

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Vestibular evoked myogenic potential (VEMP) is an inhibitory myogenic potential that results from ipsilateral saccular stimulation and can be measured from the contracted ipsilateral sternocleidomastoid (SCM) muscle. VEMP is mediated though the sacculocolic reflex arc, which reflects the function of the sacular macula, inferior vestibular nerve, lateral vestibular nucleus, vestibulaospinal tract and the motor neurons of the contracted ipsilateral SCM muscle [1]. Currently, VEMP is the only clinically available diagnostic tool that can reflect saccular function.
There are several parameters such as the presence of VEMP wave form, latency of p13 and n23 and peak-to-peak amplitude of the p13-n23 that can be used when interpreting the results of the VEMP response. Among the aforementioned parameters, interaural amplitude difference (IAD) ratio, which is the difference between the left and right side peak-to-peak amplitude [2,3], is most widely used. Though the amplitude of the VEMP response is greatly influenced by the contraction power of the SCM muscle: the amplitude of p13-n23 becomes larger as the contraction power of the SCM muscle increases [4]. Accordingly, if the contraction power of the bilateral SCM muscle is asymmetric, the IAD will be abnormally large which may be misinterpreted as unilateral saccular dysfunction. Even in normal subjects without torticollis, neck pain or cervical spine abnormality, the right and left muscle contraction power may be different. In order to overcome this problem, several methods that can control the muscle contraction power have been suggested. The most common method is to simultaneously monitor the mean rectification voltage of the SCM muscle using electromyography (EMG) while measuring the VEMP response. Blood pressure manometer monitoring has also been suggested as a method to normalize the SCM muscle contraction power [5,6]. Recently, a new method which the tonic EMG activity that occurs immediately before each sound stimulation is used for normalization of the VEMP results has been introduced [7]. This method is named the rectified VEMP (rVEMP) and is available with the Bio-logic Navigation Pro (Bio-logic System Co., Mundelein, IL, USA) evoked response potential system. In contrast to previous methods which monitor the contraction power and normalize it beforehand, rVEMP corrects the biased results afterwards even when the bilateral muscle contraction power is asymmetrical. Previous publications proved the validity of rVEMP in nearly symmetric SCM muscle contraction conditions. However, it is still not clear if rVEMP is able to correct the asymmetric muscle contraction power when the bilateral contraction power is significantly different. This study was performed in order to question the capacity of rVEMP in correcting significantly asymmetric muscle contraction power.
Go to : 
MATERIALS AND METHODS
Subjects
We tested 20 healthy subjects (16 male, 4 female) ranging in age from 26 to 33 years (average, 28.2 years). All subjects was given informed patient consent. All of the subjects had face-to-face interview with an otolaryngologist who had at least 3 years of clinical experience in dizziness and hearing loss. During the interview, any history of hearing loss or dizziness was screened and a written informed consent concerning that they do not have any health related problem was singed. All of the subjects were healthy young doctors who had specialized medical knowledge on their physical condition including inner ear problem. Subjects had normal hearing (pure tone hearing levels measured at 0.5, 1, 2, and 4 kHz was <20 dB HL) and were free of vestibular, neurological and inner ear pathologies. Their tympanic membranes were also pathology free. The study was approved by the Dankook University Hospital Ethics Committee.
VEMP measurement
The experiments were performed with an auditory evoked potential system, Navigation Pro ver. 6.1.0. The active electrode was placed on the skin overlying the medial portion of contracted SCM, the reference electrode on the upper part of the sternum and the ground electrode on the forehead. Skin impedances were <5 kΩ. The responses were obtained from each side separately using a pure tone (500 Hz, 100 dB nHL and the stimulation rate was 5.1/seconds).The rise and fall times were 4 ms and the plateau time was 2 ms. We consider the positive peak as P13 when the latency was within 11.3-15.9 ms, and we consider the negative peak as N23 when the latency was within 19.1-25.9 ms. The system obtained averaged waveforms and the user marked their points (p13 and n23). The non-rectified interaural amplitude difference ratio (IAD) = Amp_left-Amp_right) / (Amp_left+Amp_right) was first calculated with the conventional non-rectified VEMP response data.
For rectification, we chose a prestimulus rectification (PSR) function on selected waveforms and averaged the absolute value of the prestimulus muscle contraction power data during 20 msec. That value is divided into each of the 256 points along the collected VEMP waveform. Finally, new rectified waveforms are calculated [7]. The rectified IAD was calculated once more with the rectified VEMP response data. After rectification, the amplitude of the rectified VEMP became smaller than that of the conventional VEMP. But since the noise as well as the signal was rectified together, the signal to noise ratio did not change substantially.
Asymmetric muscle contraction
In order to induce compulsory asymmetric muscle contraction, the subjects were instructed to turn their head in the yaw plain. While lying down on the bed based on the subject's head location, 0°, 15°, 30°, and 45° points were marked on the ceiling (Fig. 1). Then the subjects were instructed to gaze straight at the target point by turning their head but not their eyes. The subjects were also instructed to elevate their head 2 cm from bed to provide sufficient muscle tension. The VEMP response was first obtained at 0° (no asymmetry between the bilateral SCM muscles). Afterwards, VEMP response was obtained at 15° (slight asymmetry), 30° (moderate asymmetry), and 45° (severe asymmetry). In between each condition a 3-minute break was allowed to prevent fatigue of the neck muscles.
 | Fig. 1Position of the subject to induce asymmetric muscle contraction. First, the ceiling was marked for 0°, 15°, 30°, and 45° rotations. The vestibular evoked myogenic potential (VEMP) was measured in the supine position while the head was elevated 2 cm from the bed. The head was then turned towards the right at 0°, 15°, 30°, and 45°. The VEMP was recorded in each position.
|
Muscle contraction power asymmetry
Before proceeding with the main experiment, the muscle contraction power was quantified by a electromyography system (Medelec Synergy, Oxford Instrument Inc., Surrey, UK) during 4 different positions: head rotation at 0°, 15°, 30°, and 45°. The subjects were instructed to turn their head towards the right side. Consequently, the left side SCM muscle contraction power was stronger than that of the right side. This difference was quantified using the following formula: muscle contraction power asymmetry (%)=(left muscle contraction power - right muscle contraction power)/(left muscle contraction power + right muscle contraction power)×100. For this preparatory experiment, 10 healthy subjects were included (5 men, 5 women) ranging in age between 26 and 31 years (average, 28.1 years).
Data analysis
Statistical analysis was performed using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). The results were expressed in means±standard errors. A Mann-Whitney U-test and Wilcoxon test were used for analysis and a P<0.05 was considered significant.
Go to :
RESULTS
Muscle contraction power asymmetry
Muscle contraction power on the stronger side (left side) was 191.9±13.4 mV at 0°, 264.6±11.5 mV at 15°, 331.7±15.0 mV at 30°, and 375.1±24.1 mV at 45°. Left side muscle contraction power increased in a linear pattern as the head was serially turned more and more towards the right side. Muscle contraction power on the weaker side (right side) was 181.2±11.7 mV at 0°, 169.9±13.9 mV at 15°, 159.3±14.1 mV at 30°, and 146.4±16.8 mV at 45°. Right side muscle contraction power decreased in a linear pattern as the head was serially turned more and more towards the right side. The muscle contraction power asymmetry was 6.7±1.8% at 0°, 22.5±3.5% at 15°, 35.8±3.6% at 30°, 44.8±4.6% at 45° (Fig. 2).
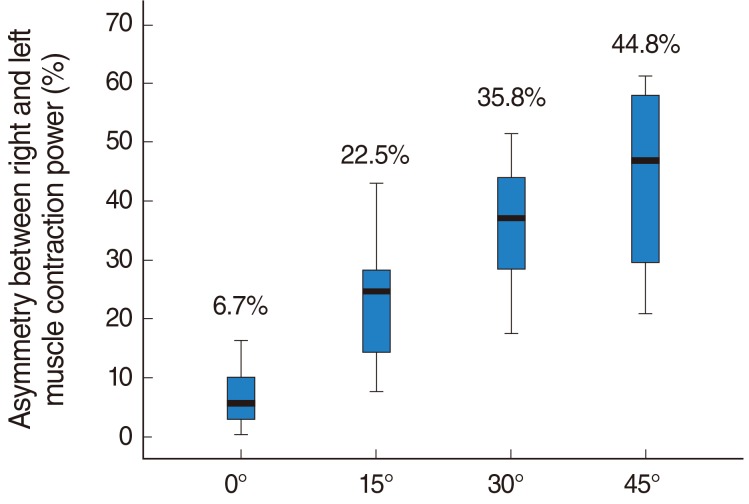 | Fig. 2Asymmetry between right and left muscle contraction power. The asymmetry of muscle contraction power increased in a linear pattern as the head was turned more towards the right side. This difference was quantified with the following formula: muscle contraction power asymmetry (%)=(left muscle contraction power-right muscle contraction power)/(left muscle contraction power+right muscle contraction power)×100.
|
Interaural amplitude difference ratio
IAD in non-rectified conventional VEMP (nVEMP) was 0.25±0.03 at 0°, 0.33±0.03 at 15°, 0.43±0.04 at 30°, and 0.44±0.03 at 45°. The IAD of nVEMP increased as the head rotation angle increased, in contrast plateaued at 30° and 45° (Fig. 3). The IAD of nVEMP during asymmetric muscle contraction (15°, 30°, and 45°) was significantly larger than at 0° condition (0°-15°, P=0.038; 0°-30°, P<0.001; 0°-45°, P<0.001).
 | Fig. 3Interaural amplitude difference (IAD). The IAD of non-rectified conventional vestibular evoked myogenic potential (nVEMP) increased as the head rotation angle increased but plateaued at 30° and 45° (A). IAD during asymmetric muscle contraction (15°, 30°, and 45°) was significantly different from the 0° condition. The IAD of rectified VEMP (rVEMP) was stable with minimal differences from 0° to 30°, but significantly increased at 45° (B).
|
The IAD in rectified VEMP (rVEMP) was 0.34±0.03 at 0°, 0.38±0.04 at 15°, 0.37±0.04 at 30°, and 0.50±0.04 at 45°. The IAD of rVEMP was stable with a minimal difference between 0° to 30°, by contrast significantly increased at 45° (0°-45°, P=0.002).
Relative increase in IAD (ΔIAD)
In order to quantify the perturbation of IAD solely due to asymmetric muscle contraction, the IAD at 15°, 30°, and 45° was compared with 0°. The ratio of IAD at each position relative to 0° IAD was expressed as ΔIAD (ΔIAD=IAD at each position /0° IAD). The ΔIAD of nVEMP was 1.95±0.46 at 15°, 2.23±0.32 at 30°, and 2.39±0.32 at 45°. The ΔIAD of nVEMP was 1.85±0.43 at 15°, 1.48±0.18 at 30°, and 2.19±0.33 at 45° (Fig. 4). That is, while the IAD of nVEMP at 15° and 30° was 1.95-2.23 times larger than that of the 0°, the IAD of rVEMP at 15° and 30° was 1.48-1.85 times larger than for 0°. The ΔIAD of rVEMP was significantly smaller than that of nVEMP at 30° (P=0.05).
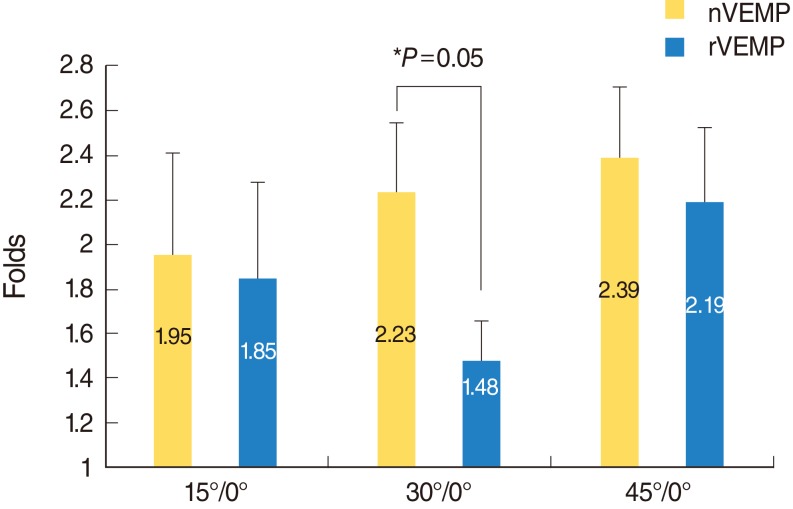 | Fig. 4Relative increase in interaural amplitude difference ratio (ΔIAD). In order to quantify the perturbation of IAD solely due to asymmetric muscle contraction, the IAD at 15°, 30°, and 45° was compared with that at the 0° condition. The ratio of IAD at each position relative to 0° was expressed as ΔIAD (ΔIAD=IAD at each position / 0° IAD). The ΔIAD of rectified conventional VEMP was significantly smaller than that of the non-rectified conventional VEMP at 30°. VEMP, vestibular evoked myogenic potential.
|
Go to :
DISCUSSION
It is well known that the amplitude of VEMP is significantly affected by the contraction power of the SCM muscle. It is necessary to minimize the effect of asymmetric muscular contraction power in order to improve the reliability of VEMP tests. There are several methods that are used to monitor symmetric muscle contraction such as mean rectified voltage monitoring through EMG and biofeedback through a blood pressure manometer. However, most commercial evoked potential systems do not allow for simultaneous electromyography monitoring while recording VEMP. Accordingly, mean rectified voltage monitoring through EMG requires a special experimental set-up [5]. Biofeedback through a blood pressure manometer has been suggested as an effective alternative. Since every clinic has a blood pressure manometer at hand, this method seemed to be a realistic solution. However a recent article has pointed out the limitation of this method [5].
rVEMP is a method that can theoretically compensate muscle contraction power asymmetry in the format of compensating the results of examination by measuring the muscle contraction powers in both sides while carrying out the examination. If this hypothesis is correct, rVEMP seems to be the simplest way to normalize asymmetric muscle contraction, since the evoked potential system itself can calibrate the asymmetry without further equipment or feedback. But the validity of this new method has not been evaluated thoroughly. It was our goal to elucidate if rVEMP can successfully correct asymmetric muscle contraction, especially when the muscle contraction power is significantly asymmetric.
From our results, we were able to prove that rVEMP was able to correct the asymmetric muscle contraction constantly up to 35.8% of asymmetry (30°), in contrast, was not able to compensate the asymmetry when the difference was too large (asymmetry of 44.8% at 45°). Also, when the ΔIAD was compared between nVEMP and rVEMP, we found a significant difference at 30°. This may imply that rVEMP was able to correct the muscle contraction asymmetry while nVEMP was not. It seems that rVEMP is capable of correcting the muscle contraction asymmetry, only when the asymmetry is smaller than 44.8% (<45°). When muscle contraction power asymmetry is larger than 44.8%, it exceeds the limit of the correcting capacity of rVEMP, and rVEMP cannot effectively correct for the asymmetric muscular contraction power. By contrast, it seems that this limitation is not clinically relevant, since an asymmetry of 44.8% is not a common situation during daily practice. When the patients are instructed to contract their bilateral muscles symmetrically as possible, the asymmetry should be less than this limit.
Another point requiring notification is that there was no significant difference in ΔIAD between nVEMP and rVEMP when the head's rotation is less than 15°. It is deemed that advantages that can be gained through rVEMP is insignificant when muscle contraction power asymmetry is less than 22.5% and rVEMP would not be absolutely necessary with small muscle contraction asymmetry. But, since it is difficult to predict whether the muscle contraction asymmetry will be small or large in each subject, it may be recommended to apply rVEMP in all cases.
There are several limitations in this study. The asymmetry of the SCM muscle was represented at only 4 positions: 0°, 15°, 30°, and 45°. Consequently, the effective range of rVEMP was presumed to be somewhere within 22.5% (15°)-44.8% (45°) of asymmetry. However, the exact amount of asymmetry that rVEMP is capable of compensating is not clear. If we had fractionated the conditions more finely, we might have been able to point out a limit of compensation more accurately. Results from this study were determined in normal subjects. Also, it is not clear if the same theory may be applied to patients with unilateral or bilateral vestibular weakness. This point may be a limitation of this study and may need verification in the future. Another limitation is that the age of all of our subjects was between 26 and 33 years. It is well known that amplitude of VEMP is influenced by aging [8,9]. Elderly patients have difficulty in contracting their neck muscles effectively. The effect of rVEMP in the elderly population seems to be clinically important, but this issue was not investigated in this study.
In this study, we showed that rVEMP has the capacity of correcting the asymmetrical muscle contraction power. Accordingly, if symmetric muscle contraction is questionable, rectified VEMP may be preferable. However, when the muscle contraction power asymmetry was more than 44.8%, rVEMP could not effectively correct for the muscular contraction power asymmetry. That is, rectified VEMP is not perfect and we should try our best to match the bilateral contraction power as much as possible. Similarly, when the muscle contraction power asymmetry was less than 22.5%, there were no significant difference between rVEMP and rVEMP. Accordingly, if symmetric muscle contraction can be guaranteed (ex. straight head elevation without head turning) rectification may not be needed. In conclusion, it seems that rVEMP is able to successfully correct the bilateral muscle contraction asymmetry, but only in a certain range of asymmetry.
Go to :
 XML Download
XML Download