

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Allergic rhinitis (AR) is a globally increasing health problem affecting roughly about 500 million patients worldwide [1]. The annual costs of AR nearly range from US$ 2-5 billion according to 2003 values [2]. It affects the quality of life and represents a major cause of morbidity [3]. AR is a chronic disease showing symptoms of nasal congestion, nasal itching, rhinorrhea and sneezing [4]. The management of the disease depends mainly on the avoidance of exposure to antigens-which is not usually feasible-and symptomatic pharmacological treatment including antihistamines and topical corticosteroid.
One of the available causal treatments is allergen immunotherapy which is effective after the end of the treatment course, unlike symptomatic drugs. Specific immunotherapy (SIT) modifies the basic allergic mechanism of the disease by inducing desensitization through gradually increasing the dose of the specific allergen over an optimum long period [3].
Over one hundred years, Leonard Noon in 1911 began to study subcutaneous immunotherapy (SCIT) in the treatment of AR [5]. In 1986, the British Committee for Safety of Medicines reported 26 deaths connected with SCIT, so multiple methods of delivery have been developed such as oral, nasal, bronchial and sublingual routes [6].
The first randomized controlled trial (RCT) worked on sublingual immunotherapy (SLIT) dates back to 1986 [4]. A panel of experts from the World Health Organization (WHO) and various allergy and immunology societies concluded in 1998 that SLIT was a viable alternative to the injection route [1]. In 2010, SLIT was included in the latest update of Allergic Rhinitis and its Impact on Asthma (ARIA) guideline for both adults and children [7].
ARIA 2008 suggested 4 main indications for SLIT: (1) patients with seasonal rhinitis "sensitive to pollens" or perennial rhinitis "sensitive to house mite"; (2) patients uncontrolled by pharmacological treatment; (3) patients presented by systemic reactions from the drugs; and (4) patients with poor compliance or refusing injections [8].
Mechanisms of SIT are not well identified till now. The most accepted theory is that SIT shifts the immune response from Th2 to Th1 through stimulation of the T-regulatory cell, which secretes interleukin (IL) and transforming growth factor (TGF)-β [9]. These T-regulatory cells with its mediators help to shift the immune response from the IgE to IgG. The IgG antibody especially IgG4 is considered as a blocking antibody which is known to interrupt the inflammatory cascade and stop the inflammatory mechanism initiated by the IgE release [10].
Today, SLIT is widely used in clinical practice, especially in European countries, since it is noninvasive, has minimal side-effects and can be easily administered at home. There are still some risks of adverse effects that range from mild local reactions like itching and swelling of the oral mucosa to severe systemic manifestation like anaphylaxis [11].
We aim to discuss SLIT in the treatment of AR, with a particular focus on efficacy, safety profile, patient adherence and the guidelines developed.
Go to : 
EFFICACY OF SLIT
Evaluation of the clinical efficacy of SIT in AR depends mainly on the assessment of reduction in symptoms severity and medication use [11]. There is an increasing number of RCTs done in this field over the last decades. The results of those RCTs were pooled on six meta-analyses for SLIT [3,12,13,14,15,16] and one meta-analysis for SCIT [17]. Meta-analysis, which is the statistical method pooling the results of different independent studies to provide a quantitative estimate of treatment, is considered the most robust proof of the efficacy of a treatment/intervention. The higher grade "A" recommendations is usually derived from meta-analyses [18,19].
SIT meta-analyses
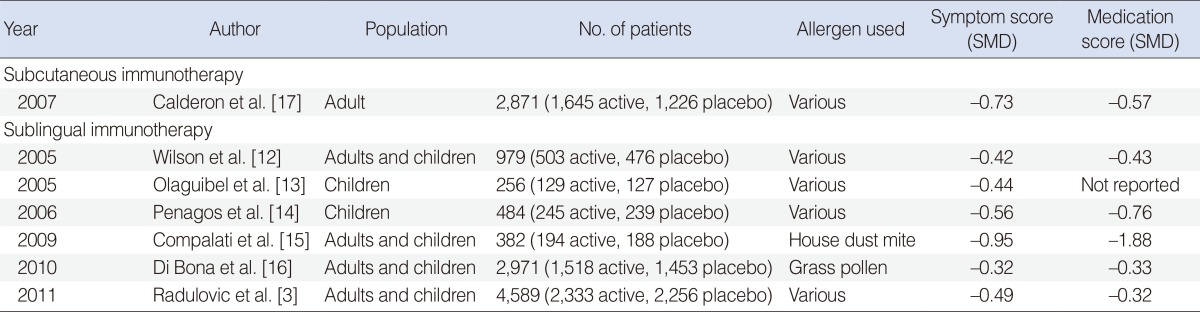
The only available SCIT meta-analysis in AR was done by Calderon et al. [17] in 2007 and was published under the frame of the Cochrane Collaboration. It examined 51 RCTs published between 1984 and 2006 with a total number of 2,871 patients (1,645 active, 1,226 placebo). None of these studies were done exclusively in children, but nine studies included participants younger than 18 years. A wide range of allergens was administered in these studies: 12 trials ragweed, 16 trials mixed grass, 5 trials timothy, 6 trials Parietaria, 4 trials birch, 3 trials cedar, 2 trials orchard, one each for bermuda, Juniperusashei, and Cocosnucifera. There was an overall significant reduction in symptom score from 15 trials with standardized mean difference (SMD) corresponding to -0.73 and to -0.57 in medication score data from 13 trials in immunotherapy treated group [17].
The SLIT meta-analyses started in 2005 when Wilson et al. [12] published a Cochrane review by working on 22 RCTs with five only in children and the total number was 979 patients (503 active, 476 placebo). This review was updated in 2011 by Radulovic et al. [3] who worked on 60 RCTs with 49 were suitable for pooling in meta-analysis with a total number of 4,589 patients (2,333 active and 2,256 placebo). There were 34 studies done in adults and 15 in children using a wide range of allergens including grass pollen in 23 trials, Parietaria in 5 trials, ragweed in 2 trials, trees in 9 trials, olive in 2 trials, cypress in 3 trials, birch pollen in 2 trials, mixed trees in 2 trials, house dust mite in 8 trials and cat in one trial. The overall results were significant in the reduction of symptoms (SMD, -0.49; P<0.001) and medication use (SMD, -0.32; P<0.001) compared with placebo. The subgroup analyses showed that SLIT is highly effective in both seasonal however perennial AR. Also, the study was not able to identify a significant reduction in either symptoms or medication scores in children [3].
There are two meta-analyses which worked only on children. The first was done in 2005 by Olaguibel et al. [13] who worked on 7 RCTs with a total population of 256 (129 active, 127 placebo) including house dust mite in 3 trials, one trial each for grass mixed, olive and Parietariain. The results showed that there was no significant effect on nasal (SMD, -0.44; P=0.27) and eye symptoms (SMD, -0.49; P=0.19) but there was a significantly effective reduction of asthma symptoms (SMD, -1.42; P=0.01) and drug consumption (SMD, -1.01; P=0.06) [13]. In 2006, Penagos et al. [14] worked on 10 RCTs with 484 pediatric patients aged from 3 to 18 years (245 active, 239 placebo). Allergens included were mites in 4 trials, grass mix in 3 trials, one trial each for olive, Parietaria, and Phleumpoa. The study showed a significant reduction of both symptoms (SMD, -0.56; P=0.02) and medication score (SMD, -0.76; P=0.03). The subgroup analyses showed that high efficacy was obtained in duration longer than 18 months and for pollen allergens compared with house dust mites [14].
According to allergen used, two meta-analyses limited their inclusion to one type of allergen. The first one was in 2009 when Compalati et al. [15] worked on 8 RCTs for house dust mite-induced AR in adult and children, including 382 (194 active and 188 placebo) and the results showed significant reduction in symptoms (SMD, -0.95; P=0.02). The medication score was (SMD, -1.88; P=0.04) in 89 patients [15]. Another one by Di Bona et al. [16] in 2010 worked on 22 SLIT RCTs conducted with grass pollen extracts in adult and children with a total number of 2,971 (1,518 active and 1,453 placebo) and found a significant reduction in both symptoms (SMD, -0.32) and medication use (SMD, -0.33). The authors concluded that adult treatment seems to be more effective that children [16] (Table 1).
There is an obvious limitation of included meta-analyses which is the heterogeneity in data. The results of meta-analyses were affected with different dosages, types of pollen, standardization methods, treatment schedules and patient populations [11]. Nieto et al. [20] concluded in his paper about the quality of SLIT meta-analyses that the meta-analyses showed "discrepancies, inconsistencies, and lack of robustness and do not provide enough evidence" for the current routine use of SLIT. These heterogeneities make the interpretation of results difficult especially when you extend the results to all patients, allergens, and AR vs. asthma [21]. There is a possible solution to overcome the problem of heterogeneity by making single multi-centric study of a large number of patients. This will allow adequate statistical power [11].
Type of allergen and doses of SLIT
The type of allergen used and its relation to efficacy is still controversial. In the United States, multi-allergen extracts are preferred to address all major sensitivities. In Europe, allergists are against this practice as they think, it may lead to dilution effect and degradation of proteolytic activity decreasing effective dose given to patients [21]. The studies published on the option of using multi-allergen SLIT are few [22,23,24] and there aren't enough data available on both efficacy and induction of immunological tolerance for either mixture or simultaneous application of various allergens. So, large studies are needed to evaluate and validate multi-allergen SLIT especially in polysensitized patients as the majority of the patients are polysensitized [25].
SLIT efficacy is suggested to be dose-dependent. The ARIA initially informed that doses-at least 50 to 100 times higher than those administered with SCIT by the same extracts-are needed for treatment success [8]. World Allergy Organization updated that a dose of about 600 mg of the major allergens every month was suggested as an optimal dose for patients with grass-induced seasonal rhinitis [26]. Di Bona et al. [16] in his meta-analysis concluded that a monthly dose of major allergens showed that the SMD of symptom scores was -0.47 in patients receiving doses from 276 to 600 mg compared with -0.16 in patients treated with a monthly dose up to 275 mg. However, more studies are still needed to determine the optimum doses and schedules.
Long-lasting and the preventive actions
The long-lasting effect and the preventive actions after discontinuation of SIT are other unique advantages beside its efficacy. These effects are due to complex, profound and persistent modifications in the immune response to allergens [27]. There is a study showed greater improvement in 70 patients with dust mites AR treated with SLIT in 3 years compared with 67 patients treated for 2 years [28]. In another prospective open controlled study, 4 groups of mono-sensitized patients to mites received drug treatment only and another 3 groups received SLIT for 3, 4, or 5 years and all groups were observed for 15 years. The clinical scores showed that the clinical benefit continued for 7 years in patients treated for 3 years, while it continued for 8 years in those treated for 4-5 years [29].
Concerning the preventive action, Marogna et al. [30], in their open randomized control study in children working with 144 patients showed that SLIT has the potential to decrease the incidence of new sensitizations. The results of the study were 3.1% in SLIT-treated patients versus 34.8% (P=0.01) in the control for 3 years follow-up.
Go to :
SAFETY OF SLIT
Most of the systematic reviews and meta-analyses met on that SLIT is safer than SCIT. Although SCIT has proved its efficacy in AR, the risk of systemic adverse effects and anaphylaxis-which may occur with all types of allergen preparations either standardized extracts, allergoids, or recombinant allergens-make it less favorable [31]. In the only available meta-analyses on SCIT for seasonal AR, 8% and 7% of patients in the treated groups experienced grades II and III systemic reactions respectively by using the European Academy of Allergy and Clinical Immunology classification for adverse events. Anaphylaxis (grade IV) was reported in 3 cases in the SCIT group (0.72%) versus 1 case in the placebo group (0.33%). This meta-analysis showed that epinephrine was used in 3.4% of treated group versus 0.25% in the placebo group but no fatalities were reported [17].
Concerning SLIT safety, there is some heterogeneity in the results recorded but the adverse effects ranged from minor local effects in the mouth and gastrointestinal reactions (diarrhea and vomiting) to systemic reactions like anaphylaxis with no deaths. In the first meta-analysis by Wilson et al. [12] in 2005 who worked on 22 RCTs and found that "there is no systemic reaction but some minor local reaction like itching and swelling of the oral mucosa were reported almost universally but were rarely of significance." Olaguibel et al. [13] worked on 7 RCTs with a total population of 256 and found that there were no severe or systemic reactions, but oral and gastrointestinal symptoms were the most common adverse effects. In the most recent meta-analysis in 2011, Radulovic et al. [3] suggested a remarkably safe profile without any severe systemic reactions, anaphylaxis or use of adrenaline in 49 studies. Also, Radulovic et al. [3] found that local reactions are common, unavoidable, have less distress, have no lasting effect and don't need the withdrawal of treatment. To our knowledge, there are only 11 cases of SLIT anaphylaxis. In some of them, the allergen used was mixture of multiple unrelated non-standardized extracts. But also, there were patients who expressed a severe reaction after the first dose of a grass tablet [32,33,34,35,36,37].
The safety of SLIT in children was evaluated in some studies suggesting that it is safe in children younger than 5 years. One study worked with 65 children aged from 3 to 7 years old and showed that high dose immunotherapy didn't increase the adverse effects including urticaria, gastrointestinal problem and oral pruritus in children less than 5 years in comparison with children aged from 5 to 7 [38]. Another study confirmed the safety of SLIT in children less than 5 years by working with 126 children aged from 3 to 5 years. The study showed that only nine adverse effects were reported in seven patients, corresponding to 5.6% of patients. Two of the nine were local oral itching which were mild and transient and did require neither dose adjustment nor medical intervention. The other seven adverse effects involved the gastrointestinal tract in the form of abdominal pain which was mild. In six cases, the pain was associated with diarrhea [39].
In the aspect of the relation between types of allergen used and safety, a study showed the same risk of adverse effect in multiple allergens compared with mono-allergen SLIT. It worked with 433 pediatric patients and concluded that the use of multiple allergens for SLIT does not increase the rate of adverse effects in children [40]. We think that more studies are needed to assess the safety according to standardized classification and reporting methods of adverse events associated with SLIT around the world.
Go to :
ADHERENCE
It is common that the term adherence and compliance are used interchangeably but actually there is some difference. Adherence is defined as "the extent to which a person's behavior, taking medication, following a diet and/or executing lifestyle changes corresponds to the recommendations agreed with a healthcare provider" [41]. This term became more globally used and more specified than compliance which is defined as "the extent to which a person corresponds to the physician's prescription" [42].
Non-adherence to the therapy or lifestyle modification is the greatest problem of medical practice in chronic diseases. This point derived WHO-in its report in 2003 on the importance of medication adherence-to use Haynes's quotation; "Increasing the effectiveness of adherence to interventions may have a far greater impact on the health of the population than any improvement in specific medical treatments" [43].
In general, the causes of non-adherence may be related to the patient himself, the disease, treatment or the health care system (Table 2) [44].
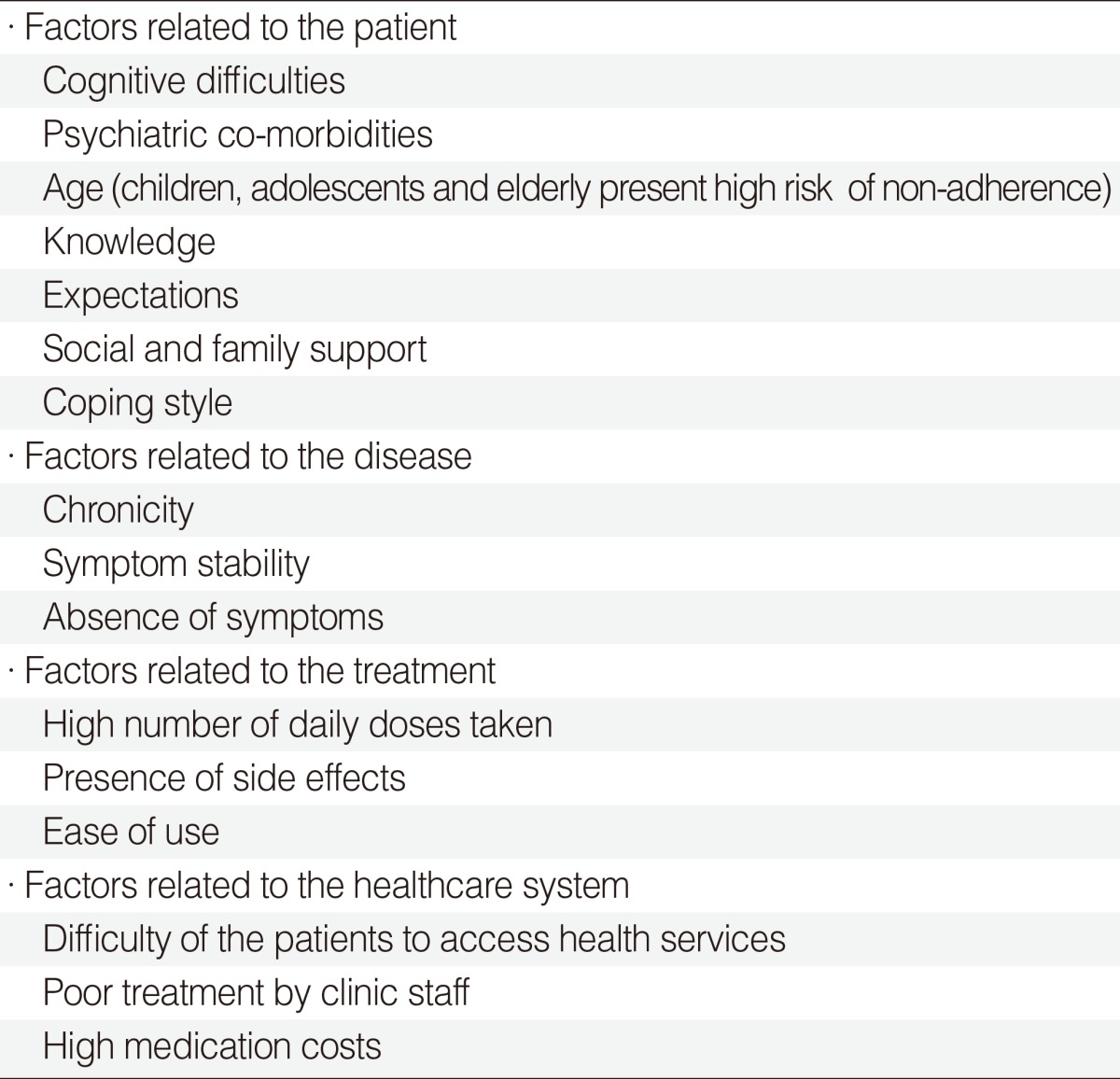
Table 2
Causes of non-adherence to treatment
Reprinted from Passalacqua et al. [44] with permission of John Wiley and Sons.
![]()
Although, SIT changes the immunological basis of the disease and decreases the times of use of symptomatic treatment, but the patient will need to adhere to the treatment for a few years. So, SIT adherence is considered one of the most critical problems affecting completion of therapy.
There are nearly few studies which assessed the adherence of the immunotherapy, so it wasn't discussed in details in the meta-analyses. In comparison of adherence to SLIT with SCIT, the adherence rate in SLIT ranged from 75% to more than 95% in 6 RCTs [45,46,47,48,49,50]. It was favorable than that of SCIT which ranged from 33% to 89% in 8 RCTs [47,51,52,53,54,55,56,57]. This is mainly due to the inconvenience of SCIT; as patients need to go for the injection in the physician's office in contrast to SLIT doses which are taken at home [58]. Despite that, SLIT still has moderate results in adherence because patients take drugs by themselves or parents [59] (Table 3).

In a recent Italian study by Senna et al. [60] in 2010 conducted on sales data provided by two major manufacturers, more than 50% of patients discontinued SLIT during the first year. In the second year, only 28% remained on the treatment which became 13% in the third year. Senna et al. [60] referred this high drop-out rate mainly to the costs and modality of reimbursement. He informed that the regimen of administration or doses didn't seem to play a relevant role in the discontinuation rate.
The solutions to improve the adherence and reduce drop-out rates are to develop more convenient allergen formula and schedules [59]. Also, receiving detailed information on special educational programs to the patient seems to be helpful in increasing adherence. The not well-trained patient will lead to trivial side-effects to SLIT such as oral and gastrointestinal local reactions, and this will lead to sudden withdrawal of the treatment [61].
In a trial to know the causes of non-adherence, a survey conducted between the specialists who routinely prescribed SLIT, reported that the absence of the perceived efficacy is the most frequent causes for withdrawing followed by cost and tolerability. The side effects, patient education and ease of use were judged to be of low importance [62]. What makes this study of a low importance is that the data were obtained from the doctors not from the patient, who are the main protagonists of the compliance scenario [44]. We suggest that more studies discussing adherence are needed to assess and determine the main limitations in patient adherence to treatment.
Go to :
SLIT GUIDELINES
Clinical practice guidelines for the management of AR had been developed over the past 15 years and proved its efficacy in improving the medical care [63]. SIT was firstly introduced and discussed in January 1997-in Geneva, Switzerland-in a meeting between experts from WHO and many other allergic societies in a trial to produce guidelines for allergen immunotherapy [1]. After one year in 1998, the editors and participating members reached a consensus about the information to be published under the title "Allergen immunotherapy: therapeutic vaccines for allergic diseases. WHO position paper." They informed that SCIT is effective in alleviating symptoms and modifying the basic allergic mechanisms of the disease but there were sever adverse effects reported like anaphylaxis and other systemic reactions. That derived the experts to search for other safe routs like sublingual swallow, oral immunotherapy or bronchial routs. They suggested that SLIT is a good available alternative route to SCIT but it is not recommended and well-designed studies were needed to prove its efficacy [1].
In 1999, during the ARIA WHO workshop, a panel of experts provided suggestions that were published in 2001 [64] under the title of "Allergic Rhinitis and its Impact on Asthma (ARIA) guideline." This was considered the first in the field of guidelines for AR. The ARIA guideline was innovative in many items like proposing a new AR classification into "intermittent" or "persistent" according to persistence and severity of symptoms and the co-morbidities between upper and lower airways disease. Regarding SIT, the ARIA recommended the use of SLIT for adult and children complaining from seasonal AR and for adult with perennial AR. But, there was no recommendation for children with perennial AR [64]. After 7 years, in 2008, the ARIA group made a major revision to cover the growing up knowledge in AR in collaboration with Global Allergy and Asthma European Network (GA2LEN) and AllerGen NCE. This update recommended SLIT in the treatment of pollen allergy in adult and not recommended but "may be used" in patients with mite allergy [8].
In the World Allergy Organization position paper in 2009, SLIT was recommended as an effective treatment for AR. The paper informed that SLIT is effective in children ≥5 years of age and it may be safe in children ≥3 years of age. It also informed that SLIT can be used for AR in children with asthma. In this paper, comparison between SLIT and SCIT was made. It concluded that SLIT is well tolerated and safer than SCIT. All adverse effects of SLIT occur during the first dose and the majority of them are local. Only few cases of SLIT-related anaphylaxis have been reported with no fatalities. The experts confirmed at the point that the patient must be well informed about adverse effects, how to deal with them and when to seek medical advice especially as the doses will be administered at home [26].
On July 2010, GA2LEN/European Academy of Allergology and Clinical Immunology (EAACI) pocket guide for SIT for AR and asthma answered the question "which route of administration is preferable SLIT or SCIT?" by informing that there are many independent studies comparing SLIT with SCIT concluded that there was no difference in efficacy. No fatality and only few severe adverse events have been reported with SLIT but many local adverse effects were recorded. Regarding the final choice between SLIT and SCIT, the guide suggested making the decision individually with each patient after many considerations such as home based treatment vs. doctor visit, fear of injection, costs and compliance. Concerning the point of age, the guide concluded that many studies suggested the age to be more than 5 years to be safer and more effective and for old age there is no upper limit [65].
In December 2010, American Academy of Allergy, Asthma & Immunology (AAAAI), American College of Allergy, Asthma & Immunology (ACAAI) and Joint Council of Allergy, Asthma & Immunology (JCAAI) concluded that SLIT reduces symptoms but require higher doses than that of subcutaneous route with frequent local and gastrointestinal adverse effects. But, currently there is no Food and Drug Administration (FDA)-approved formulation for a non-injection immunotherapy extracts [66].
All these guidelines and recommendations used evidence-based approaches but none of them used Grading of Recommendation, Assessment, Development and Evaluation (GRADE) system [67,68,69]. This system grades recommendations on two levels: strong and weak (alternative term is conditional) and quantifies evidence into four categories: high (in symbolic language four plus), moderate (three plus), low (two plus), and very low (one plus) [67].
In 2010, a panel of ARIA and GA2LEN experts formulated 42 questions about prevention, management of AR and the relation between AR and asthma in the same patient. Then, methodologists developed 48 questions based on patient-intervention-comparison-outcome (PICO) style and evidence based answer was prepared for each question using the GRADE approach. This made ARIA 2010 update more understood and accepted from the health care provider [69]. SLIT in ARIA 2010 update was recommended for adult with AR due to pollen (with weak recommendation and moderate quality of evidence) or house dust mites (weak recommendation and low quality of evidence). This recommendation is due to the high value in alleviating the symptoms and relatively low value on avoiding adverse effects and costs. In children with AR due to pollen, SLIT is recommended with weak recommendation and moderate quality of evidence. But, in children sensitive to mites, it suggested not to administer SLIT outside highly prepared clinics (weak recommendation and low quality of evidence) [7] (Table 4).
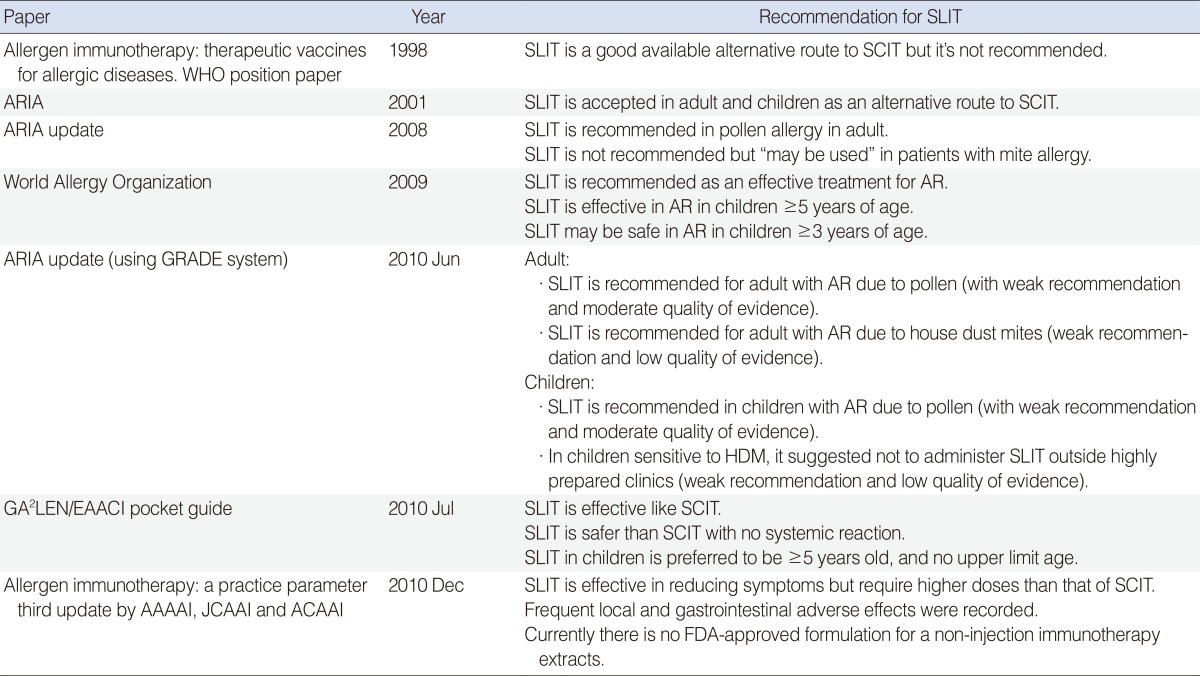
Table 4
Chronological presentation of SLIT recommendations
SLIT, sublingual immunotherapy; WHO, World Health Organization; SCIT, subcutaneous immunotherapy; ARIA, Allergic Rhinitis and its Impact on Asthma; AR, allergic rhinitis; GRADE, Grading of Recommendation, Assessment, Development and Evaluation; GA2LEN, Global Allergy and Asthma European Network; EAACI, European Academy of Allergology and Clinical Immunology; AAAAI, American Academy of Allergy, Asthma & Immunology; JCAAI, Joint Council of Allergy, Asthma & Immunology; ACAAI, American College of Allergy, Asthma & Immunology; FDA, Food and Drug Administration.
![]()
Implementation of these guidelines and re-evaluation is very important. Derivative of guidelines such as pocket guides, web-based activities, questionnaires and web-based documents must be disseminated internationally. The 2008 ARIA update was translated into more than 50 languages, and there was a plan to disseminate 2010 update internationally [69]. Specialists and primary care physicians should be encouraged to use these guidelines and its derivatives and should be involved in their production.
Go to :
CONCLUSION
SLIT has been established as evidence-based treatment for AR. SLIT was introduced in latest update of ARIA guidelines in 2010 with weak recommendation and moderate quality of evidence for patient sensitive to pollen and low quality of evidence for house dust mite according to the GRADE system. Beside its efficacy in reducing the symptoms and medication scores recorded in meta-analyses, the unique advantages of long-lasting and preventive actions are due to profound and persistent modifications in the immune system. Also, the safety of SLIT was found to be more favorable than SCIT. The most common recorded adverse effects were minor local effects in the mouth, gastrointestinal reactions and rare anaphylaxis with no fatality. In children, many of guidelines and recommendations suggested not to start SLIT in children ≤5 years due to lack of safety evidence. Adherence to treatment was found to be more better for SLIT with less drop-out rates than SCIT mainly due to its safety, noninvasiveness and easy administration at home. We support the call to conduct large multi-centric studies to gain more statistical power and overcome the problem of heterogeneity observed in the meta-analyses. Also, retrospective studies are needed to record causes of drop-out rates in the real life.
Go to :
 XML Download
XML Download