

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
The frontal recess (FR) is a narrow space in the shape of an inverted funnel behind the frontal beak (FB) and it is pneumatized by various anterior ethmoidal cells. The key to successful drainage of the frontal sinus is a complete understanding of the unique, complex anatomy of the FR of each individual in stereovision. However, previous studies of the pneumatization pattern of the FR have focused on Caucasian populations (1, 2) and there are few reports on the prevalence of frontal recess cells (FRCs) in Korean populations (3, 4).
The frontal sinus outflow tract (FSOT) is determined by the pneumatization pattern of the FRCs, attachment of the uncinate process, size of the FB, and shape of the skull base, and these anatomical factors vary among individuals and races (3, 5). Standard coronal and axial paranasal sinus (PNS) computed tomography (CT) images do not provide adequate information for reliable identification of the FSOT. Reconstructed parasagittal images better define the structural impingement of anterior ethmoid air cells on the FSOT and clearly show the length between the FB and the junction of the posterior table of the FS with the anterior skull base (6-8). They show the size of the agger nasi cell (ANC) and the anterior-to-posterior (A-P) length of the FI and FR, which is not detected on conventional PNS CT. Parasagittal images also provide more accurate information on the suprabullar cell (SBC) and frontal bullar cell (FBC) and the type of frontal cells (FCs) (7). To confidently build a three-dimensional picture of the anatomy of the FR and FSOT requires the simultaneous study of coronal, axial, and reconstructed parasagittal images.
This study evaluated the pneumatization pattern of the FR in a Korean population using axial and coronal PNS CT with reconstructed parasagittal images. Additionally, the correlation between the volume of the ANC and the A-P length of the FI and FR was determined.
Go to : 
MATERIALS AND METHODS
We identified patients from the primary endoscopic sinus surgery cases of one senior surgeon (HJR) treated over the past 4 yr. In total, 105 chronic rhinosinusitis patients who underwent preoperative PNS CT of the sinus with an image-guided protocol were identified. The ratio of males to females was 62:43, and the mean age was 46.2 yr (range, 19 to 62 yr).
The scans were performed using GE LightSpeed plus CT scanners (GE, Milwaukee, WI, USA) with 0.67 mm contiguous axial and coronal slices. Parasagittal images (0.6 mm thickness) were reformatted on the GE LightSpeed plus workstation system.
Two physicians (BNY and SSP) reviewed the preoperative routine PNS CT scans, separately. From the 210 sides, 20 sides in which it was difficult to identify the delicate structures of the FR due to the high soft tissue density in the FR or metal artifacts, were excluded. Ultimately, 190 sides examined in routine PNS CT were available for the final analysis.
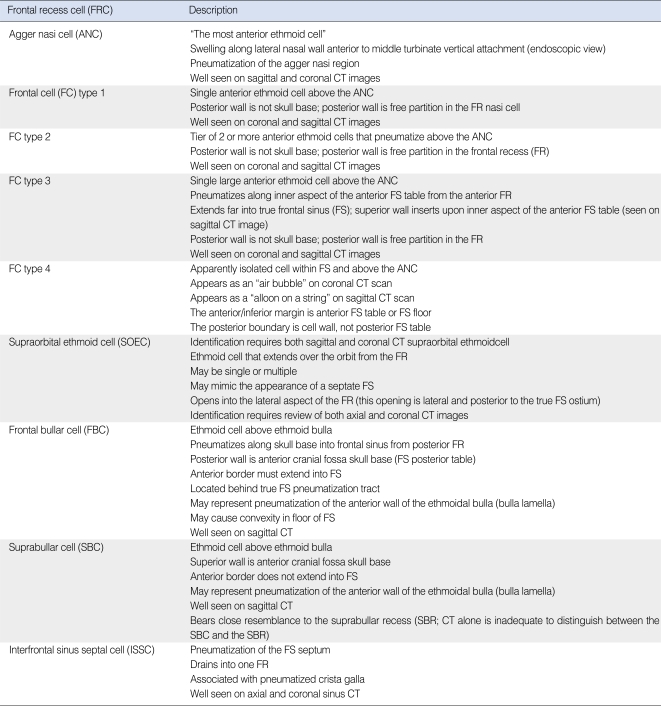
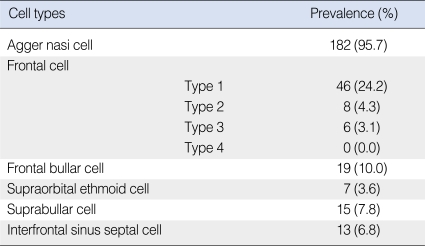
The frontoethmoidal cells were classified using the "frontal pneumatization pattern definitions and criteria" of Lee et al. (5) (Table 1). The thickness of the FB and the A-P length of the FI and FR were measured in the same parasagittal plane where the FB was the most prominent. The A-P length of the FI was defined as the shortest length between the most prominent portion of the FB and the posterior table of the FS. The A P length of the FR was defined as the length between the most prominent portion of the FB and the superior attachment of the ethmoidal bullar lamella (Figs. 1 and 2). The size of the ANC was measured in both the parasagittal and coronal planes. The volume of the ANC was defined as (the longest A-P diameter in the parasagittal plane)×(the longest vertical diameter in the parasagittal plane)×(the longest diameter from side to side in the coronal plane) (Fig. 3).
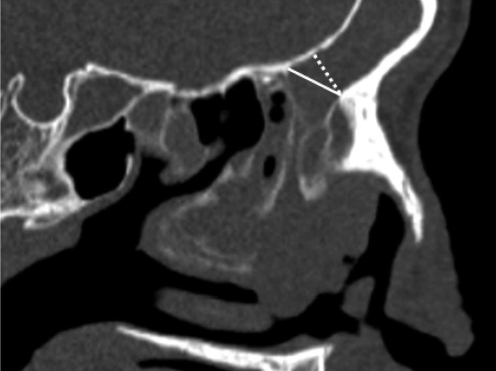 | Fig. 1A-P length of the frontal isthmus (FI; dotted line) and frontal recess (FR; solid line) on the parasagittal CT image. The anterior to posterior (A-P) length of the FI is the shortest length between the most prominent of the FB and the point of the posterior wall of the frontal sinus. The A-P length of the FR is the length between the most prominent of the FB and the superior attachment of ethmoid bullar lamella to the skull base.
|
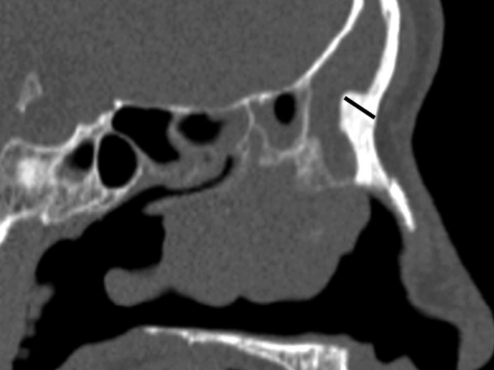 | Fig. 2Thickness of the frontal beak (FB) in prasagittal CT image. The thickness of the FB was measured on the parasagittal image where the FB showed the most prominent.
|
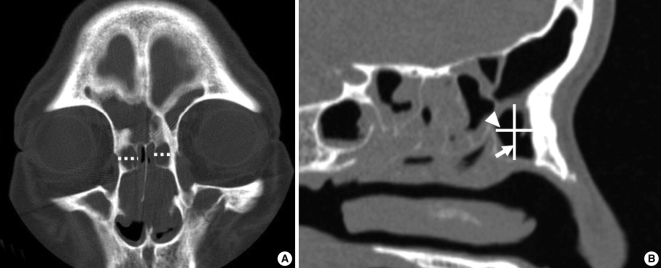 | Fig. 3Measure of the volume of the agger nasi cell (ANC) in coronal (A) and parasagittal (B) CT image. (A) The lateral diameter (dotted line) of the ANC was the longest diameter from side to side on the coronal image. (B) The longest anterior to posterior diameter (arrow head) and superior to inferior diameter (arrow) of the ANC were measured on the parasagittal image.
|
Pearson's correlation analysis (SPSS ver. 12.0, SPSS Inc., Chicago, IL, USA) was used to determine the relationship between the volume of the ANC and the A-P length of the FSOT.
Go to :
RESULTS
Prevalence of the FRCs
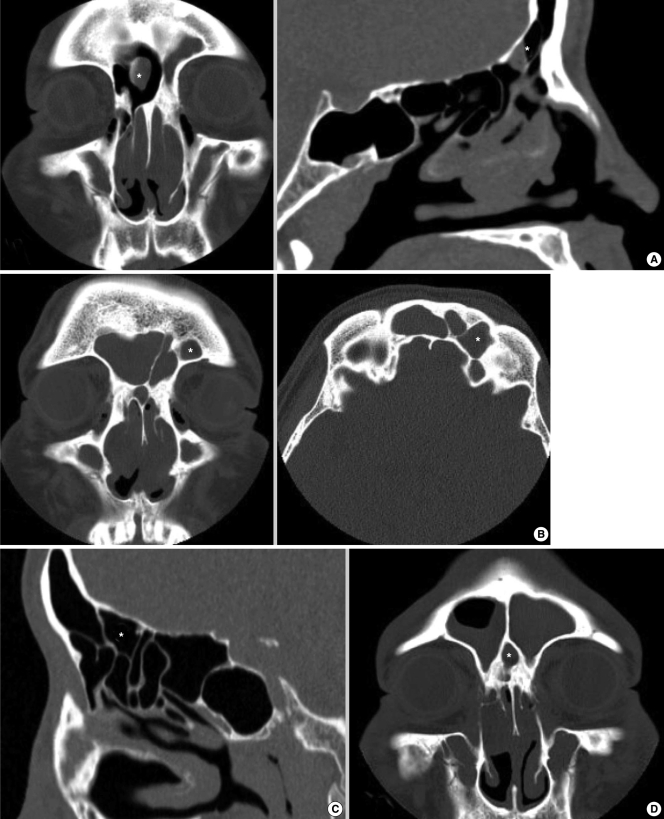
The ANC was observed in 182 sides (95.7%). FCs were noted in 60 sides (31.5%); the prevalences of FC types 1, 2, and 3 were 24.2% (46 sides), 4.2% (8 sides), 3.1% (6 sides), respectively (Fig. 4). Type 4 frontal cell was not identified. The prevalences of FBCs (Fig. 5A), suprabullar ethmoid cells (Fig. 5B), SBCs (Fig. 5C), and interfrontal sinus septal cells (ISSCs) (Fig. 5D) were 10% (19 sides), 3.6% (7 sides), 7.8% (15 sides), and 6.8% (13 sides), respectively (Table 2).
 | Fig. 4Frontal cells (FCs). CT image demonstrating FC type 1, 2 and 3. Each FC cell is shown as asterisk (*) marker at A (FC type 1), B (FC type 2) and C (FC type 3).
|
Anatomic measurements of the FSOT
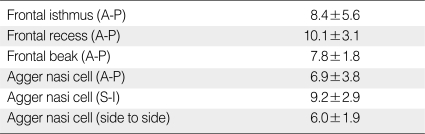
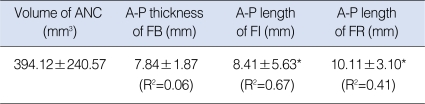
The FB was 7.8±1.8 mm thick. The A-P lengths of the FI and FR were 8.4±5.6 and 10.1±3.1 mm, respectively. The A-P, superior-to-inferior, and lateral diameters of the ANC were 6.94±3.84, 9.21±2.91, and 6.00±1.98 mm, respectively. The volume of the ANC averaged 394.1±240.5 mm3 (Table 3).
Correlation between the size of the ANCs and other anatomic measurements of the FR and/or FI
The volume of the ANC showed a moderate positive correlation with the A-P length of the FI (r=0.67) (P<0.001) and a weak positive correlation with the A-P length of the FR (r=0.41; P<0.001). However, there was no correlation between the volume of the ANC and the thickness of the FB (r=0.06) (Table 4).
Go to :
DISCUSSION
Incomplete removal of cells in the FR is the most common cause of failed endoscopic sinus surgery (9); thus, a comprehensive understanding of the FR anatomy is essential for a successful outcome. Advances in endoscopic visualization and high-resolution CT have facilitated a better understanding of the frontal recess anatomy. Recent reports have proposed that parasagittal CT images, reconstructed from high-resolution scans, 1 mm or less thick, are the important images that surgeons should use to convert two-dimensional CT images into three-dimensional anatomical pictures of the FR (6, 7). This study analyzed the pneumatization pattern of the FR and structural impingement of the FI and FR using axial and coronal PNS CT with reconstructed parasagittal images, which were reformatted from 0.65-mm axial and coronal slice CT images.
Many studies have sought to improve our understanding of the cells in the FR, and, currently, Kuhn's classification (5) is widely accepted. The prevalencea of ANCs (95.7%), SOEs (3.6%), and ISSCs (6.8%) we observed were consistent with two prior reports (3, 4) in Korean populations, while the prevalence of SBCs (7.8%) was lower than the report of Cho et al. (3)(39.5%). The most common frontal cell was the type 1 FC (31.5%), followed, in order, by types 2 and 3; the two reports had similar findings (3, 4). However, while Lee and Lee (4) observed type 4 FC in 2.0% of their cases, this was not confirmed in Cho et al. (3) or our series. This difference could be explained by differences in CT; Lee and Lee (4) used axial and coronal images without reconstructed parasagittal images. In this study, five cases of FBC were mistaken for FC4 in the coronal images. For example, Fig. 6 shows what appears to be a large FC4 in the left FS on the coronal CT (Fig. 6A), while the parasagittal scan (Fig. 6B) confirms that it is the FBC, extending into the FS. Thus, it is reasonable to suggest that the FC4 noted by Lee and Lee (4), could be the FBC mistaken for FC4 on conventional CT without reconstructed parasagittal images.
 | Fig. 6Frontal bullar cell (FBC). The coronal CT image (A) shows a large frontal cell (FC) type 4 in the left frontal sinus. However, in the parasagittal CT image (B), it is the FBC, pneumatizing along the skull base into the frontal sinus from the posterior frontal recess and extending the anterior border into the frontal sinus, mistaken for the FC type 4 on coronal image.
|
The course, width, and depth of the FSOT are determined by the pneumatization patterns of the anterior ethmoidal air cells and surrounding bony plates. The superior insertion of the uncinate between the lamina papyracea and middle turbinate is important for determining the course of the FSOT in the coronal plane (10).
Recently, the use of the ANC as an alternative landmark for the FR has been proposed (11). It becomes important to understand the interaction between the uncinate process and ANC to understand the anatomy of the FR. In most cases, the uncinate process attaches to the lamina papyracea; however, a large ANC may push the upward continuation of the uncinate medially, so that it becomes implanted in the skull base or middle turbinate (11).
Parasagittal images provide additional information about the relationship between the volume of the ANC and the A-P length of the FI and/or FR (2, 6, 7), demonstrating the cellular structures between the FB and superior attachment of the anterior wall of ethmoidal bullae (EB) (2, 7). In this study, we found a positive correlation between the volume of the ANC and the A-P length of the FI and FR. Initially, we postulated that a large ANC reduces the thickness of the FB and the absence of these cells resulted in a thick beak (11); consequently, we expected that a positive correlation between the volume of the ANC and the A-P length of the FI and/or FR could be explained by a reduction in the thickness of the FB with the increased volume of the ANC. However, we found no correlation between the volume of the ANC and the thickness of the FB. Our results actually indicate that a large ANC pushes the posterior table of the FS and superior attachment of the anterior wall of the EB posteriorly, increasing the A-P length of the FI and/or FR regardless of the thickness of the FB. The air space in FR represents potential space for a communication between FS and middle meatus created by surgical resection of the thin walls of FRCs. Therefore, Increasing pneumatization of the ANC, which is associated with a significant increment in the A-P length of the FI and FR, is believed to allow for wide surgical marsupialization by resection of the posterior/superior ANC wall and anterior/superior wall of the EB.
A limitation of this study is that our anatomic measurements were just of the cephalad margin of FR or the size of the frontal ostium, and they do not reflect the course, width, and depth of FSOT concretely. Nevertheless, The A-P length of FI and FR, which is only detected on the parasagital images, could be a one of the important information for building a 3-dimensional picture of the FSOT.
This study examined the pneumatization patterns of the FR in a Korean population using multiplanar PNS CT images. The ANC was seen in 96% and FCs in 32% of the cases. The prevalences of FC types 1, 2, and 3 were consistent with the findings of other studies, while FC type 4 was not identified here. It is thought that FC4 noted in other studies may have been FBC mistaken for FC4 on conventional CT without reconstructed parasagittal images. We also demonstrated that a larger volume of the ANC tended to be associated with an anteroposteriorly longer FI and FR.
Go to :
 XML Download
XML Download