

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Individuals with hearing impairments have been described as having speech characteristics that are low in intelligibility due to inappropriate resonance (1). There have been many studies comparing the speech characteristics of individuals with normal hearing (NH) and those who are hearing impaired (HI), as well as studies of individuals before and after receiving cochlear implants (2-4). Resonance problems are generally known as a nasal resonance problem (5). The degree of nasal resonance can be determined by obtaining a nasalance score as measured by a nasometer (6). Nasalance scores are measured during the production of passages that contain different proportions of stop consonants and nasal consonants, and they are used to judge the presence of hyper-nasality and/or hypo-nasality. Deviant nasal resonance, a common speech characteristic of an HI individual, is dependent on the phonemic context. For instance, hyper-nasality may be observed during one type of sound production, while hyponasality may also be reported at another time (7). Researchers who have completed previous studies on the speech problems of HI individuals have discovered that cochlear implantation has a positive influence in the recipients' lives by helping them to overcome their hearing loss through improvements in auditory feedback. Some studies have even reported that the aspects of deviant nasal resonance are similar to those seen in NH individuals (2-4). However, various acoustic variables still exist after cochlear implantation in children with hearing impairments at borderline or deviant levels (7). In addition, nasalance scores were reported as being significantly higher in HI than in NH individuals, regardless of the degree of hearing loss, age or the frequency of using hearing aids (8, 9). Although previous studies describing resonance problems using the measurements of nasalance scores have focused primarily on the velopharyngeal incompetency of individuals with cleft lip and palate, efforts have also been made to study the unique speech characteristics of HI individuals by relating the velopharyngeal functions to nasalance scores (10). Previous studies have been performed in order to investigate the speech characteristics and voice problems of HI individuals; however, strong conclusions were not able to be drawn as numerous variables had diverse explanations.
A cul-de-sac resonance, a typical resonance pattern observed in HI individuals, occurs due to the muffled airflow near the lower pharynx which blocks the resonance cavity (5, 11). In addition, previous studies have discovered incomplete closures during velopharyngeal closure in HI individuals, which explains the phenomenon in relation to nasalance score. However, nasal characteristics do not fully explain the problems of resonance as a whole (10), and the relations between velopharyngeal openings and the extent of nasality have been found to be statistically insignificant (10, 12). Therefore, not all resonance problems in HI individuals can be attributed to nasal resonance alone; the entire resonance cavity should be systematically evaluated.
Effective and appropriate resonances of speech sounds are produced when the sound energy created from the vocal cords effectively flows through the oral and nasal cavities, and such functions in each cavity must be controlled in the correct manner in order to create the appropriate resonance energy. However, HI individuals demonstrate a wide range of deviant vocal behaviors (7, 11, 13), which stimulate inappropriate resonance patterns by forcing the airflow and the resonance energy into a single cavity. As mentioned, HI individuals demonstrate deviant resonance patterns by either focusing the resonance energy in the lower pharyngeal cavity or by showing inappropriate resonance patterns in the nasal and oral cavities. New views are needed regarding the locations of resonance within the vocal tract. Therefore, this study attempted to study the ratings using the 'vertical focus of resonance (VFR)' tool to determine perceptual aspects by examining where the resonance energy is focused within the vocal tract and by describing the resonance qualities of HI individuals. In addition, the relationship between the focus of resonance and nasalance scores measured during the production of syllables or passages in diverse phonemic contexts were verified prior to the perceptual evaluation.
Go to : 
MATERIALS AND METHODS
Subjects
Two subject groups were comprised of NH and prelingual HI adults. Subjects in the HI group met the following conditions: 1) sensory-neural hearing loss in both ears with an average greater than 71 dB HL in the dominant ear (ANSI, 1989), 2) a hearing aid in one or both ears or the use of cochlear implants, 3) no neurological deficiencies, congenital deficiencies, such as cleft lip or palate, or functional phonological disorders, sensory disorders, cognitive disorders or behavioral disorders, 4) no vocal deficiencies, such as nodules, paralysis or polyps in the vocal cords, 5) no aspiration features in stop sound observed during the consecutive production of /pha/, and 6) no differences in waveforms from the results of repetitively producing /amma/ and /appha/ five consecutive times. Subjects who were not able to distinguish between the production of the nasal consonant /m/ and the stop consonant /pha/ were excluded from the study. The NH group was required to demonstrate the following: 1) normal hearing in both ears, 2) no neurological deficiencies, congenital deficiencies, such as cleft lip or palate, congenital or functional phonological disorders, sensory disorders, cognitive disorders or behavioral disorders, and 3) no vocal deficiencies, such as nodules, paralysis or polyps in the vocal cords. The age and gender ranges were similar in the two groups due to frequency matching as shown in Table 1. Both groups of subjects were recruited from a local university in the city of Cheonan. The HI individuals commonly used verbal speech and sign language, and most had severe to profound hearing loss prior to language acquisition. Each subject was asked to complete syllable and passage tasks in order to measure the nasalance scores with a nasometer.

Assessment tools
Nasometer assessment
To obtain the nasalance scores of the subjects' speech as Table 2 was provided as a source for the nasal resonance norm of an NH adult, based on passage tasks (14). Nasalance scores were used to determine hyper-nasality in the oral consonant passages and hypo-nasality in the nasal consonant passages (15).
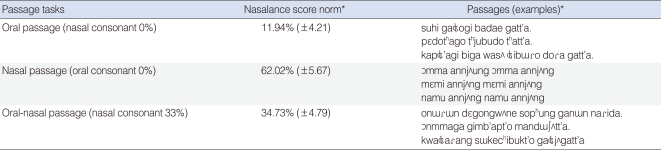
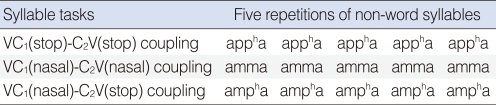
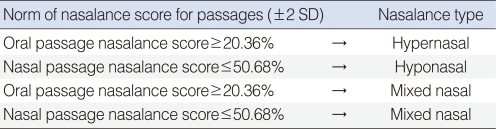
Subjects produced non-word syllables (/appha/, /amma/, and /ampha/) five times consecutively, as outlined in Table 3. The results from the tasks were used to categorize the normal and the abnormal nasalance groups, as determined by scores±standard deviations (SD) from the average nasalance score for the passage tasks in Table 2. The abnormal nasalance group was further categorized into subgroups, as described in Table 4. Nasalance cut-off scores were set according to previous studies. The standard nasalance score for hyper-nasality was set at greater than 20% in the oral passage (16), 20-30% was considered the borderline range, and a nasalance score greater than 30% was considered to be hyper-nasality (17). In another study, when deciding whether or not to perform pharyngeal flap surgery for children with cleft lip and palate, patients were asked to read both oral and nasal passages, which had a sensitivity level of 0.75, and a specificity of 0.91 (18). Thus, the rating standard of the nasalance score was set at 2SD. Nasalance scores greater than 2SD in the oral passage were considered as hyper-nasality, and scores that were below 2SD in the nasal passage were categorized as hypo-nasality. In cases where both hyper-nasality and hypo-nasality were shown in the oral passage and in the nasal passage, the subject was classified in the mixed nasal group.
Perceptual evaluation based on the VFR tool
Previous studies have generally focused on identifying resonance problems through nasalance evaluations. However, vocal vibrations produced from the larynx are processed not only through the nasal cavity, but also through the vocal tract, which acts as the resonator, as well as through the velopharyngeal valve vibrating within the oral cavity. While the vibration is processed through the oral cavity, the acoustic energy may be reflected from the hard palate and the teeth, which may produce an amplified volume of sound. Therefore, such oral structures may also function as a resonance cavity (19). When the acoustic energy produced from the vocal cords goes through the velopharynx, the soft palate and the base of the tongue, which are connected to the oral cavity, may prevent the resonance energy from going toward the nasal cavity, or it may induce the production of sound in the nasal cavity. When such structures within the resonating cavities show improper actions, or when the resonance energy is inappropriately focused at a specific location within the resonance cavity, a deviant resonance pattern may occur. Such standards are mentioned below in Fig. 1, and the ratings for the VFR are described in Table 5 by applying and modifying the faulty production (the settings for differentiating the place of phonation) from Shakespeare (1921) (20).
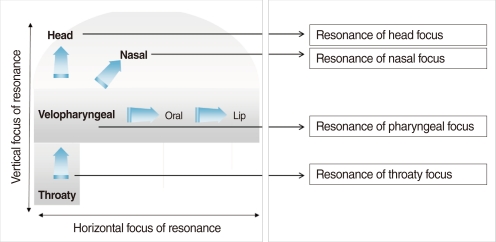

Fig. 1 describes the resonance problems that occur due to inappropriate focus of resonance. VFR used for perceptual evaluation as mentioned in Table 5. Three speech-language pathologists (SLP) were engaged to act as the perceptual raters for this study. All three were certified SLP and have more than ten years of clinical experience, focused primarily on velopharyngeal insufficiencies of cleft lip and palate patients.
After explaining the criteria for each VFR to the raters, the first trial for the rating using the VFR tool was completed. Two weeks later, a second trial of ratings was completed. The raters were given three speech samples, which were mixtures of oral and nasal passages (Table 2), produced by a severely HI adult. If the sound energy produced from the vocal cords showed inappropriate VFR, leading to deviant resonance problems, it was marked as 'Present' in Table 5. Since a participant may demonstrate several inappropriate vertical focuses of resonance from one speech sample, each participant could be marked as having multiple vertical focuses of resonance. We tried to identify the concordance between instrumental evaluation and perceptual rating, according to the results from the perceptual ratings and the nasometer illustrate the relationship between VFR and the nasalance score.
Statistical analysis
The Statistical Product and Service Solution ver. 15.0 (SPSS Inc., Chicago, IL, USA; 2006) was used to analyze the data. An independent samples t-test was performed in order to compare the mean differences between the task results of the NH group and the HI group, and a correlation analysis was completed between the nasalance scores and the task. In addition, the Fisher's exact test was used to clarify the relationship between nasalance scores and a perceptual rating, which fixed the significance level at 0.05.
Go to :
RESULTS
Comparison of nasalance scores from the NH and HI groups
Both the NH and HI subjects were asked to complete the 'stop to stop consonant coupling,' 'nasal to nasal consonant coupling,' and the 'nasal to stop consonant coupling' non-word syllable tasks. The average nasalance scores produced from these tasks, as measured by the nasometer and the SD, and the results from the two independent t-test were calculated (Table 6). The NH group demonstrated a significantly lower average than the HI group in the stop consonant syllable task, showing a nasalance score that was 6.16% lower (t=-3.298, P=0.002). On the other hand, the NH group received a higher average in both the nasal consonant task and the nasal-stop consonant task, scoring 2.25% (t=2.329, P=0.024) and 5.60% (t=4.272, P<0.001), respectively, in the nasalance scores. In the two independent t-tests for the passage task, the NH group demonstrated a significantly lower nasalance average than the HI group in the stop consonant passage, demonstrating a nasalance score that was 3.81% lower (t=-2.116, P=0.040). In addition, the NH group also showed 6.84% (t=5.377, P<0.001) and 11.54% (t=4.177, P<0.001) increases in the nasal consonant passage task and the nasal-stop consonant passage task, respectively, which were significantly higher scores than that of the HI group.

Comparison of nasalance scores in the syllable and passage tasks
A correlation analysis of the nasalance scores in both syllable and passage tasks ('stop-stop coupling,' 'nasal-nasal coupling' and 'nasal-stop coupling') for both groups were determined (Table 7). In Table 7, the correlation analysis results for the NH group are indicated above the diagonal line, and the HI group results are below the diagonal line. In the NH group, while the nasal-nasal syllable task and the nasal-stop syllable task showed statistically significant correlations, the stop-stop syllable task and the nasal-nasal syllable task did not show any significant correlations. Moreover, neither the oral passage task nor the nasal passage task demonstrated a significant relationship to either the nasal-nasal syllable task or the stop-stop syllable task. The results of the passage task differed from the syllable task, demonstrating statistically significant correlations in the oral passage task, the nasal passage task and the nasal-oral passage task. The correlation analysis results for the HI group in each task were different from those of the NH group, demonstrating statistically significant correlations in all tasks within the syllable task and the passage task.

Results of the VFR ratings
If two of the three evaluators showed a consensus on the resonance energy with a deviant focus of resonance, it was recorded as a 'yes (1).' As a result, none of the NH subjects showed any VFR, while the HI subjects were not perceived as having an inappropriate VFR.
Rating result of the VFR and rater concordance


Comparison of VFR ratings and nasalance types
Fisher's exact test was performed in order to verify the presence of differences between the VFR ratings for each nasalance type (normal nasalance, hyper-nasality, hypo-nasality and mixed nasality) (Table 11). The results revealed that no nasalance type had the same VFR (P<0.05).
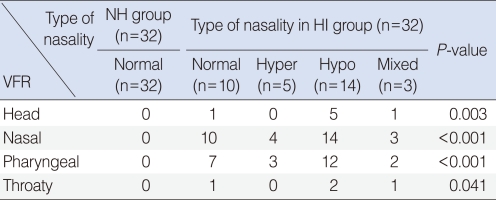
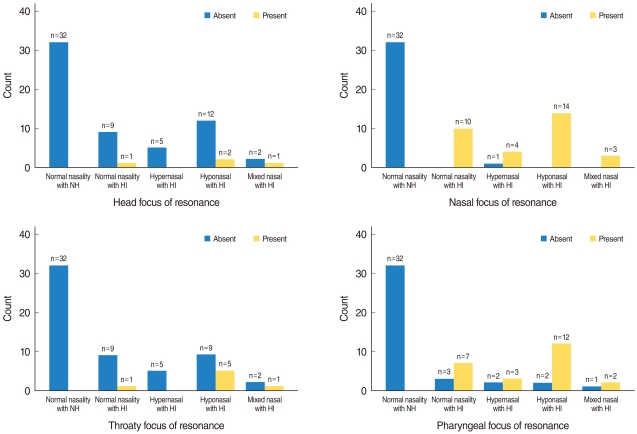
The focus of resonance and nasalance type are indicated in Fig. 2. VFR was perceived even in the subjects with normal nasalance levels. However, those with hyper-nasality did not show a head or throaty focus of resonance, and cases of hypo-nasality mostly demonstrated a nasal focus of resonance. Examples of a pharyngeal focus of resonance were observed in all types of nasalance.
Go to :
DISCUSSION
Comparison of the nasalance type of the NH and the HI groups
Speech characteristics of HI individuals with nasal resonance have been reported as hyper-nasality (8, 21), and some studies have mentioned that they demonstrate low nasalance levels (14). The present study similarly showed that the two groups demonstrated different aspects of nasalance scores based on the given task. When given an oral passage, the HI group demonstrated higher nasalance scores than the NH group, while showing lower nasalance scores than the NH group in the nasal passage and the nasal-oral passage. Such results imply that the groups show different nasalance levels depending on the characteristics of the speech task. Because of this, the speech characteristics of the HI group were thoroughly examined based on the nasalance scores. In the syllable task, the NH group showed no correlation between the nasalance scores for the stop consonant /appha/ and the nasal consonant /amma/. Velopharyngeal opening is not required for producing the stop consonant /appha/, while velopharyngeal closure is not required for the production of the nasal consonant /amma/. However, if the nasalance scores were high for producing the stop consonant /appha/ in HI individuals, the nasalance scores were similarly high in their production of the nasal consonant /amma/. Demonstrating a similar pattern, if the nasalance scores were low for /appha/, the nasalance scores were also low for /amma/. Such patterns in the HI group can be explained by velopharyngeal functions. If the nasalance score increased or decreased, regardless of the conditions of the velopharyngeal opening and closure, it seems that the velopharyngeal opening or closure was not affected by the phonetic context. Our results also demonstrated that both groups showed similar nasalance patterns in the passage tasks regardless of the phonetic context. The statistical significance shown in the NH group can actually be attributed to the individuals' unique speech characteristics. For instance, speech characteristics are distinctly different by gender and age. If an individual's voice pitch and resonance are within the limits of the normal range, their unique voice/speech sound should be accepted as a unique characteristic, rather than being viewed as pathological. In addition, nasality levels should also be considered normal as long as they do not go beyond the normal limits, even if there are tendencies of hyper-nasality or hypo-nasality. Nasality should not only be judged merely from the production of stop consonants, but should also be judged from the production of nasal consonants. Moreover, tendencies of hyper-nasality and hypo-nasality can be judged regardless of the phonetic context. However, nasal resonance has been evaluated only based on the segmental aspects. In general, hyper-nasality is defined as demonstrating a higher nasalance score than the average in the stop consonant task, and hypo-nasality is defined as demonstrating a lower than average nasalance score. However, an individual's nasality characteristic is not only limited to segmental aspects. Moreover, resonance is a physiological phenomenon that occurs within the resonance tract and cannot be completely explained as a phenomenon that is perceived in a specific phonetic context. Therefore, there are limitations in explaining resonance characteristics in terms of segmental aspects. The NH group's nasalance scores were overall higher than the standard in both the oral passage and the nasal passage tasks (Table 6). In other words, the samples of the NH group generally showed higher nasalance scores than those of the experimental group. However, the HI group had nasalance scores that were higher than the standard in the oral passage task and lower in the nasal passage task. This shows that a passage that requires velopharyngeal closure involved an opening to the nasal cavity, and when an opening was actually needed in the nasal passage task, the velopharynx was not fully closed. Moreover, the HI group's nasalance scores showed less consistency compared to that of the NH group, which also implies a limitation in judging them as hyper-nasal or hypo-nasal. Similar results were obtained from the comparison of the nasalance scores between the groups. The nasalance scores of the HI group were significantly higher in both the consonant syllable and passage tasks compared to those of the NH group, and scores were significantly lower in both the nasal syllable and passage tasks.
In conclusion, the methodology of judging the nasalance level in terms of segmental aspects, which categorizes the nasalance scores as high or low within a phonetic context, could not fully explain the resonance features of HI individuals. As a result, resonance features should be judged as part of an overall speech pattern. Prior to judging an individual's speech pattern as being normal or abnormal, it is crucial to observe whether the speech sound of an individual is due to their inherited characteristics (22).
In short, passage tasks that are a form of connected speech provided the most accurate information on the high and low nasalance levels compared to that of a normal hearing group, and it also provided information on how much of an individual's speech sound can be accepted as normal. In addition, the essential resonance problems of HI patients may be interpreted through the nasal-stop consonant coupling, which reflects the movements of the resonance cavity.
Comparison of the nasalance type based on VFR rating
As stated above, there were differences in the VFR ratings depending on the nasalance type. There were also cases of normal nasalance levels that showed deviant resonance levels based only on the VFR rating. Even in earlier studies regarding the hearing loss of prelingual HI subjects, the subjects demonstrated normal nasalance levels in standardized passage reading tasks even if they showed deviant resonance patterns (23). It was also concluded that a perceptual evaluation of the characteristics of hyper-nasality or hypo-nasality in an individual's speech was extremely difficult after merely listening to their speech (23). Although instrumental measurements of nasalance may be more efficient because they provide objective data, speech with excessive deviant resonance and sound characteristics may be limited from accurate measurement using this methodology. Some results from this study showed normal nasalance ranges, while having a perceptually deviant resonance problem. Moreover, it is not easy to rate the resonance in the nasal cavity alone. Thus, this study suggested the rating of nasalance in the whole resonance cavity at different focus areas, rather than limiting it to the resonance in the nasal cavity. Several experimental subjects showed a normal nasalance score but still showed deviant resonance aspects through the VFR rating (Fig. 2). These results were determined to be normal by the nasometer, but a perceptual evaluation of VFR revealed a deviant resonance pattern, indicating its abnormality. An individual's resonance cavity can be compared to a track that is blocked on one side, and the original speech sound is forced to go through the supraglottal space, therefore, passing through the vocal tract by creating a resonance energy that will be released through the opened cavities, such as the oral and nasal cavities. However, the cases of hyper-nasality showed nasalance patterns (Fig. 2) that were not evaluated through the head or throaty focus of resonance. Thus, cases where the VFR was in the head or the throat did not show a release of resonance energy, suggesting that the energy was focused in other areas within the resonance cavity. In cases where the nasal focus of resonance was also in the normal nasalance range, the resonance energy was sometimes perceived as being focused only in the nasal cavity. Cases of hypo-nasality were merely evaluated through the nasal focus of resonance. These results provide evidence that, in the nasal focus of resonance, the resonance energy remains focused in the nasal cavity without being released. This concept may explain why during a cul-de-sac resonance, the speech sound may be focused toward the front part of the nasal cavity, which may show a transformed aspect of hypo-nasality due to a muffled speech sound (24). When the resonance energy is focused in the nasal cavity like this, it can be perceived as a nasal focus of resonance in the VFR rating. Therefore, the nasal focus of resonance, in terms of VFR, is redefined as focused resonance energy in the nasal cavity, suggesting the possibility of hypo-nasality due to the blockage of the nasal cavity at one end.
In the pharyngeal focus of resonance ratings, a wide range of nasality levels (hyper-nasality, hypo-nasality and mixed nasality) was reported. The phenomenon of resonance energy being focused in the pharyngeal cavity implies that the tongue has been excessively pulled toward the posterior pharyngeal wall, which begins to contract and allows the resonance energy to be focused in the oropharyngeal cavity. This phenomenon can be explained through a different form of cul-de-sac resonance (25, 26). This form of cul-de-sac resonance is a type of pharyngeal resonance (27), oropharyngeal resonance (5), or oropharyngeal resonance (27), and can be perceived as an abnormal resonance pattern. When the resonance energy is focused at the posterior part of the oral cavity or the pharyngeal cavity, such as above, it is defined as a pharyngeal focus of resonance in terms of the VFR rating.
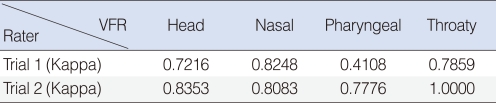
In the perceptual evaluation applying the definitions for VFR, the nasal focus of resonance and the pharyngeal focus of resonance showed a 50% agreement in the intra-rater reliability. Moreover, the inter-rater reliability during the first trial also showed a low agreement of 41%. Reasons for such low reliability were due to inaccurate explanations for defining the pharyngeal focus of resonance to the raters during the first trial of ratings; the pharyngeal focus of resonance was explained as a cul-de-sac resonance.
Reasons for a cul-de-sac resonance can be explained by first, the resonance energy remaining within the oropharyngeal cavity due to blockage of the entrance of the oral cavity and second, a velopharyngeal incompetency pushing the resonance energy toward the anterior section of the nasal cavity. Such reasons created confusion in precisely discriminating between the nasal focus of resonance and the pharyngeal focus of resonance. Despite the professional abilities of the three raters and that they were all knowledgeable in velopharyngeal incompetence, they faced confusion during the first trial of ratings when discriminating between the nasal focus of resonance and the pharyngeal focus of resonance. However, in the second trial of ratings, they understood the speech sound characteristics of the HI individuals, the concepts of cul-de-sac resonance, and were also able to categorize the muffled sections of the focus of resonance. Therefore, the confusion that they experienced during the first trial was clarified during the second trial, allowing them to clearly rate the resonance located in the pharyngeal cavity and eliminating the low intra-rater reliability in the subsequent trials. Using Fisher's exact test, it was verified that all raters understood that the cases of hypo-nasality were a nasal focus of resonance where the resonance energy could not be released. Thus, the definitions of nasal focus of resonance and pharyngeal focus of resonance were redefined in terms of VFR, and this method was efficient for rating the categorized resonance characteristics.
Using the results of the syllable tasks, as measured by the nasometer, hyper-nasality in HI individuals is explained by the tendency of the velopharyngeal opening, hypo-nasality can be explained due to the tendency of the velopharyngeal closure, and mixed nasality is demonstrated by an inappropriate coordination of the velopharyngeal function. Such explanations support the appropriateness of applying the deviant resonance characteristics of HI individuals. Rather than categorizing these characteristics as hyper-nasality or hypo-nasality, considering the aspects of velopharyngeal opening and closure may reflect the tendencies by specifically understanding a delayed velopharyngeal contact or a short-term weakness in velopharyngeal closure.
Nasalance scores are limited in explaining all resonance problems because they only provide information based on resonances in the nasal cavity and do not explain the phenomenon of the resonance energy being muffled in the resonance cavity. Such scores cannot explain the limitations in the velopharyngeal contact, which occur due to changes in size or shape of the resonance cavity. This study suggests perceptual ratings for VFR and defines each focus of resonance based on location. By applying such a rating method, it will be much easier to explain cases of hyper-nasality, hypo-nasality, mixed nasality and deviant resonance aspects, which are difficult to explain without a specific rating scale. It may also describe inappropriate VFR in terms of the speech characteristics of HI individuals since articulatory characteristics are insufficient for explaining such speech characteristics. Moreover, the descriptions of deviant resonance aspects could be clarified. Not only does this study evaluate the speech sound of an HI individual, but the study itself is significant in that it can be directly applied in the clinical field because it provides a new approach for evaluating articulatory problems and resonance problems.
Although this study only deals with VFR, it is necessary to briefly discuss 'horizontal focus of resonance,' as mentioned in Fig. 1. Since the function of articulation is considered more important than the resonance function when speaking of the oral cavity, the resonance function of the oral cavity may be omitted from the discussion. However, oral resonance is intimately related to tongue placement. When the location of the tongue is excessively protruded toward the front of the mouth, it shows a thin type, but when the tongue is excessively pulled toward the back, it shows a form of a cul-de-sac resonance (5). From this point of view, the 'horizontal focus of resonance' can be categorized into three concepts: frontal focus, central focus and back focus. There is a significant need for future studies based on the 'horizontal focus of resonance' rating in order to understand and describe the speech characteristics of HI individuals with resonance problems. Also, an objective approach will be necessary for accurately analyzing and understanding the 'horizontal focus of resonance.'
Go to :
 XML Download
XML Download