

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Evidence exists that suggests that age-related hearing loss differs between men and women (1). The vast majority of studies measuring pure-tone thresholds in men and women in other countries have indicated that older men have substantially more high-frequency hearing loss and slightly less low-frequency hearing loss, as compared with older women (2-9). These sex differences in high-frequency thresholds often have been attributed to the likelihood that men have been exposed to more noise, at work and recreationally, than women. Some researchers have suggested that this sex difference is not totally due to changes in the cochlea. For example, women, tend to have smaller pinnae and ear canals, might produce greater physiological masking noise at low frequencies, and the coupling of the earphone used in audiometric testing may be less effective for women because of their smaller outer ears (10). However, age-related changes in middle-ear function, which could affect low-frequency thresholds, generally do not vary by gender (2). Also, hormonal differences between men and women also might explain some of the variance in hearing among the elderly (1). There is some evidence that innate differences between the sexes might affect the course of age-related hearing loss.
A few studies of age-related hearing loss have been conducted in Korea. However, reports of sex differences in hearing sensitivity of Koreans have been inconsistent. An early Korean study concluded that women have poorer hearing than men above 2 kHz (11). To date no sex difference in the incidence of presbycusis has been reported (12, 13). Other studies have reported better hearing sensitivity in women than in men (14-16).
The aim of our study was to establish sex- and age-specific reference ranges of hearing thresholds in normally aging Koreans and to identify age-related sex differences in pure-tone hearing thresholds.
Go to : 
MATERIALS AND METHODS
Subjects
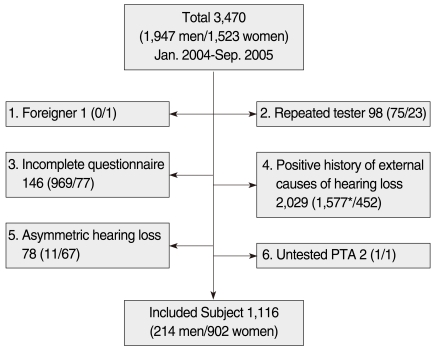
Subjects were clients who visited the Health Promotion Center, Daegu Fatima Hospital, Daegu, Korea between January 2004 and September 2005. Three thousand four hundred seventy subjects who submitted hearing questionnaires voluntarily were evaluated. Subjects included 1,947 men and 1,523 women.
Data were excluded for the present analyses if the subjects were foreigners, repeated testers, or did not complete the questionnaire. Also excluded were subjects with a positive history of otorrhea for any ear, usage of intravenous antibiotics, diuretics, and chemotherapeutic agent, head injury, job in a noisy environment, and military service. Any subjects with asymmetric hearing results were also excluded. More than a 15 dB difference at 0.5, 1, or 2 kHz was defined as asymmetric hearing. Fig. 1 depicts the number of subjects excluded. Many male subjects were excluded because of a history of military service. Finally, 214 men (11% of the initial male group) and 902 women (59% of initial females) were included. Ages ranged from 15 to 83 yr and the mean age of men and women were 47.6 and 46 yr, respectively.
When investigating "pure presbycusis," it is difficult to control external factors. For example, the Baltimore Longitudinal Study of Aging described subjects as "a relatively homogeneous group of well-educated, predominantly healthy, upper-middle-class, community dwelling men" (17). Since the clinical tests and procedures at our? Health Promotion Center were costly and not covered by medical insurance, it can be assumed that the subjects in this study were community dwelling people and not very sick or very poor, and, in this regard, were thought to be relatively homogeneous
Apparatus and procedures
As part of the health check, subjects completed continuous puretone audiologic testing followed by pulsed pure-tone testing. Hearing threshold levels were obtained at six frequencies (0.25, 0.5, 1, 2, 4, and 8 kHz) using a Beltone Model 112 Audiometer (Beltone Electronics Corporation, Chicago, IL, USA). Subjects were instructed to press a hand-held response key upon hearing a tone. Each ear was tested individually with pulsed tones presented through a TDH 50P headphone. The better ear was tested first or the right ear tested first if the subject indicated that hearing sensitivity was the same in both ears. During the audiometric tests, subjects were seated in a sound-treated chamber (Model IAC 400 A, Industrial Acoustics Company Inc., Bronx, NY, USA).
Testing began at 1 kHz, and continued successively to the higher test frequencies (2, 4, and 8 kHz) and then back to 1 kHz for a reliability check. The lower frequencies, 0.5 and 0.25 kHz, were presented last. Threshold levels were determined in 5-dB steps by three ascending and descending crossings. The audiometer was calibrated to audiometric zero in accordance with standards set by the American National Standards Institute (ANSI 1989).
Statistical methods
The average threshold of both ears for each subject expressed in dB HL (hearing level) at each of 6 frequencies was used for analyses.
Descriptive statistics were used to obtain sex- and age-specific reference levels for hearing thresholds.
In order to control for high-incidence causative factors of hearing loss other than age, subjects with a positive history of military service were excluded intentionally. In this study of an elderly population, there were more women than men, which is characteristic of the general population. For these two reasons, subjects were more likely to be women. Since age and sex effects were confounded, a one-way analysis of covariance (ANCOVA) was used to analyze the data to reveal sex differences after adjusting for age effects.
The slope of a linear regression line was used to calculate the rate of change in pure-tone threshold frequencies. Linear regression was chosen as the preferred procedure over nonlinear regression because linear regressions are easier to interpret and compare. Slope differences between men and women were also evaluated.
Go to :
RESULTS
Sex- and age-specific reference levels for hearing thresholds
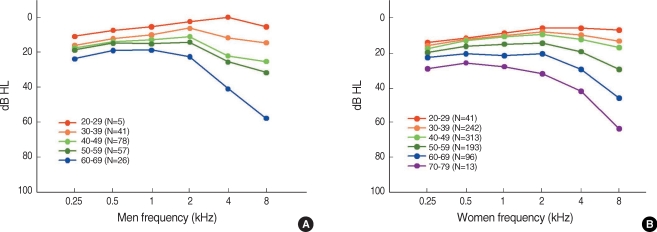
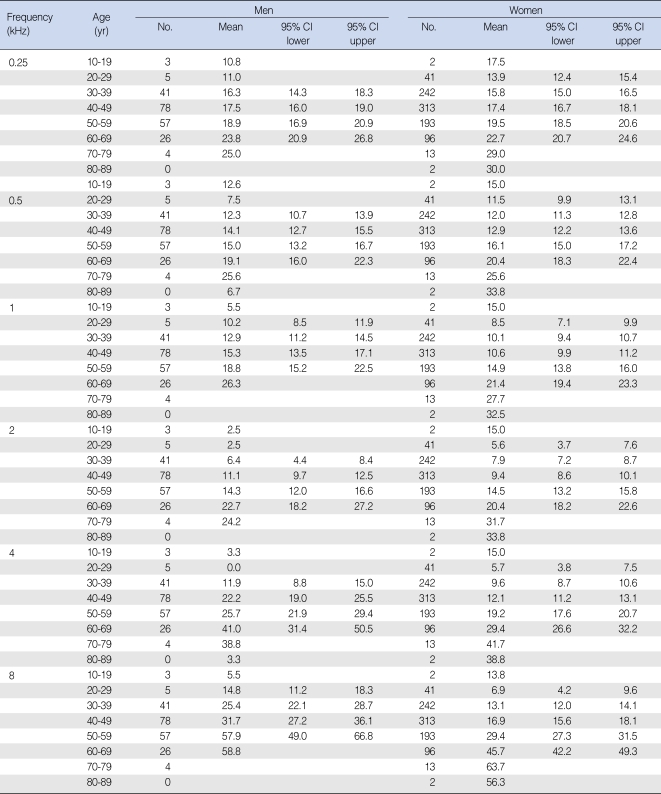
Average hearing thresholds increased with age in both men and women for all of the tested frequencies. Fig. 2 shows the audiogram of averaged thresholds for each decade of age for men and, separately, for women. The mean values and 95% confidence intervals of pure-tone threshold are summarized in Table 1.
Sex and age effects on hearing threshold
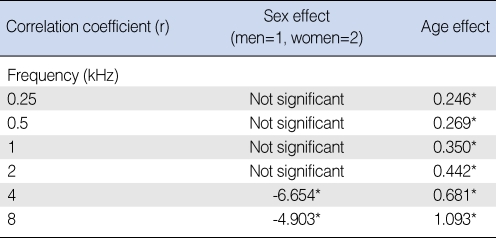
To determine sex effects without confounding age effects, ANCOVA of the rate of change in pure-tone thresholds was performed at each frequency, with sex as a grouping factor and age as a covariate. This approach allowed the age effect to be separated from the sex effect as age was held constant when the sex difference was measured. Results of the ANCOVA (Table 2) showed that the sex effect (state the actual effect) was significant at 4 and 8 kHz, whereas the age effect (state the age effect) was significant at all the tested frequencies.
Sex and frequency effects on rate of threshold change
The slope of a linear regression line was used to estimate the rate of change in pure-tone thresholds in the cross-sectional study. There was a significant correlation between age and hearing threshold for each frequency in men and women (P<0.001).
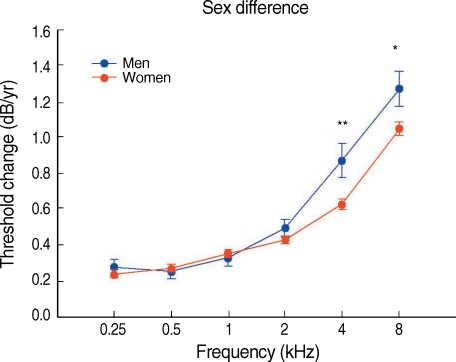
Fig. 3 shows the rate of change in pure-tone thresholds for men and women. The rate of change ranged from increases of 0.28 dB per year at 0.25 kHz to 1.27 dB per year at 8 kHz in men and from 0.24 dB per year at 0.25 kHz to 1.05 dB per year at 8 kHz in women. Men had a significantly greater rate of change at 4 and 8 kHz than women.
Go to :
DISCUSSION
Results indicated lower pure-tone thresholds for women than men at frequencies above 2 kHz. This finding is consistent with current knowledge of sex differences in hearing sensitivity, as reflected in cross-sectional studies (18-20). Until now, sex differences in rates of change in hearing thresholds were less clearly documented across the adult lifespan. A large study of pure-tone thresholds in the Framingham cohort suggested that the rate of change with age did not differ by sex (2). Additionally, previously published longitudinal analyses of age-related changes in hearing thresholds that included both men and women generally had less than 10 yr of follow-up, and only two or three repeated observations, and did not include individuals younger than 60 yr of age (2, 7, 21). Since hearing sensitivity begins to decline before age 60, as shown in this study (Fig. 2), it is necessary to evaluate the sex differences in the rates of change in hearing sensitivity throughout a broader lifespan. Further, this cross-sectional study revealed greater rates of threshold change in the higher frequencies, and that men have a significantly greater rate of change above 2 kHz than women have.
This study can not provide the underlying biological causes for sex differences in age-related hearing loss. However, it does provide new phenotypical data regarding hearing loss in adult Koreans.
It is well established that long term exposure to noise can affect the rate of change in hearing thresholds. Even though the subjects in this study were from relatively low-noise occupations and with little evidence of noise-induced hearing loss, innate differences between the sexes of unknown origin likely modulate the course of age-related hearing loss. For example, the influence of hormones such as estrogen, progesterone, and aldosterone remain to be evaluated as factors in the long-term effect of sex differences and invite further research.
In conclusion, our cross-sectional findings document sex differences in hearing levels and in age-related rates of threshold changes at 4 and 8 kHz. This study contributes to our understanding of age-related hearing loss in Koreans with little evidence of noise-induced hearing loss.
Go to :
 XML Download
XML Download