

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Asian ginseng (Panax ginseng) and its unique constituents of saponin glycosides called ginsenosides has been the subject of many experimental and clinical researches to reveal the diverse biological properties in humans, such as immunostimulatory, anti-tumor, hypolipidemic, hypoglycemic, hypotensive, antithrombotic, anti-inflammatory, anti-oxidative, antimicrobial, sexual arousal, and skin photoprotective effects. Red ginseng represents one of the commercially available forms of the P. ginseng root, which is steamed and dried for the preservation and production of therapeutic components.
It was reported that Korean red ginseng (KRG) has protective effects on ototoxicity [1,2,3] and cochlear ischemia [4] by acting as an antioxidant. In addition, KRG was known to have a potent antithrombotic, anti-platelet activity to prevent vascular occlusion [5,6]. However, there have been few studies about the therapeutic effects of KRG on idiopathic sudden sensorineural hearing loss (SSNHL), of which the incidence is increasing in the general population.
Systemic steroid therapy in moderate doses has become the most widely accepted treatment option for idiopathic SSNHL. However, one of the side effects is an increase in blood glucose level, which can limit the use of steroid in diabetic SSNHL patients. The major pathophysiologic mechanism of glucose intolerance is glucocorticoid-induced insulin resistance resulting in an increment in hepatic gluconeogenesis [7]. Among the pharmacologic activities of KRG, the hypoglycemic effect has been most extensively studied [8,9,10,11].
The aim of the present study was to examine whether the combined use of KRG was effective in elevating the hearing recovery rate in SSNHL patients undergoing systemic steroid therapy, and in addition, to investigate its effect on glucocorticoid-induced hyperglycemia [12].
Go to : 
MATERIALS AND METHODS
Subjects
The Institutional Review Board of the hospital approved the study, and adult subjects who submitted written informed consent were enrolled. Between March 2009 and April 2011, data was collected prospectively from the subjects diagnosed with SSNHL. The diagnostic criteria for SSNHL in this study were the idiopathic hearing loss of 30 dB or more in three contiguous frequencies that occurred abruptly or progressively within a few days. Patients with systemic diseases other than diabetes or hypertension were excluded. In addition, the patients with known etiology of hearing loss or other otologic conditions were excluded by a thorough history, physical examination and radiologic studies. The subjects were divided randomly into 2 groups: the steroid alone and the combination of steroid and red ginseng.
Assessment of auditory function and blood glucose
Pure tone averages (PTA) were obtained from the pure tone thresholds at 0.5, 1, 2, 3, 4, and 6 KHz of pure tone audiogram at the first visit and 2-month follow-up. Hearing gain was defined as the change in PTA between the two analyses. The severity of hearing loss was categorized as mild (25-40 dB), moderate (41-70 dB), severe (71-90 dB), and profound (>90 dB). The types of audiogram were determined by the audiometric curve patterns: ascending, descending, flat, and U-shaped. The treatment responses were classified into complete recovery, partial recovery, slight improvement, and no improvement, according to the criteria proposed by Siegel [13].
All subjects were hospitalized for treatment. Blood samples were obtained at 7:00 AM on the treatment day 1 and 5 before administration of medications. The fasting blood glucose was measured at the hospital laboratory using glucose oxidase method. The data from the diabetic patients with a current use of anti-diabetic medications were excluded from the statistical analysis.
Treatment protocol
All subjects in both groups were treated with a 10-day course of orally administered methylprednisolone at tapering doses: a daily dose of 48 mg twice a day (every 12 hours in the morning and afternoon) for 5 days, and thereafter, decreasing 8 mg a day for the next 5 days (40 mg to 8 mg). In the combination group, the patients received KRG extract (KRG powder capsule, 500 mg; Korea Ginseng Co., Daejeon, Korea) at a daily dose of 3 g by mouth 3 times a day for 20 days, in addition to methylprednisolone. Other treatment modalities for SSNHL were not implemented in both groups.
Data analysis
Before treatment, initial clinical characteristics and the factors that can bias the treatment outcomes were compared between the groups: age, gender, affected ear, duration, PTA, blood glucose, the severity of hearing loss, the type of audiogram, and the presence of vertigo. Data was analyzed with the paired t-test to compare the pre- and posttreatment mean PTAs/blood glucose levels in each group. The mean hearing gains were compared between the groups using Student t-test; the treatment responses, Pearson χ2 test. A P-value of <0.05 was considered significant.
Go to :
RESULTS
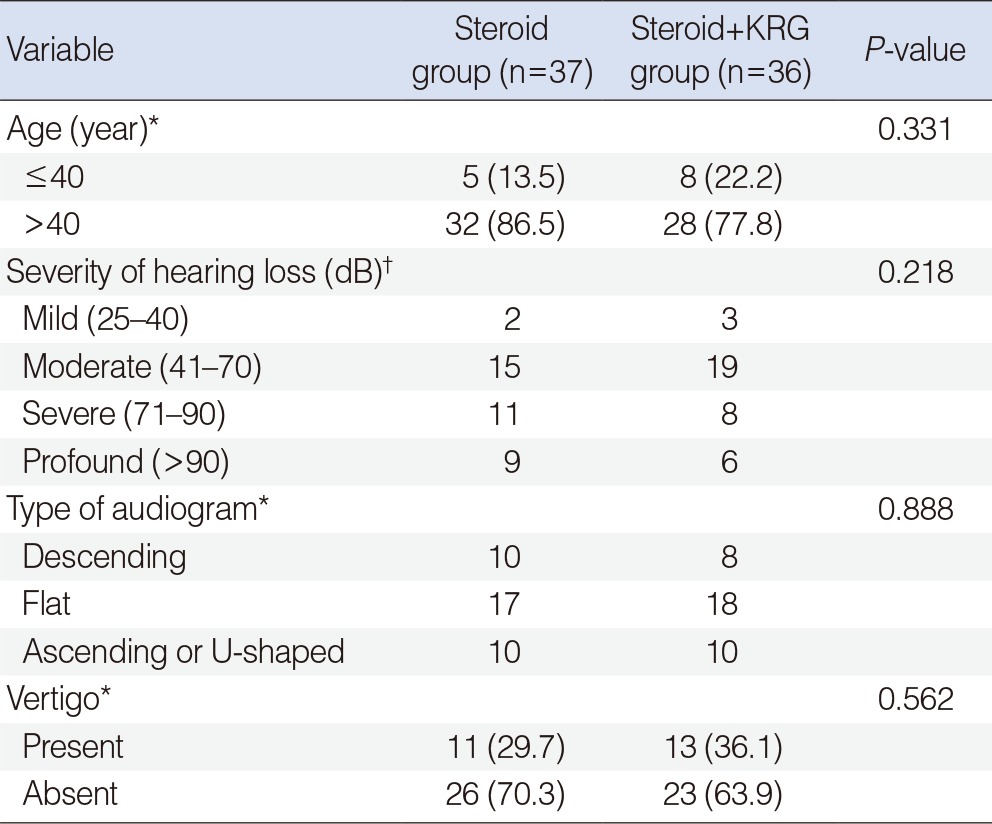
Thirty-seven subjects in the steroid group were 13 men and 24 women, with a mean±SD age of 56.6±12.7 years ranged from 22 to 77 years. The combination group of 36 subjects was composed of 14 men and 22 women, with a mean±SD age of 50.8±12.8 ranged from 23 to 70 years. Clinical characteristics, PTAs, and blood glucose levels showed no significant differences between the groups before treatment (Table 1). Patient distribution was also similar in each category of the prognostic factors: age, the severity of hearing loss, the type of audiogram, and the presence of vertigo before treatment (Table 2).

At the 2-month follow-up, PTAs improved significantly in both groups as expected (Fig. 1A). Although the mean hearing gains appeared to be slightly higher in the combination group (30.0±23.8 dB) than in the steroid group (25.1±17.7 dB), the difference was not statistically significant (Fig. 1B). The proportion of patients with a complete or a partial recovery accounted for 43.2% in the steroid group, and 50.0% in the combination group along with the equal distribution of subjects in each category of treatment responses. Data are described in Table 3.
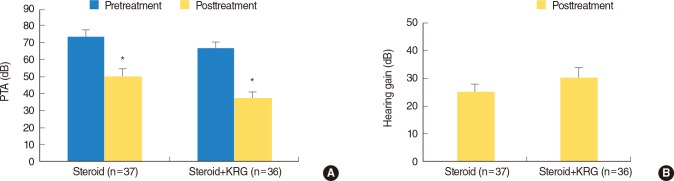 | Fig. 1Hearing improvements at 2 months in the steroid and combination groups. (A) Pure tone average (PTA) improved from 73.9±24.3 (mean±SD) dB to 50.2±25.5 dB in the steroid group; from 66.7±22.5 dB to 37.1±22.9 dB in the combination (steroid + Korean red ginseng [KRG]) group. *P=0.000, paired t-test. (B) Hearing gains demonstrate no significant difference between the groups: 25.1±17.7 dB in the steroid group, and 30.0±23.8 dB in the combination group. P=0.324, Student t-test. Error bars indicate SE.
|

The numbers of patients without diabetes who were the subjects of blood glucose analysis were 27 in the steroid group, and 34 in the combination group. The mean blood glucose was significantly elevated from 117.2 to 145.0 mg/dL (a 23.7% increase) on day 5 in the steroid group. In contrast, blood glucose level did not change in the combination group in spite of the steroid administration, which is shown in Fig. 2.
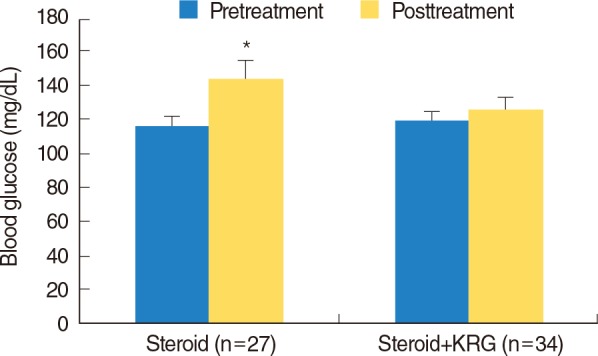 | Fig. 2Changes in blood glucose on day 5 in the steroid and combination groups. Pretreatment blood glucose was 117.2±26.2 (mean±SD) and 120.2±29.6 mg/dL in the steroid and the combination group, respectively; posttreatment value was 145.0±53.1 and 126.7±35.2 mg/dL in the steroid and the combination group, respectively. KRG, Korean red ginseng. *P=0.001 in the steroid group, P=0.371 in the combination group, paired t-test. Error bars indicate SE.
|
Go to :
DISCUSSION
The present study was designed to evaluate the therapeutic effects of KRG on hearing recovery and glucocorticoid-induced hyperglycemia in SSNHL patients undergoing systemic steroid therapy.
Principal theories of the etiology of idiopathic SSNHL include viral infection and vascular occlusion, and the viral origin has long been thought to be the most common cause. Treatment should be based on etiology, but the treatment options of SSNHL still depend on empirical guidelines. Besides the most commonly used oral steroids, vasodilators have been extensively used as an alternative or a combined regimen in the treatment of SSNHL, although no controlled study has shown a positive result.
We postulated that the previously reported antioxidant, antithrombotic activities [1,2,3,4,5,6], and the similar protective effects of KRG against neuronal damage in cerebral ischemia [14,15,16] might also have beneficial effects on SSNHL. However, our results revealed no difference in the hearing gain or in the recovery rate between the single steroid and the KRG-combined steroid therapies. We suggest that further study may be needed, in which the treatment groups consist of the placebo, steroid, and KRG groups.
Glucocorticoids are widely used in hospitalized patients, and commonly induce new-onset hyperglycemia in patients without a history of diabetes or will provoke severely uncontrolled hyperglycemia in patients with diabetes [17]. According to the American Diabetes Association guidelines, a subject with a consistent range of glucose level between 100 and 126 mg/dL is considered hyperglycemic, while above 126 mg/dL is generally held to have diabetes. However, no standard guidelines are currently available concerning the treatment of glucocorticoid-induced hyperglycemia [12]. It has been also reported that mild hyperglycemia produced by high-dose prednisone normalizes spontaneously in noncritically ill patients [18].
Red ginseng has been reported to normalize glucose homeostasis through a variety of mechanisms in experimental and clinical studies [8,9,10]. KRG mediates the crucial pathways that regulate insulin action and insulin secretion associated with the development of type 2 diabetes. Three types of anti-diabetic mechanisms were suggested in type 2 diabetes: enhanced insulin sensitivity in adipose tissue and skeletal muscle, enhanced insulin secretion, and increased β-cell mass in the pancreas [8]. In other reports, postprandial glycemia levels were lowered by KRG in healthy individuals [9], and KRG exerted a prophylactic action in type 1 diabetes [10]. Our study also demonstrated that while the steroid only group showed hyperglycemia, KRG-taking subjects exhibited a consistent glucose level in spite of the steroid administration. To the best of our knowledge, this is the first report on the hypoglycemic effect of KRG on glucocorticoid-induced hyperglycemia in normal (non-diabetic) subjects.
In conclusion, although the combined use of KRG with oral steroid did not provide greater therapeutic effects on hearing recovery than the steroid alone, we suggest that red ginseng can be a useful adjuvant to steroid therapy for SSNHL. It would help to normalize glucocorticoid-induced hyperglycemia in non-diabetic patients, during the treatment of SSNHL.
Go to :
 XML Download
XML Download