

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Sjögren's syndrome is a chronic inflammatory autoimmune disease. Its clinical characteristics are dry eyes (keratoconjunctivitis sicca) and dry mouth (xerostomia) and its histological characteristic is lymphocytic infiltration and destruction of the salivary and lacrimal glands [1]. Labial minor salivary gland biopsy is used as a part of the diagnostic workup for suspected Sjögren's syndrome. The focus score in minor salivary gland biopsy is one of the revised classification criteria for Sjögren's syndrome proposed by the multicenter European study [2]. Among the techniques used to obtain the labial minor salivary gland, the most widely used method is conventional incisional lip biopsy [3]. This technique, however, is time consuming and requiring surgical instruments and assistance to be performed. The biopsy using a minimal incision with a needle tip of the labial minor salivary gland is a new technique that can easily be done as an office procedure causing minimal discomfort to the patients.
This study is to compare the usefulness and complications of biopsy using a minimal incision with a needle tip with those of conventional incisional lip biopsy in the diagnosis of Sjögren's syndrome.
Go to : 
MATERIALS AND METHODS
A retrospective chart review of all patients requested for the minor salivary gland biopsy for the diagnosis of Sjögren's syndrome at the tertiary hospitals from January 2005 to December 2008 was performed. One hundred forty-three patients were enrolled and they were 116 females (81.1%) and 27 males (18.9%).
Patients were divided into two groups depending on the biopsy techniques as the biopsy using a minimal incision with a needle tip and the conventional incisional lip biopsy. The existence and numbers of the minor salivary gland obtained and complications of the two techniques were assessed. The adequacy of the specimen is defined as the existence of at least one salivary gland tissue adequate for the diagnosis. This study protocol was approved by Institutional Review Board of Seoul National University Hospital.
Procedure technique
All the labial salivary gland specimens were obtained from normal-appearing mucosa in the lower lip between the midline and the commissure. The normal appearance is important because mucosal inflammation could result in inflammatory cell infiltration of submucosal salivary glands. In the biopsy using a minimal incision with a needle tip group, the lower lip was everted by the patient, and local anesthesia was administered with local infiltration of 2% lidocaine with epinephrine (at 1:100,000 dilution). A 5 mm-sized vertical incision was made on the mucosa with a needle tip (21-22 Gauge). The depth of the incision was 2-3 mm. The salivary glands are then released from the surrounding tissue by a sharp dissection using the needle tip. When a gland was taken out, it was grasped with small forceps gently and separated from the bed with the sharp edge of the needle tip. The small incision wound did not need to be reapposed (Fig. 1).

In the conventional incisional lip biopsy group, a 5×10 mm sized elliptical incision was made at the lower lip mucosa around the midline after local anesthesia. The mucosa and the underlying tissues, down to the muscle layer, were taken out with the scalpel or scissors. When the tissues were taken out, the presence of the salivary gland tissues was not evaluated routinely at the time of biopsy. The mucosal wound was sutured with an absorbable suture.
Safety assessment
Complications were investigated immediately after the procedure and postoperative 7 days based on objective sings through the physical examination and subjective symptoms through open-type questions.
Statistical analysis
In the present study, statistical analyses were performed using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). Patients were divided into two groups depending on the biopsy techniques as the biopsy using a minimal incision with a needle tip and the conventional incisional lip biopsy. Success rates were compared using a chi-square test. The numbers of salivary glands obtained were compared using t-test. Statistical significance was set at P<0.05.
Go to :
RESULTS
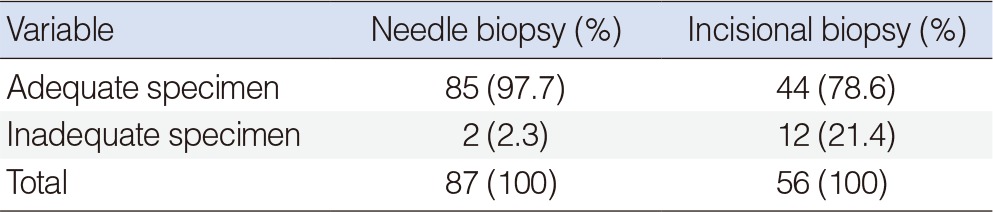
Out of 143 patients, 56 patients underwent the conventional incisional lip biopsy and 87 patients received the biopsy using a minimal incision with a needle tip. In the biopsy using a minimal incision with a needle tip group, adequate salivary gland samples were obtained from 85 patients out of 87 patients (97.7%). In the conventional incisional lip biopsy group, adequate specimens were acquired from 44 patients out of 56 patients (78.6%). The success rate to obtain adequate biopsy specimens was significantly higher in the biopsy using a minimal incision with a needle tip group than in the conventional incisional lip biopsy group (P<0.0001) (Table 1). In the patients with adequate specimens, the numbers of obtained salivary glands were not different among two groups (needle tip biopsy 1.78 vs. incisional lip biopsy 1.43, P=0.111). There was no complication in the patients after the biopsy using a minimal incision with a needle tip. In the conventional incisional lip group, one patient complained transient numbness of the lip.
Go to :
DISCUSSION
The biopsy using a minimal incision with a needle tip of the minor salivary gland is a new less invasive technique targeting the gland itself directly. It was easy to perform and safe. In this study, we had a better result with this technique than with the conventional one in term of the adequate specimen in the diagnosis of Sjögren's syndrome.
There is yet no definite or simple diagnostic test for Sjogren's syndrome [4]. According to the European criteria proposed in 1993, diagnosis requires 6 items, which are ocular symptoms, oral symptoms, evidence of keratoconjunctivitis sicca, focal sialadenitis by minor salivary gland involvement, instrumental evidence of salivary gland involvement, and presence of autoantibodies [2]. After that, a new set of classification criteria in a joint effort by the American and European Consensus Group was proposed [5]. The main change is that a positive Ro/La serology and histopathology is compulsory for the diagnosis. A minor salivary gland biopsy with a focus score ≥1 is a positive histopathology for the criteria. A focus is defined as an agglomerate of at least 50 mononuclear cells; the focus score is defined by the number of foci in 4 mm2 of glandular tissues [6].
The technique for minor salivary gland biopsy was first introduced in 1966 [7,8]. It made an elliptical incision of oral mucous membrane down to the muscle layer [9]. After that, many modifications in a type or length of incision were reported [3,4,10,11,12,13,14,15,16,17,18,19,20,21,22]. The minor salivary gland punch biopsy was introduced in 2001 [17]. Although many techniques were introduced as substitutions for the conventional incisional lip biopsy, it is still generally used because of not being too difficult to perform and not making significant problems [3].
In this study, we introduced a less invasive biopsy technique with a needle tip. No special equipments but a needle, forceps and gauzes were required for this simple procedure. Complete wound healing can be achieved in 5 days even without the wound closure with sutures. Since this technique is a targeted procedure to the salivary glands, it is helpful to harvest salivary gland tissues selectively without surrounding tissues those are not necessary for the diagnosis. On the contrary, the specimen after the conventional incisional lip biopsy contains surrounding soft tissues those are not necessary for the diagnosis (Fig. 2).
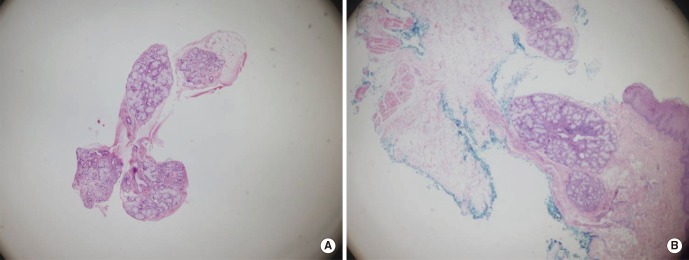 | Fig. 2Microscopic findings of the specimens from the two techniques (H&E, ×40). The specimen (A) from the biopsy using a minimal incision with a needle tip shows highly selective salivary gland tissues. The specimen (B) from the conventional incisional lip biopsy contains not only salivary glands but also epithelium, fatty tissues and muscles.
|
In conclusion, the less invasive labial minor salivary gland biopsy using a minimal incision with a needle tip was easy to perform and safe and showed the better result than the conventional incisional lip biopsy in terms of the adequate specimen in the diagnosis of Sjögren's syndrome. So it might be a good alternative to the conventional incisional lip biopsy.
Go to :

 XML Download
XML Download