

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Tinnitus retraining therapy (TRT) that consists of directive counseling and sound therapy to promote habituation of reaction and habituation of perception has been widely accepted as an effective therapeutic option for tinnitus relief [1,2]. Individualized counseling session, one of the hallmarks of TRT, requires a considerable time commitment and trained specialists; therefore, it is not easy to implement it in general otolaryngologic practices other than specialized tinnitus clinics. Ever since TRT was introduced by Jastreboff, the technique of TRT has been modified and customized by practitioners.
Although TRT is one of the popular treatment modalities for tinnitus, it is not a causal, but a behavioral treatment that does not regard its etiology. Pharmacologic interventions with benzodiazepines or other GABA agonists aim at reducing the tinnitus-related neuronal activity, based on the hypothesis of central neural hyperactivity after loss of inhibition [3-7].
The authors have treated chronic tinnitus patients using a combination of a simplified TRT and oral medications for the last ten years: a single session of directive counseling, ambient sound stimulation, and a short-term pharmacologic therapy with alprazolam and ginkgo biloba extract, which has been called a modified TRT. In the previous study, we reported the therapeutic efficacy of this combination version of TRT [8]. Subsequently, we also have attempted small-group counseling in order to find a time-effective equivalent of prototypical individual counseling, which can be applied more easily even in crowded otolaryngology clinics.
The aim of the present study was to evaluate the effectiveness of the small-group counseling in our modified TRT by comparing the treatment outcomes between the individual and the small-group counseling.
Go to : 
MATERIALS AND METHODS
Subjects selection and outcome measures
Data was collected from the patients who presented to our clinic for chronic tinnitus perceived for at least 3 months between January 2009 and December 2010, and met the inclusion criteria. The institutional review board approved this study. The authors retrospectively reviewed the 6 months' outcomes of our tinnitus management protocol.
Patients underwent a full otolaryngologic examination and audiometric tests to rule out any other pathology causing the tinnitus. A standardized interview form and validated tinnitus questionnaires were used to ask the patients to score the subjective severity of their tinnitus. These self-rating scores constituted the following outcome measures: awareness (AW, percent of time aware of tinnitus during the waking hours), 10-point visual analogue scale (VAS) for tinnitus loudness (LD), annoyance (AN), and effect on life (EOL) [9], and tinnitus handicap inventory (THI) [10,11]. The same questionnaires were repeated at 3 and 6 months' follow-up after the initial interview.
We classified patients according to Jastreboff's category [9]. The patients in category 1 and 2 were included except those who had sensorineural hearing loss of more than 50 dB, because of the difficulty in conducting appropriate group counseling and the need for sound therapy with hearing aids. Category 0 patients with a minimal problem exhibiting no handicap (THI scores 0-16) were excluded from this protocol because most of the patients in this category only needed a single session of directive counseling without medications. Category 3 and 4 were also excluded owing to the heterogeneous adoption of the TRT protocol along with the small number of the patients. The subjects were placed into two groups: group 1:1 for one-on-one counseling during the former study period, and group 1:4 for one-on-four counseling during the latter study period.
A modified TRT
All subjects in both groups received a single session of directive counseling from a single TRT specialist (the first author). The counseling session, presented with a Power Point display for 30 minutes, consisted of the following contents: the education of the neurophysiological model of tinnitus [1] and the process of habituation, general information on hearing and tinnitus, tinnitus demystification, motivation, reassurance, and advice to avoid silence and add pleasant sounds to any quiet environment for ambient sound stimulation. At the end of the counseling, a short question-and-answer session was provided for the participants. In addition to wthis simplified TRT, alprazolam in a daily dose of 0.25 mg and ginkgo biloba extract in a daily dose of 80 mg were administered orally to every subject for 3 months. The patients were recommended to revisit at 3-month intervals.
Outcome assessment and data analysis
The initial data including the patient profiles, pure tone threshold average (PTA) at 0.5, 1, 2, and 3 kHz, Jastreboff's category, and the subjective tinnitus severity scores were compared between groups 1:1 and 1:4. Treatment outcomes were evaluated using patients' compliance based on the follow-up rates, and the multiple outcome measures: the scores for AW, LD, AN, EOL, and THI. Follow-up rates at 3 and 6 months were compared between the groups using the chi-square test. The mean AW/LD/AN/EOL/THI scores at the 3-month follow-up were compared with the initial values in each group using the paired t-test. In the subjects available at 6 months, the changes in the above scores at the three points of time-pretreatment, 3- and 6-month follow-ups-were compared within each group and between the groups using repeated-measures ANOVA and multiple comparison corrected by Bonferroni's method. Treatment responses were classified as improvement, no changes, and worsening, according to the changes in the self-report scores. The criteria for improvement/worsening were a decrease (improvement)/an increase (worsening) of ≥ 20 points in the AW score; ≥ 2 points in each of the LD, AN, and EOL score; ≥ 20% with respect to the initial value in the THI score. The frequency distributions in each response category were compared between the groups using the chi-square test. A P<0.05 was considered significant.
Go to :
RESULTS
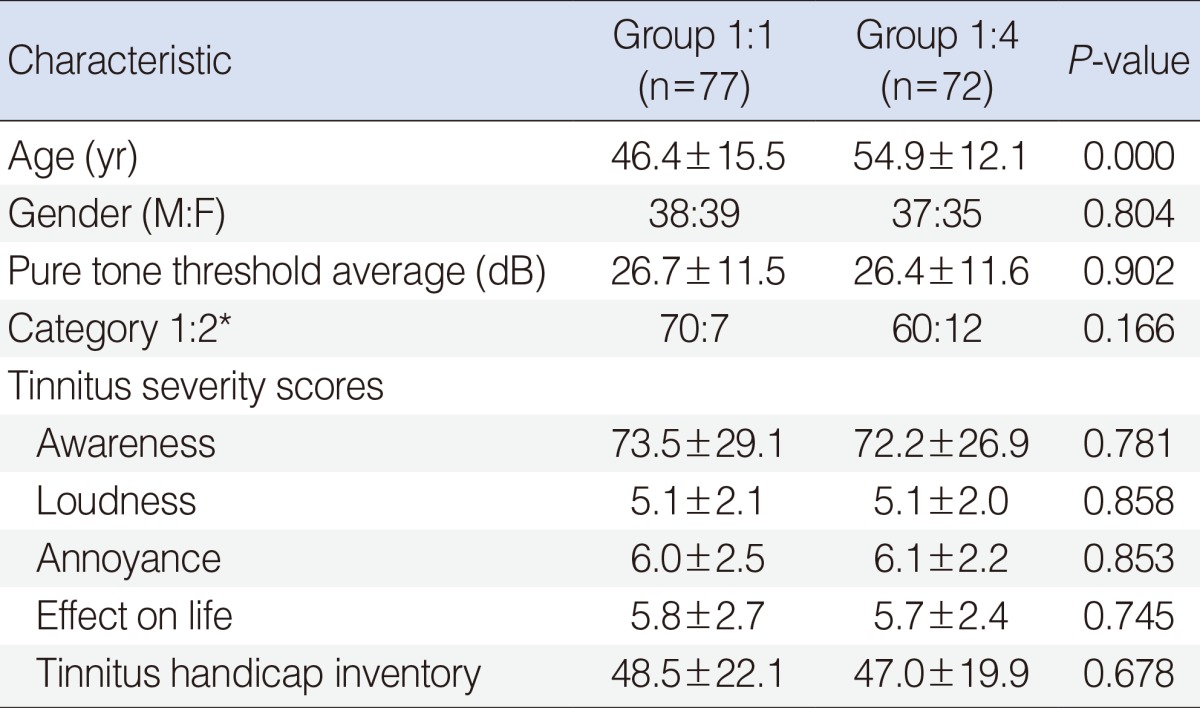
Group 1:1 comprised 77 subjects (38 men, 39 women; mean age, 46.4 years; range, 18 to 76 years), and group 1:4, 72 subjects (37 men, 35 women; mean age, 54.9 years; range, 20-76 years). The patients in Jastreboff's category 1 were 70 in group 1:1, and 60 in group 1:4; those in category 2 were 7 in group 1:1, and 12 in group 1:4. The groups were balanced for gender, category, PTA, and the tinnitus severity scores except for age (Table 1).
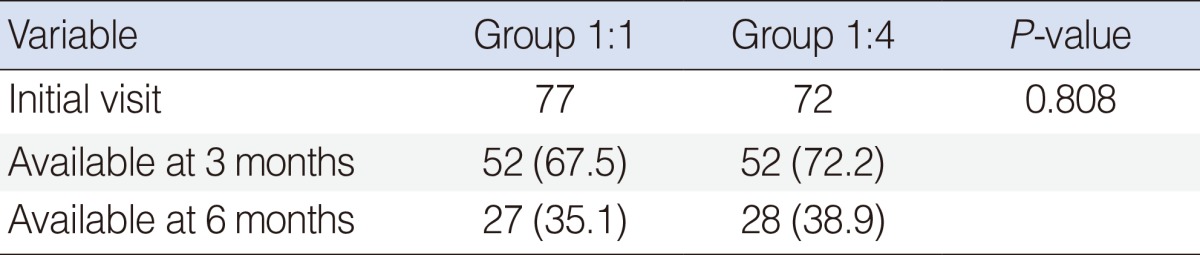
Of the total 149 patients, 104 patients completed the protocol at 3 months; 55 patients, at 6 months. Group 1:1 patients available for the 3-/6-month assessment were 67.5/35.1%; group 1:4, 72.2/38.9%. The follow-up rates showed no difference between the groups (Table 2).
Changes in the tinnitus severity scores following the treatment were as follows: the mean AW/LD/AN/EOL/THI scores decreased from 71.7±30.5 (mean±SD)/5.1±2.1/6.1±2.5/5.8±2.8/49.8±21.5 to 51.4±32.1 (P=0.000)/4.4±2.3 (P=0.053)/3.8±2.5 (P=0.000)/4.1±2.7 (P=0.000)/36.1±23.8 (P=0.000) in group 1:1 at 3 months (n=52); from 71.7±28.5/5.1±2.2/6.0±2.3/5.7±2.2/47.7±18.4 to 54.6±27.6 (P=0.000)/4.7±2.0 (P=0.091)/4.2±2.0 (P=0.000)/4.4±2.2 (P=0.000)/38.1±19.7 (P=0.001) in group 1:4 at 3 months (n=52). Both groups showed significant declines in these outcome measures except for LD as shown in Fig. 1.
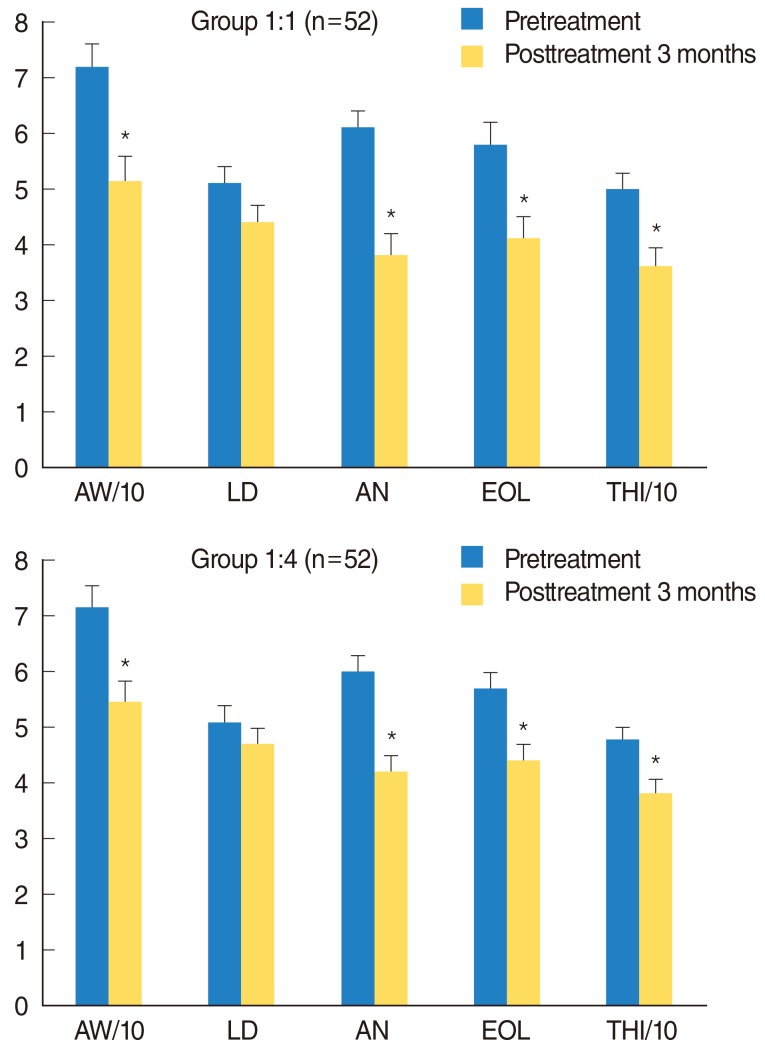 | Fig. 1Changes in tinnitus severity scores at 3 months after modified tinnitus retraining therapy. All scores except LD improved significantly in both groups (*P<0.05 vs. pretreatment scores, paired t-test). AW, awareness; LD, loudness; AN, annoyance; EOL, effect on daily life; THI, tinnitus handicap inventory. Error bars indicate SE.
|
In the total 55 patients who were follow-up at 6 months, the above five scores before the treatment were not different between group 1:1 and group 1:4. All the mean scores declined significantly throughout 6 months within each group, but showed no between-group difference. However, the values between the 3- and 6-month assessments were not different (Fig. 2).
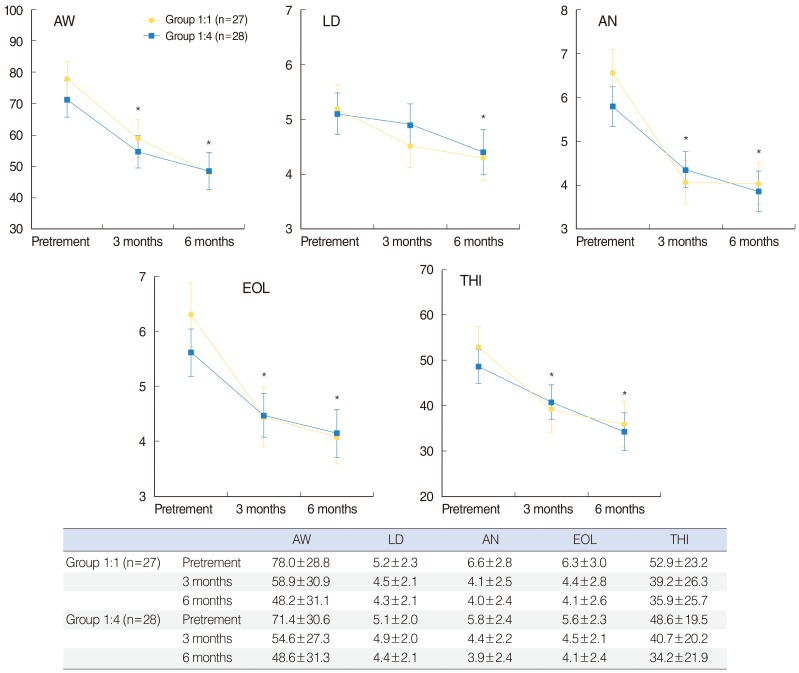 | Fig. 2Changes in tinnitus severity scores at 3- and 6-months after modified tinnitus retraining therapy. The pretreatment scores are not different between the groups (t test). All scores declined significantly throughout 6 months without between-group difference (*P<0.01 vs. pre-Tx scores, repeated-measures ANOVA). The slow declines from the 3- to 6-month values are not statistically significant. Data presented in the table are mean±SD. Error bars indicate SE. AW, awareness; LD, loudness; AN, annoyance; EOL, effect on daily life; THI, tinnitus handicap inventor.
|
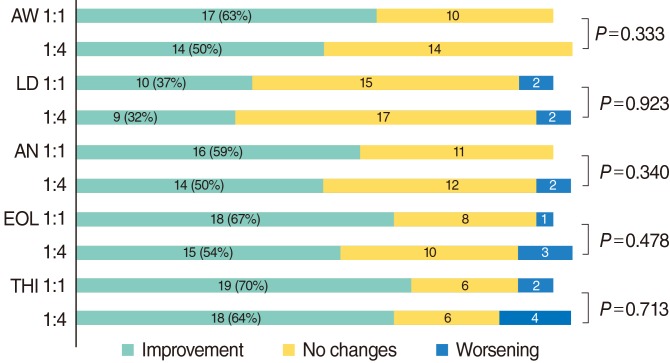
Treatment responses assessed only in the patients available at the follow-ups were similar in both groups. At 3 months after the initial treatment, 60% of group 1:1 and 48% of group 1:4 exhibited improvements in AW; 60% of group 1:1 and 50% of group 1:4, in THI. With regard to LD, only 33% in group 1:1 and 23% in group 1:4 showed improvements. At 6 months, 63% of group 1:1 and 50% of group 1:4 exhibited improvements in AW; 70% of group 1:1 and 64% of group 1:4, in THI; 37% in group 1:1 and 32% in group 1:4, in LD. There were no between-group differences in the patient distributions in each response category. The details based on each outcome measure are presented in Figs. 3 and 4.
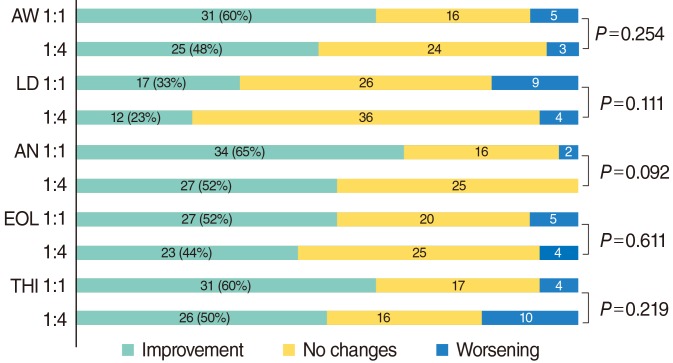 | Fig. 3Therapeutic outcomes based on each tinnitus severity score at the 3-month assessment. Data presented are number of patients. Improvement/worsening=a decrease/an increase of ≥ 20 points in the AW score; ≥ 2 points in each of the LD, AN, and EOL score; ≥ 20% with respect to the initial value in the THI score. 1:1=group 1:1 (n=52); 1:4=group 1:4 (n=52), chi-square test. AW, awareness; LD, loudness; AN, annoyance; EOL, effect on daily life; THI, tinnitus handicap inventor.
|
Go to :
DISCUSSION
The authors evaluated the effectiveness of a small-group version of the modified TRT through retrospective study on chronic tinnitus patients. Our previous study proved that a combination of TRT and short-term medications with alprazolam and ginkgo biloba extract has greater efficacy than the medical therapy alone [8]. The present study aimed to find an effective simple method that is equal to individual counseling in our modified TRT setting for tinnitus, because few studies have been found on this kind of a combination therapy.
In this study, we adopted one-on-four counseling and ambient sound stimulation as the primary therapeutic modality for chronic tinnitus. This small-group counseling showed equal treatment outcomes comparable to individual counseling in multiple tinnitus severity scores. The scores for THI, AW, LD, AN, and EOL declined significantly over a period of 6 months. The success rate based on the THI score, most commonly used outcome measure, was 70% and 64% in the individual and the small-group counseling patients, respectively at the 6-month follow-up.
Nevertheless, the present study has some limitations. (1) There was no control group because this was a retrospective study and we did not have a waiting list for counseling. The primary benefit of this group counseling was that the patients could undergo TRT as soon as possible. In addition, only the patients with chronic tinnitus were selected for this management protocol. It is hard to speculate that they might have experienced spontaneous relief from their tinnitus without any treatment. (2) Therapeutic results were assessed only through 6 months; thus, the long-term stability of the improvements is unknown. (3) The criteria for enrollment were strict, excluding anyone with more than a mild hearing loss, no handicap in category 0, acute tinnitus, or hyperacusis. Therefore, a broad interpretation of the results to general tinnitus populations requires caution. (4) Although it was reported in a few studies that benzodiazepines may impair brain plasticity and reduce the ability to habituate [12], there is still a controversy regarding the use of these medications. Our over-10-year experience of tinnitus management revealed that many patients, especially those who suffered sleep disturbance (frequently associated with tinnitus), preferred a combined medical therapy to the behavioral therapy alone. Besides, we used a protocol of a short-term minimal dose that did not interfere with the learning ability. Alprazolam was documented to improve loudness level and the VAS score for loudness in two reports [13,14]. One of the complex pharmacological actions of ginkgo biloba is to increase microcirculatory blood flow to the inner ear [15]. In the earlier studies, the disagreeing therapeutic results of gingko biloba as a treatment for tinnitus can be attributed to no standard methodology, no optimal dosage, or no use of validated tinnitus questionnaires [15,16]. (5) The overall success rate, based on the most common outcome measures like THI or AW, was not calculated due to follow-up losses during the treatment course, although there is no consensus on the best standard criteria for determining successful outcomes.
At present, the choice of a treatment for tinnitus can be multiple. Disadvantages of TRT include a relatively long treatment period, time-consuming directive counseling, a need for trained counseling specialists, and the instrumentation of high economic cost.
In conclusion, despite some limitations, the results of the present study indicate the potential efficacy of this small-group version of our modified TRT. The small-group counseling could produce benefits comparable to those produced by individual counseling for tinnitus relief. We suggest that the authors' fast and simple tinnitus management protocol can be implemented effectively in any crowded otolaryngology clinics.
Go to :
 XML Download
XML Download