

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
During episodes of epilepsy, patients suffer from diverse visual symptoms (such as illusion, hallucination, and visual loss) and oculomotor signs (tonic eye deviation, eyelid blinking, or myoclonus) [1]. Epileptic nystagmus (EN) is defined as a quick, repetitive jerky movement of the eyeball associated with seizure activity [2]. Because EN is a rare accompanying phenomenon of epilepsy, fewer than 50 cases of EN have been reported [3].
A number of different cortical regions could induce EN. However, cases of EN due to ictal discharge from the posterior temporo-parietal-occipital region or occipital lobe have been reported [3]. In addition, there is still significant controversy regarding the exact pathophysiologic mechanism of EN. Clinically, epilepsy associated with simultaneous ictal discharge from multiple cortical lesions is not uncommon. In cases of EN associated with this multiple discharge, localization of the exact epileptogenic zone inducing EN could be difficult.
In a pediatric patient with EN and vertigo associated with bilateral temporal and frontal lobe epilepsy, we could infer the epileptic focus by interpreting the patient's clinical picture, characteristics of nystagmus, and findings of electroencephalography (EEG). Therefore, we report on this case with a review of relevant literature.
Go to : 
CASE REPORT
A nine-year-old female visited our outpatient clinic suffering from intermittent, rotatory vertigo for one year. Initially, she experienced a dizzy spell two or three times a week. The duration of vertigo was less than one minute. During vertigo attack, there was no loss of consciousness, visual loss or hallucination, or any orbital discomfort. Based on the clinical pictures (spontaneous rotatory vertigo lasting less than 1 minutes, symptoms sometimes related to positional change, and no prominent abnormal findings in neurologic function test), doctor at the local clinic prescribed medication for dizziness (dimenhydrinate 150 mg/day) under the initial diagnosis of benign paroxysmal positional vertigo. However, there was no improvement of the attacks of dizziness.
Two months before visiting our clinic, she had experienced more frequent (>10 dizzy spells in a single day) and severe vertigo attacks. Since then, her father has reported observation of rapid, jerky movements of the eyeball during vertigo attack. There were no accompanying neurologic, ophthalmologic, or audiologic complaints. Her father reported that he had experienced several attacks of generalized tonic-clonic seizure.
In order to rule out the peripheral cause of vertigo, we performed head shake test, head impulse test, Dix-Hallpike test and head rolling test. We also performed video nystagmography, caloric test and posturography during the interictal period. Results of all these examinations were normal during the interictal period.
Results of neurologic examination were normal during interictal phase. However, during the ictal phase, horizontal rapid left-beating nystagmus was observed for approximately 20 seconds. The rapid phase of nystagmus was left-sided, and the slow phase was right-sided without crossing the midline (Video clip 1, Supplementary material). There was no cognitive impairment, gaze deviation, cortical blindness, or visual hallucination during episodes of EN. No specific findings were observed on magnetic resonance imaging (MRI). Her ophthalmologic examination for visual acuity and visual field showed normal findings.
Interictal electroencephalography (EEG) showed no abnormal epileptic activity. Frequent ictal episodes were monitored during a 12 hour video EEG. During the left-beating nystagmus, the ictal EEG pattern showed rhythmic fast frequency spikes discharges initially in the right temporal regions (Fig. 1A), with rapid spread to both temporal regions (Fig. 1B). It was then followed by rhythmic fast spikes in bilateral frontal areas (Fig. 1C).
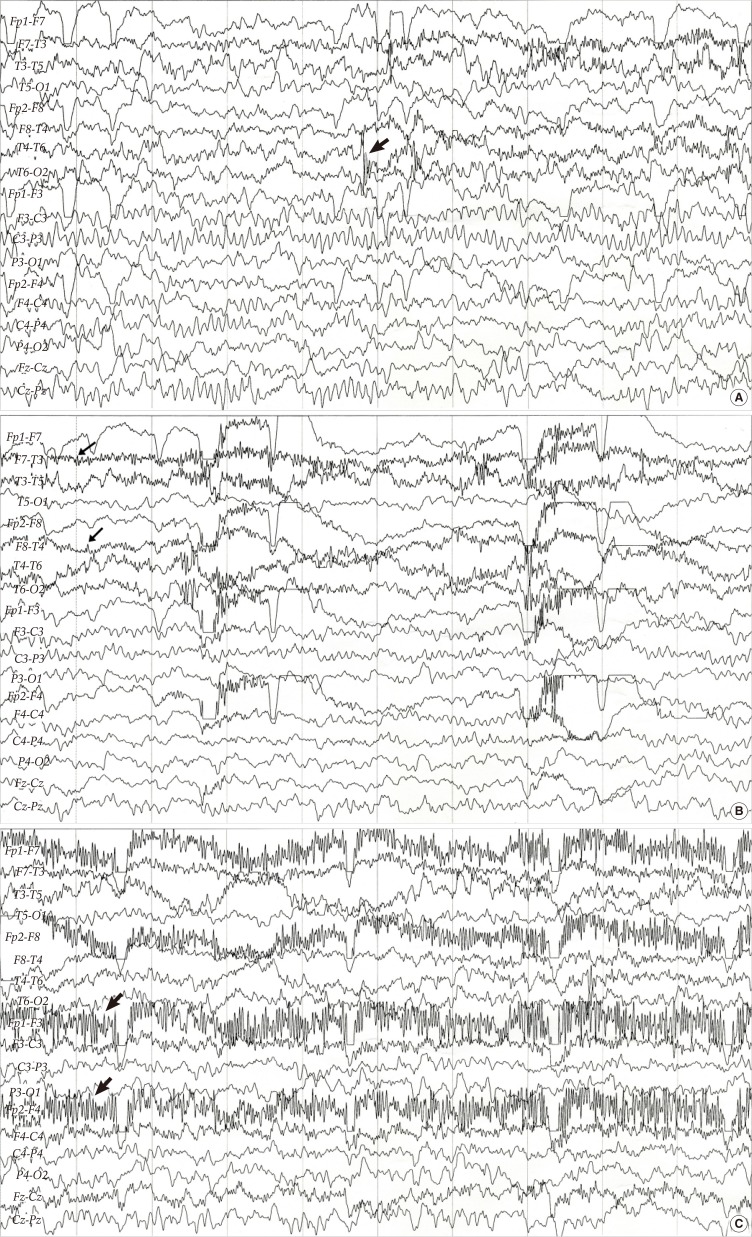 | Fig. 1Ictal electroencephalography shows (A) initial rhythmic fast spikes with discharges in the right temporal area (arrow) during the onset of nystagmus and vertigo and (B) continued rhythmic fast spikes in bilateral temporal regions (arrow). Which were followed by (C) rhythmic fast frequency spikes in the bilateral frontal area (arrow). Fp, frontopolar; F, frontal; C, cental; T, temporal; P, parietal; O, occipital; Even number, right; Odd number, left.
|
Under the impression of EN, we started carbamazepine (15 mg/kg/day). Only two days after the initial treatment, we observed a decrease in frequency (<10 times a day) and duration (<10 seconds) of EN and vertigo attack. After two weeks of treatment, she no longer complained of vertigo attack. Maintaining carbamazepine (15 mg/kg/day) since then, she had not experienced any dizziness for the previous 12 months.
Go to :
DISCUSSION
Vertigo is not a common complaint in the pediatric population, therefore, few studies of pediatric vertigo have been reported, compared to studies of the adult population [4]. EN is an uncommon ictal phenomenon characterized by repetitive jerking movements of the eye due to seizures [5]. It usually presents as binocular horizontal nystagmus and other symptoms and signs such as episodic gaze deviation, visual hallucinations, cortical blindness, and vertigo may be associated or not. Age onset of EN has been reported from 10 postnatal days to 75 years [5]. However, vertigo due to epilepsy in pediatric patients is very rare [5]. Therefore, it is difficult for physicians to suspect EN clinically as the possible cause of pediatric vertigo.
In patients with epileptic seizures, vertigo is known to be induced by temporal lobe epilepsy [6]. According to Bense et al. [7], the cortical saccade region (including the frontal eye field, supplementary eye field, parietal eye field, and posterior parietal lobule) and parieto-insular-vestibular cortex (PIVC, located at posterior parietal operculum and plays a pivotal role in central vestibular network) is also associated with vertigo. In our case, dizzy spells preceded EN for approximately 10 months. Therefore, we could suppose that epileptic discharge from the temporal lobe, cortical saccade region or PIVC could be responsible for the initial vertigo in our patient.
In most cases of EN, several oculomotor signs, including gaze deviation, blindness, or eye blinking are observed along with nystagmus [5]. However, in our case, there were absolutely no accompanying oculomotor signs, except nystagmus. Although many patients with EN have a brain anomaly, such as hemorrhage, tumor, cortical dysplasia, or cortical atrophy [5], in our case, MRI finding was completely normal. Under these conditions, definite diagnosis of EN would be quite difficult.
EN could be classified as two types according to their pathophysiologic mechanisms. In type I, the cortical saccade region (including the frontal eye field, supplementary eye field, parietal eye field, and posterior parietal lobule) is activated for production of epileptic discharge, and contributes to nystagmus with a contralateral fast component [8]. In type II, the Broadmann area 19/37/39 junction (temporo-parietal-occipital area) is involved in nystagmus with an ipsilateral slow component [8]. In our case, as there was a left-sided fast component and right-sided slow component of nystagmus, right type I (contralateral) and right type II (ipsilateral) could both be responsible for the pathophysiologic mechanism. The main difference between each type is that the slow component does not cross the midline in type I, while the slow component crosses the midline in type II [8,9]. In our case, as the slow component of nystagmus did not cross the midline, the right cortical saccade region should be responsible for EN.
Although, in our case, we observed discharges from multiple brain areas during the ictal phase, we could suppose that discharges from the right temporal area should be responsible for the EN. In fact, initial ictal discharges started from the right temporal region, spreading to other brain areas. Therefore, in such a confusing case, thorough understanding of the pathophysiologic mechanism of EN could be helpful in localizing the brain area responsible for nystagmus and dizziness.
Further imaging modality, such as single photon emission computer tomography (SPECT), could be considered for better localization of epileptic lesions [2]. Although one study identified interictal hypoperfusion and ictal hyperperfusion using SPECT [10], few research studies on the correlation between EEG findings and SPECT image have been reported. Nicita et al. [2] recently reported that suspected brain lesions from EEG findings showed strong correlation with active foci during the ictal phase in SPECT images. In our case, SPECT could have further localized and confirmed cortical lesions associated with EN and vertigo among multiple foci. However, due to parents' dissent, we could not perform SPECT.
Previous researchers reported that eyeball movements could cause artifacts to readings of EEG [11]. However, in our case, ictal discharge preceded nystagmus. Therefore, EEG artifact caused by nystagmus could be ruled out. Furthermore, after the anti-epileptic medication, patient's symptoms of vertigo and nystagmus were totally subsided.
In conclusion, putting clinical findings, characteristics of nystagmus, and EEG findings together, we could induce a possible focus of EN among multiple brain lesions in the bilateral hemisphere. As an ENT doctor, we should suspect brain lesions in cases with prolonged, unexplained vertigo refractory to conventional medication, such as in our case. And we should also perform several studies, including MRI and EEG, in cases with seizure activity and atypical nystagmus which could not be explained by peripheral neuropathy. And, if EEG shows abnormal findings, such as ictal discharge, further imaging study, such as SPECT could be considered for better localization of the lesion.
Go to :

 XML Download
XML Download