

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Since the introduction of a safe and reliable laryngopharyngeal sensory testing apparatus in 1993, laryngopharyngeal sensation has been increasingly assessed to delineate the role of laryngopharyngeal sensory deficit in the pathogenesis of upper aerodigestive tract disorders [1,2,3,4,5,6,7,8,9]. Laryngopharyngeal sensory motor function is evaluated by administering endoscopically directed pulses of air to the laryngeal mucosa. The lowest stimulus intensity sensed by the individual; i.e., psychophysical technique, or stimulated adduction of the true vocal folds; i.e., laryngeal adductor reflex is determined. Conventionally, aryepiglottic fold is stimulated to evaluate sensory capacity of the laryngopharyngeal region. To date, laryngopharyngeal sensation is reported to be diminished in patients suffering from laryngopharyngeal reflux, dysphagia, aspiration, laryngomalacia, or apnea [2,3,4,5,6,7,8,9].
Patients with laryngopharyngeal reflux may present with laryngopharyngeal signs such as postcricoid edema or hypertrophy, erythema and/or edema of arytenoids, vocal fold, sulcus vocalis, or vocal cord nodules or polyps [10,11,12,13,14]. Given the variety of laryngeal signs in laryngopharyngeal reflux, we hypothesized that laryngopharyngeal sensory deficit in laryngopharyngeal reflux is not limited to aryepiglottic fold and involves the majority of laryngopharyngeal sites. The aim of the present study was to map mechanoreceptor response in various regions of the laryngopharynx in healthy individuals and patients with suspected laryngopharyngeal reflux.
Go to : 
MATERIALS AND METHODS
Five patients with suspected laryngopharyngeal reflux (2 men, 3 women; range, 30 to 57 years; mean±SD, 48±11 years) and six healthy volunteers (6 women; range, 23 to 43 years; mean±SD, 37±11 years) were studied. The Institutional Research Review Board approved the studies and participants gave written informed consent prior to the studies. Participants were recruited by advertisement and filled out a detailed health questionnaire before their studies. The subjects with a history of smoking, excessive alcohol intake, neurological abnormality, and aerodigestive tract disorder were ineligible.
Healthy volunteers had no esophageal or laryngeal symptoms. In addition, healthy volunteers did not exhibit any laryngeal and pharyngeal abnormality during the flexible fiberoptic laryngoscopy. Patients with suspected laryngopharyngeal reflux complained of the following symptoms: intermittent hoarseness, chronic hoarseness, frequent throat clearing, sore throat, or chronic cough. Reflux Symptom Index Score [15] abnormal, i.e, score >10, in four patients (range, 12 to 22) and 9 in one patient. Flexible fiberoptic laryngoscopy documented laryngitis in one of the five patients with laryngopharyngeal reflux. Laryngeal mechanoreceptor response was tested prior to acid suppressive treatment. After the testing, patients received proton pump inhibitor and all patients were asymptomatic after treatment.
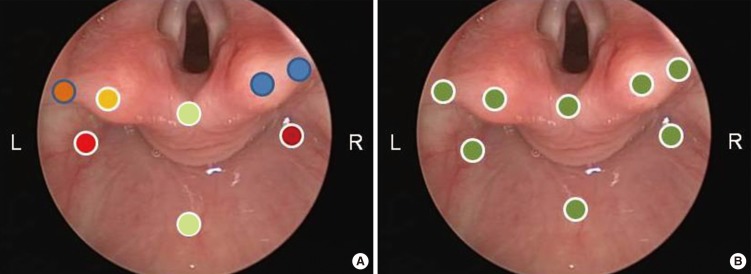
Mechanoreceptor response was assessed using an air pulse stimulus to evoke laryngopharyngeal sensation and the laryngeal adductor reflex. The flexible fiberoptic laryngoscope (FNL 10 AP Laryngoscope; Pentax Precision Instruments Co., Orangeburg, NY, USA) with a channel connected to a calibrated air pressure device (AP-4000 Air Pulse Sensory Stimulator; Pentax) was used to deliver an air pulse to evoke mechanoreceptor response in the posterior pharyngeal wall of the hypopharynx, interarytenoid area, bilateral arytenoids, bilateral aryepiglottic folds, and bilateral pyriform sinuses. With the participants sitting upright in a chair, the more patent side of the nasal cavity was anesthetized by passing a cotton tipped swab covered with 2% lidocaine gel. Then the laryngoscope was passed through the nose to the nasopharynx and pharynx until the laryngopharyngeal region was observed. Air pulse stimulation was delivered by advancing the tip of the laryngoscope to 2 mm of the target region. The duration of air pulse was 50 ms and the intensity of the air pulse increased in 0.5 mmHg increments starting from 2 mmHg to 10 mmHg until the participant felt the air pulse. The participants were instructed to raise the index finger when they felt the air pulse. The air pulse pressure resulting in reproducible response upon testing the target region three consecutive times was considered as the threshold stimulus to elicit mechanoreceptor response. Each stimulus was separated by 30-second resting period. The threshold stimulus evoking mechanoreceptor response was recorded as sensory threshold for each region.
During the delivery of stimulus, air pulse pressure inducing laryngeal adductor reflex was also noted for the regions of bilateral arytenoids, bilateral aryepiglottic folds, and interarytenoid region as observance of vocal fold adduction was feasible only for the arytenoids, aryepiglottic fold, and interarytenoid region. The air pulse pressure inducing reproducible laryngeal adductor reflex by stimulating the targeted regions three consecutive times was considered as the threshold stimulus to evoke the laryngeal adductor reflex. Each stimulus was separated by 30-second resting period and the threshold stimulus eliciting the laryngeal adductor reflex was recorded laryngeal adductor reflex threshold for each region.
The threshold air pulse pressure evoking laryngopharyngeal sensation or laryngeal adductor reflex was rated as normal for air pulse pressure less than 4 mmHg, moderate deficit for air pulse pressure ranging from 4.0 to 6 mmHg, or severe deficit for air pulse pressure more than 6 mmHg [2]. Statistical comparisons between groups were performed using parametric (student t-test) and nonparametric test (Mann-Whitney Rank Sum Test), as appropriate. A P-value less than 0.05 deemed statistically significant. Data are presented as mean±standard error.
Go to :
RESULTS
All patients tolerated the procedure and allowed stimulation of the targeted regions. Of the six healthy controls, two subjects could not allow stimulation of the interarytenoid region or the pyriform sinuses. In controls, an air pulse of 2 mmHg pressure evoked laryngopharyngeal sensation in all regions (Fig. 1), except bilateral aryepiglottic folds of one control requiring 4 mmHg and 8 mmHg. The sensory threshold was within normal limits in all regions except left aryepiglottic fold of one control.
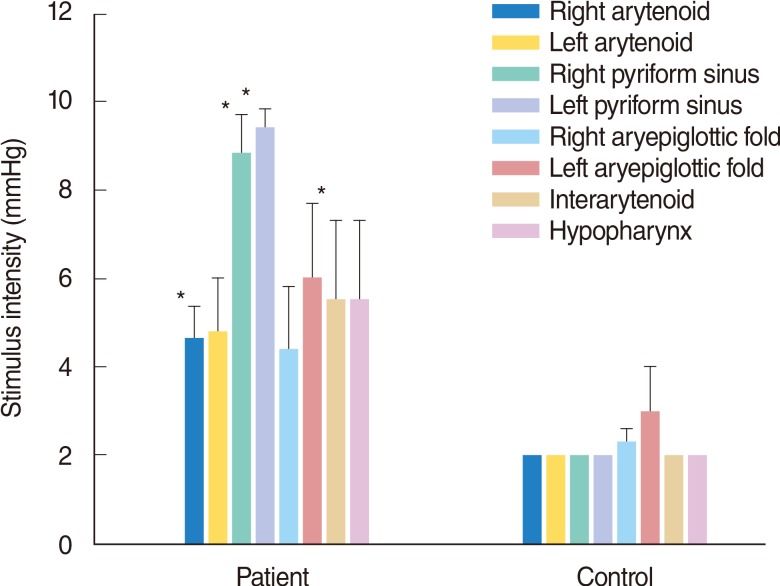 | Fig. 1Threshold stimulus intensity evoking sensation in patients and controls. Threshold stimulus intensity evoking sensation showed regional variation in the patient group. Although there is a trend for the patient group to have greater stimulus intensity to evoke sensation in the studied regions, these differences reached statistical significance in the right arytenoids (*P=0.03), right pyriform sinus (*P=0.004), left pyriform sinus (*P=0.004) and interarytenoid regions (*P=0.03) compared with the control group. Data presented as mean and standard error.
|
All patients reported sensation with air pulse intensities ranging from 2 mmHg to 8 mmHg in the arytenoids. Stimuli between 2 mmHg and 9.5 mmHg evoked sensation in the aryepiglottic folds. Two patients had no aryepiglottic fold response to stimuli delivered up to 10 mmHg. Of the 5 patients, one patient had sensation in response to stimulation of bilateral pyriform sinuses. Two patients had no sensation in pyriform sinuses in response to the stimuli reaching up to 10 mmHg. Two patients had unilateral pyriform sinus sensation in response to the threshold stimuli of 8 mmHg and 9 mmHg. Air pulse intensities ranging from 2 mmHg and 10 mmHg evoked sensation in the interarytenoid region and posterior pharyngeal wall in the hypopharynx. The threshold air pulse pressure resulting in laryngopharyngeal sensation varied between the right and left sides of the arytenoids, aryepiglottic fold and pyriform sinuses in the majority of the patients (Fig. 1).
The laryngeal adductor reflex was evoked by a 2 mmHg air pulse pressure in all controls, except one control who required the stimulus of 4 mmHg to the left aryepiglottic fold. The threshold stimulus to evoke laryngeal adductor reflex was within normal limits in all controls (Fig. 2). In patients, air pulse pressures ranging from 2 mmHg to 9.5 mmHg delivered to the arytenoids evoked the laryngeal adductor reflex. The air pulse pressure eliciting the laryngeal adductor reflex was same for the right and left arytenoids in three of the five patients. In three patients, the threshold air pulse pressure to evoke the laryngeal adductor reflex was within normal limits in arytenoids. Laryngeal adductor reflex was elicited by air pulse pressure ranging from 2 mmHg to 9.5 mmHg in nine of the ten aryepiglottic folds stimulated in five patients. In one patient, delivery of air pulse pressure of 10 mmHg to right aryepiglottic fold did not induce laryngeal adductor reflex. The air pulse pressure eliciting the laryngeal adductor reflex was same for the right and left aryepiglottic folds in three of the five patients. The threshold stimulus to evoke laryngeal adductor reflex was within normal limits in seven of the ten aryepiglottic folds. The laryngeal adductor reflex was evoked by delivering the stimuli ranged between 2 mmHg and 10 mmHg to the interarytenoid region. The threshold stimulus was within normal limits in four of the five patients.
 | Fig. 2Threshold stimulus intensity eliciting laryngeal adductor reflex in patients and controls. Threshold stimulus intensity evoking laryngeal adductor reflux showed regional variation in the patient group. Although there is a trend for the patient group to have greater stimulus intensity to evoke laryngeal adductor reflux sensation in the studied regions, these differences reached statistical significance in the right arytenoids (*P=0.03), compared with the control group. Data presented as mean and standard error.
|
In controls, the threshold stimulus to evoke laryngeal adductor reflex was same as the sensory threshold stimulus in all regions except aryepiglottic fold of one subject (Figs. 3, 4). In patients, the threshold stimulus eliciting laryngeal adductor reflex was not same as the sensory threshold stimulus in the majority of arytenoids and aryepiglottic folds (Figs. 3, 4). In the interarytenoid region, the threshold stimulus inducing laryngeal adductor reflex was same as the sensory threshold stimulus in four of the five patients.








In the patient group, the stimulus intensity eliciting sensation in the right arytenoid, bilateral pyriform sinuses, interarytenoid regions was higher than that of the control group (P<0.05) (Fig. 3). The stimulus intensity eliciting sensation in the left arytenoids, bilateral aryepiglottic fold and hypopharynx were no statistically different between patient and control groups (Fig. 4). In the patient group, the threshold stimulus to evoke laryngeal adductor reflux in the right arytenoid was greater than that of the control group (P<0.05) (Fig. 4).
Go to :
DISCUSSION
Laryngopharyngeal sensation has been increasingly studied to delineate the role of supraglottic sensory function in the pathogenesis of laryngopharyngeal reflux [3,4,6]. Patients with possible laryngopharyngeal reflux had a diminished laryngopharyngeal sensation as determined by the stimulation of the mucosa of aryepiglottic fold. In the light of a wide range of laryngeal signs associated with laryngopharyngeal reflux,, we investigated regional sensory function of the laryngopharyngeal structures in addition to commonly tested mucosa of the aryepiglottic fold.
Previous studies documented that stimulation of the aryepiglottic fold evokes sensation and triggers laryngeal adductor reflex [16]. In healthy normal subjects, the laryngopharyngeal sensation threshold is reported to be same as the stimulus threshold triggering the laryngeal adductor reflex [16]. Our findings documented that the threshold air pulse pressure eliciting sensation was same as the stimulus inducing laryngeal adductor reflex in five of the six normal healthy volunteers. The normal healthy volunteer who had dissimilar thresholds for sensation and laryngeal adductor reflex was the oldest volunteer in the healthy group. Plausibly, the observed dissimilarity is a reflection of aging associated changes in the laryngopharyngeal sensorimotor function. Nevertheless, the threshold stimuli eliciting sensation and laryngeal adductor reflex were within normal limits except left aryepiglottic fold of one volunteer. The present study also documented mechanoreceptor response in the arytenoids, interarytenoid region, posterior pharyngeal wall of the hypopharynx, and pyriform sinus. Stimulation of the targeted regions by delivering 2 mmHg air pulse elicited sensation and laryngeal adductor reflex in all normal healthy controls. The range of normal values of sensory discrimination threshold in the laryngopharyngeal structures other than the aryepiglottic fold has not been determined. Present study findings provide preliminary evidence that the normal sensation values established for the aryepiglottic fold may be applied for the rest of the laryngopharyngeal structures. However, previously described variances in distribution and density of sensory nerve fibers in the laryngopharyngeal region may cause differences in the regional sensorimotor response among the laryngopharyngeal structures [17]. Establishment of normative values for various structures in the laryngopharyngeal region in a larger group of normal healthy subjects is needed to better assess the integrity of laryngopharyngeal sensation in healthy and diseased individuals.
In the present study, stimulation of mechanoreceptors in various structures of the laryngopharyngeal region revealed inter- and intra-subject differences in the regional laryngopharyngeal sensation in patients with suspected laryngopharyngeal reflux. In contrast to healthy volunteers, patients with laryngopharyngeal reflux did not exhibit a uniform threshold stimulus for eliciting sensation or laryngeal adductor reflex among the studied laryngopharyngeal structures. Using the previously reported normal sensory threshold range, we identified sensory deficit in 20 of the 30 stimulated sites. These findings support our hypothesis that laryngopharyngeal sensory deficit in laryngopharyngeal reflux is not limited to the aryepiglottic fold and involves the majority of laryngopharyngeal sites. Indeed a sensory deficit of >5 mmHg air pulse pressure in the interarytenoid region is reported to be 90% sensitive and 90% specific as a diagnostic indicator of reflux disease [18].
The laryngeal sensory deficit in patients with laryngopharyngeal reflux potentially impacts the integrity of laryngo-upper esophageal sphincter contractile reflex defined as contraction of upper esophageal sphincter in response to laryngeal stimulation [19,20]. The elicitation of the laryngo-upper esophageal sphincter contractile reflex deteriorated with age [21]. Patients with dysphagia had decreased frequency of triggering of the laryngo-upper esophageal sphincter contractile reflex [20]. Plausibly, the laryngo-upper esophageal sphincter contractile reflex may stop laryngopharyngeal reflux by preventing further entry of reflux material in the regions above upper esophageal sphincter when the upper esophageal sphincter contracts in response to reflux bolus contacting the laryngeal structures. To date, integrity of the laryngo-upper esophageal sphincter reflex in patients with laryngopharyngeal reflux has not been evaluated.
In conclusion, air pulse stimulation of mechanoreceptors in the laryngopharyngeal structures including the arytenoid, interarytenoid, aryepiglottic fold, and pyriform sinus evoked sensation and laryngeal adductor reflex in healthy volunteers and patients with laryngopharyngeal reflux. Healthy volunteers exhibited identical threshold stimulus for sensation and laryngeal adductor reflex among the stimulated sites. The threshold stimuli to evoke sensation or laryngeal adductor reflex were heterogeneous among the stimulation sites in patients with laryngopharyngeal reflux. Further studies are needed to establish the normative data for sensory function of the laryngopharyngeal structures, and to determine the sensitivity, specificity, positive predictive value and negative predictive value of sensory testing of the laryngopharyngeal structures as a diagnostic indicator of laryngopharyngeal reflux.
Go to :
 XML Download
XML Download