic change was not significant (Fig. 3).
Histopathological analysis
Collagen was found chiefly in the lamina propria of the vocal folds. As seen with MT for assessing collagen deposition, the normal saline-injected vocal fold showed a significant increase in collagen deposition throughout the entirety of the injured lamina propria (P<0.05). On the PRP-injected side, however, collagen was well organized and was distributed chiefly in the PRP-injected lamina propria without excessive deposition (Table 2). In contrast to the findings with collagen, there were no significant differences in the densities of fibrosis and inflammatory reaction between the normal saline-injected vocal fold and PRP-injected vocal fold (Fig. 4).
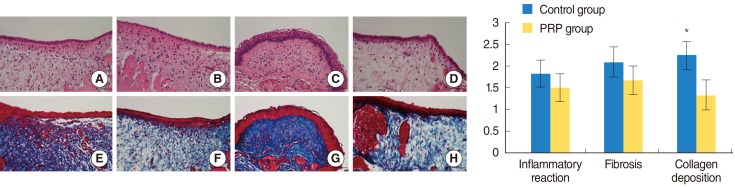 | Fig. 4Histological findings of platelet-rich plasma (PRP)-treated group and control group. PRP-treated side (B, D) and control side (A, C). There were no significant differences in the densities of fibrosis and inflammatory reaction between the control and PRP-treated groups. Histological finding of PRP-treated group in coronal plane. PRP-treated side (F, H) showed better wound healing with moderate collagen (stained blue) compared with control side (E, G) showed dense collagen deposit (stained blue). *P<0.05.
|
Growth factor expression analysis
A western blot assay performed 14 days after surgery found that the PRP-treated group showed marked expression of several growth factors, including PDGF, TGF-β, VEGF, and EGF. These factors have been reported to prevent foreign body reactions, tissue necrosis, or extensive fibrosis (Fig. 5). However, a western blot assay after the 12 week later which did not marked expression of growth factors.
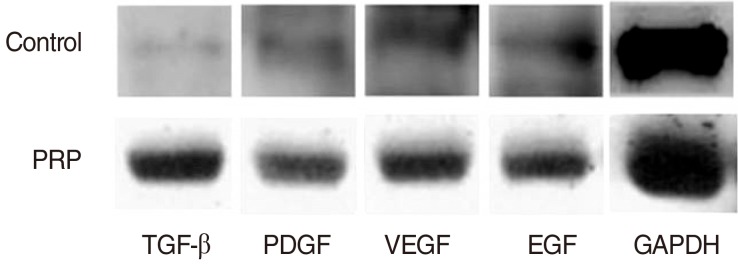 | Fig. 5Western blotting (A) and densitometric analysis (B). Expression of growth factors in platelet-rich plasma (PRP) treated group 14 days after surgery. Western blot showed strong expression of all tested growth factors in PRP treated group. TGF-β, transforming growth factor-beta; PDGF, platelet-derived growth factor; VEGF, vascular endothelial growth factor; EGF, epidermal growth factor.
|
Go to :
DISCUSSION
Prophylactic treatments are based on the notion that the acute healing phase including the proliferative phase represents a critical period, because migrating inflammatory cells and resident fibroblast begin to synthesize ECM 2-3 days following injury. Thus, therapeutic interventions are generally administered at the time of the injury for minimize eventual scar formation [8-10]. MSCs, vitamin A, corticosteroids, MMC, HA-based biomaterials, decellularized scaffold materials, and HGF have all been used in animal models during the past year [1,11].
MMC has been used in attempts to prevent scarring of the vocal fold and glottic stenosis [12-14]. It is suspected that as MMC inhibits fibroblast proliferation, MMC might reduce not only collagen synthesis but also the synthesis of other interstitial proteins required for optimal vibration. However, Gray et al. [15] reported that topical administration of MMC to injured skin of rats induced down-expression of the elastase, hyaluronidase, and procollagen genes in dermal fibroblasts, resulting in poor wound healing. Thus, the application of MMC at vocal fold wounds remains controversial to date.
Of the many cytokines and growth factors that affect wound healing and scarring, HGF has recently drawn considerable attention because of its demonstrated antifibrotic activity during wound healing [16-18]. Despite several advantages, the high cost of HGF and other growth factors and the attendant required injection of synthetic materials remain drawbacks. It is also important to keep in mind that wound healing is not determined by any single growth factor. Because of these and other such concerns, the need for more convenient and inexpensive autologous materials continues to grow.
Emerging new therapies such as PRP can have an adjunctive role in a standardized, quality treatment plan. The application of autologous PRP to soft tissue healing has been a subject of great interest for much of the past two decades. Multiple growth factors are present in high concentrations within PRP. Some of the most important of these include PDGF, TGF-β, VEGF, EGF, and IGF. PDGF, TGF-β, VEGF, and EGF have been shown to be increased 3 to 7 times in autologous PRP as compared with baseline levels, but the concentration of IGF-1 has not been shown to increase [19].
PRP has been shown to initiate and modulate soft tissue healing. in vivo prospective controlled studies as well as retrospective and cost effectiveness studies documenting the effects of this therapy have been published [20-23]. Its biocompatible and biodegradable properties prevent the PRP from inducing foreign body reactions, tissue necrosis, or extensive fibrosis [24-27]. In addition, in vitro research has shown that platelets contain components and properties essential for wound healing [28]. Another significant advantage of PRP is that it can be obtained easily and used promptly during surgery.
In the current study, the effectiveness of PRP in the prevention of vocal fold scarring was examined using an in vivo rabbit model. The results were encouraging. The entire process of preparing the autologous PRP took an average of 40 minutes. The mean platelet concentration was 1,315,000 platelets/mm3, which was an effective concentration to apply the vocal fold scar [29]. We observed markedly increased expression of growth factors (PDGF, TGF-β, VEGF, and EGF) in the vocal fold fragment in the PRP-treated group 14 days after surgery, suggesting that PRP acts as a source of growth factors and accelerates vocal fold regeneration. These growth factors have been reported to prevent foreign body reactions, tissue necrosis, or extensive fibrosis [24-26]. However, a western blot assay performed 12 weeks later did not show marked expression of the same growth factors. Thus, we guess that the PRP had an effect at an early phase in wound healing and that this effect did not last for a long period. Probably the platelet released the growth factors and attracted the other growth factor at early phase. It appears that the early phase of scar formation is key, as it is during this time that collagen and hyaluronic acid deposits are determined.
The present study indicated that PRP prevented excessive collagen deposition and resulted in well organized collagen deposit in injured vocal folds, whereas the control group showed dense collagen accumulation. The PRP-treated group showed a significant decrease in granulation tissue throughout the entirety of the injured vocal folds. Overall, PRP appeared to help maintain the layered structure of the injured vocal fold.
The benefits of autologous PRP can be summarized as follows: (1) offers high potency: multiple growth factors are present in high concentrations within PRP; (2) has the ability to produce the desired effect: PRP prevented excessive collagen deposition and controlled well organized collagen deposit; and (3) consists of both quantitative and qualitative components: PRP appeared to help maintain the layered structure of the injured vocal fold. Thus, PRP is an effective material for the prevention and healing of scarring in laryngeal surgery patients.
This study has several limitations. For example, in the procedure of wound healing, hyaluronic acid plays an important role. However, HA staining was not performed in this study. Therefore, we determined the effect of PRP using only collagen staining. This does not provide a clear and comprehensive picture of wound healing in vocal fold scarring. In addition, we analyzed the growth factors at only one time point, two weeks following the surgery. While that was a reasonable time to evaluate the wound healing it was not representative of the entire healing process. Consequently, more research is required into the role of PRP in the vocal fold wound healing process, the vocal folds' ultimate structure, pliability of the healed vocal folds, and quantification of the various growth factors. Another limitation of our study was the observer bias that could result from the necessarily subjective grading of our morphologic and histologic findings. We tried to decrease the bias, however, and all findings were confirmed by two otolaryngologists and two pathologist.
Injection of injured vocal folds with PRP led to improved wound healing and fewer signs of scarring as demonstrated by decreased inflammation and excessive collagen deposition in the treated vocal folds compared with the untreated folds. These results could be useful for researchers in the growing fields of tissue repair and experimental wound healing.
Go to :
 XML Download
XML Download