

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
A pleomorphic adenoma is the most common benign tumor in the salivary glands. It mainly occurs in the parotid gland and submandibular gland. If the tumor occurs in the minor salivary glands, the most common site is the palate, but this tumor can also occur in other sites include the upper lip, cheek, floor of the mouth, larynx and trachea (1). Although a pleomorphic adenoma is a benign tumor, it is considered to have metastatic potential. Only few cases of metastasizing pleomorphic adenoma have been reported in the medical literature, and all these cases were associated with previous incomplete surgery of a primary lesion (2). The frequent sites of metastases are the bone and lung (3). However, there are no reports of a benign pleomorphic adenoma that metastasized to the sphenoid sinus. We recently experienced a case of a metastasizing pleomorphic adenoma in the soft palate and the site of distant metastasis was the sphenoid sinus.
CASE REPORT
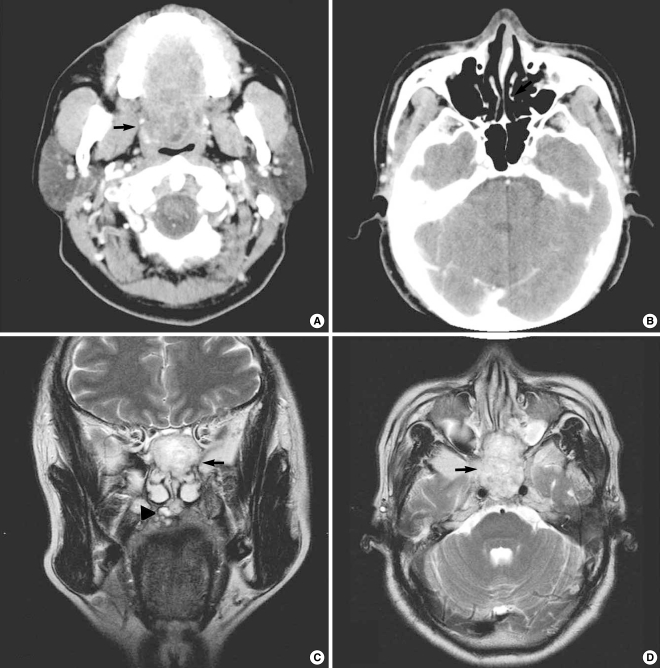
A 48-years old male patient visited the Department of Otorhinolaryn-gology due to a palpable mass in the soft palate for several years. On physical examination, a mass was palpated and it was round shaped, 4×4 cm sized, non-tender and fixed to the underlying soft tissue and it had a hard consistency. The mass had a smooth surface and the overlying mucosa was not involved. An anterior rhinoscopic examination revealed normal mucosa and there was no mass in both the nasal cavities. Following a fine needle aspiration biopsy, the mass of the soft palate was considered to be a pleomorphic adenoma. The computed tomographic scan showed a round shaped, 4×4 cm sized mass with well enhanced soft tissue density in the soft palate without invasion of the adjacent tissues (Fig. 1A), but the scan did not show a mass in any other region of the head and neck, including the sphenoid sinus (Fig. 1B). Therefore, the mass was resected and the defect of the soft palate was not continuous into the nasal cavity. The defect of the soft palate was treated by primary closure without reconstruction. Histopathological examination of the specimen revealed the presence of a benign pleomorphic adenoma.
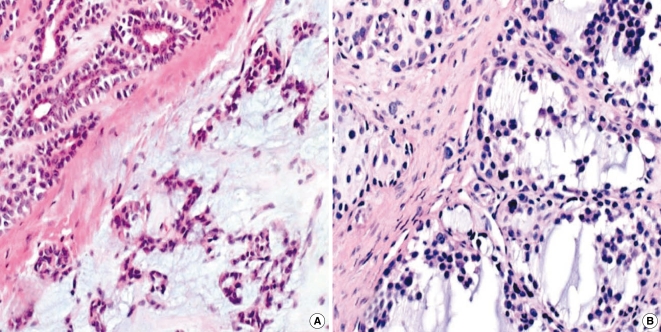
One year later, the patient visited the clinic due to a mass of the soft palate and diplopia that was present for the previous one month. On physical examination, a round shaped, 1×1 cm sized mass with a hard consistency and that was non-tender and fixed to the underlying soft tissue was seen. The mass had a smooth surface and the overlying mucosa was not involved. An anterior rhinoscopic examination revealed the normal overlying mucosa in both the nasal floors. The diplopia symptom was due to paralytic strabismus according to an examination performed by ophthalmologists. Computed tomography and magnetic resonance imaging were performed. The coronal and axial T2-weighted magnetic resonance imaging sequences showed a round shaped, 1×1 cm sized mass with high signal intensity at the soft palate without invasion of the adjacent tissues (Fig. 1C) and a large mass lesion with high signal intensity at the sphenoid sinus that apparently extended to the both posterior ethmoid sinuses (Fig. 1C, D). However, the sphenoid sinus had no abnormal lesion seen on the previous computed tomographic scan obtained one year previously (Fig. 1B). The mass of the soft palate was considered to be a pleomorphic adenoma based on a fine needle aspiration biopsy. In addition, a transnasal endoscopic biopsy was performed under local anesthesia for making the histological diagnosis of the mass in the sphenoid sinus, and a histopathological examination of the specimen revealed the presence of a benign pleomorphic adenoma without atypical cells (Fig. 2). However, treatment of the mass was not performed as the patient refused surgical treatment and follow-up.
DISCUSSION
A pleomorphic adenoma is a benign tumor, but it can metastasize, and especially when enucleation or incomplete excision is performed (2). A metastasizing pleomorphic adenoma is classified as a salivary gland tumor by the World Health Organization. For making the diagnosis, the primary site and metastatic site have the same histological characteristics of a pleomorphic adenoma that is indistinguishable from a typical pleomorphic adenoma and that is distinguished from a carcinosarcoma (true malignant mixed tumor) by the lack of malignant epithelial or mesenchymal components. In addition, conversion of a pleomorphic adenoma to a malignant tumor should be excluded (2, 4). Likewise, the histopathological findings of the present case indicated that the tumors of the soft palate and the sphenoid sinus were typical benign pleomorphic adenomas without conversion to a malignancy.
Most cases of a metastasizing pleomorphic adenoma are known to occur after surgical excision or local recurrence. The most frequent site of a metastasizing pleomorphic adenoma is the parotid gland, where complete excision is difficult due to the critical anatomical problems such as the presence of the facial nerve, followed by the presence of the submandibular gland and the minor salivary glands. The most common site of a metastasizing pleomorphic adenoma in the minor salivary glands is the palate (2). The time interval between the diagnosis of a primary pleomorphic adenoma and metastasis has ranged from three to 22 years (4). In this case, the interval between surgery for the primary pleomorphic adenoma and the distant metastasis was one year, and this represents a very short interval as compared with that of the previous reported cases (2-5). The common sites of metastasis of a benign pleomorphic adenoma are mainly the bone and lung, and the tumor less commonly metastasizes to the lymph nodes, oral cavity, pharynx, skin, liver, retroperitoneum, kidney, paranasal sinus and central nervous system (2, 3). Within the head and neck, a frequent site of metastasis of a benign pleomorphic adenoma is a cervical lymph node, but the paranasal sinuses represent a very rare site of metastasis; only two cases of metastases to the maxillary sinus from the palate and the parotid gland have been reported in English-language clinical literature between 1953 and 2006 (2, 3). To the best of our knowledge, this is the first case report of a benign pleomorphic adenoma of the soft palate that metastasized to the sphenoid sinus.
The mechanism for the metastatic behavior of a metastasizing pleomorphic adenoma is not clear. It has been reported that rupture of the capsule on a benign pleomorphic adenoma frequently occurs during enucleation or incomplete excision. Along the ruptured site, the myxoid material in the tumor spreads to the surrounding damaged soft tissue and distant sites through a venous or lymphatic route (3, 5). In the present case, it was thought that the benign pleomorphic adenoma of the soft palate was a local recurrence due to incomplete excision at the time of initial surgery and the benign pleomorphic adenoma of the sphenoid sinus was a distant metastasis through the blood circulation.
The metastatic site of a benign pleomorphic adenoma has the characteristics of slow growth and long-term persistence (3, 4). However, the tumor sometimes is clinically malignant and it can cause a fatal condition. Therefore, the treatment of choice for a metastasizing benign pleomorphic adenoma is complete surgical excision. Recurrence is rare after complete removal and the prognosis is excellent (3-5). However, chemotherapy or radiotherapy has still not been demonstrated to be useful for managing primary and metastatic lesions, and to prevent further recurrence and metastasis for a metastasizing pleomorphic adenoma (4).
To summarize, although a metastasizing pleomorphic adenoma is rarely encountered, the head and neck surgeon should be aware that meticulous resection is necessary at the initial surgery for preventing distant metastasis and close postoperative follow-up should be done for detecting possible metastasis.
 XML Download
XML Download