

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
The obstructive sleep apnea syndrome (OSAS) is characterized by periods of breathing cessation and reduced breathing. Many studies have suggested that OSAS elevates the risk for cardiovascular morbidities such as systemic hypertension, coronary heart disease, atherosclerosis and stroke independently of other known risk factors (1-5). The presence of repetitive nocturnal hypoxemia, negative intrathoracic pressure and arousal states in OSAS patients are associated with the activation of sympathetic, hormonal, thrombotic, and metabolic factors (6). Although the precise mechanisms have not yet been elucidated, one possible etiology may include the pathophysiology of endothelial dysfunction (6). In addition, inflammatory processes may be associated with OSAS which may act as potential mediators of cardiovascular morbidities in these patients (4).
There are variable biomarkers such as white blood cell count, serum interleukin-6, fibrinogen, C-reactive protein (CRP), albumin concentration and erythrocyte sedimentation rate (ESR) that are indices of systemic inflammation (7). Recent interest has been focused on the association between circulating inflammatory biomarkers and the severity of OSAS as well as the prediction of cardiovascular events in patients with OSAS (8). Furthermore, patients with OSAS and elevated plasma CRP levels have shown a reduction in their levels of CRP after treatment with nasal continuous positive airway pressure (9).
The ESR, which measures the tendency of red blood cells to aggregate, is a widely used laboratory test. ESR has been reported to be elevated in many of the acute and chronic diseases characterized by tissue necrosis and inflammation (10). The normal range of ESR is 0-10 mm/hr for men and 0-15 mm/hr for women. However, the upper limit of the normal range increases with advancing age and obesity (7). A recent study has reported that after adjusting for gender and hematocrit, ESR was directly associated with coronary atherosclerosis (7). Although ESR is a cheap and widely used test and has a possible predictive value for cardiovascular disease (11), there have been few reports on the relationship between the plasma ESR level and the severity of hypoxemia or the risk for cardiovascular events in OSAS patients.
The aim of this study was to determine the relationship between the plasma ESR level and the demographic data or polysomnographic variables of OSAS patients and to examine the role of obesity in OSAS patients. In particular, we evaluated the relationship between the duration of nocturnal oxygen desaturation and the plasma ESR level in the study group and analyzed the results in obese and non-obese patients.
MATERIALS AND METHODS
Seventy-two patients (age range, 24 to 67 yr; mean age, 45.2 yr) who were diagnosed with OSAS by polysomnography and referred to the Department of Otorhinolaryngology between July and December of 2005 were enrolled in this study. Patients who had a medical history of cardiovascular disease (cardiac failure, angina pectoris, myocardial infarction, or stroke), inflammatory diseases (chronic sinusitis or chronic renal failure), transplantation or other surgery and a previous history of therapy using continuous positive airway pressure (CPAP) were excluded from the study.
The study was approved by the Institutional Ethics Committee at our hospital, and informed consent was obtained from all patients. Information on smoking habits, alcohol consumption, the use of antihypertensive drugs, and a history of diabetes was obtained from a self-administrated questionnaire. In addition, all patients received the Epworth Sleepiness Scale (ESS) test which evaluates subjective daytime somnolence. Blood samples were collected to measure the plasma ESR level (mm/hr) using the Test1 kit (ALIFAX SPA, Padova, Italy). The body mass index (BMI) was calculated, and patients were categorized into obese (BMI ≥25) and non-obese (BMI <25) groups. All patients received overnight polysomnography in order to evaluate the objective somnolence. Polysomnography was performed using an Alice3 (Healthdyne Technologies®, Marietta, GA, USA) recorder. Electroencephalogram (C3-A2 and C4-A1), left and right electro-oculograms, electrocardiogram, chin and anterior tibialis electromyograms, abdominal and thoracic movements by inductive plethysmography, nasal/oral airflow, and oxygen saturation by pulse oxymetry (SpO2) were monitored during the test. Apnea was defined as the cessation of breathing for at least 10 sec, and hypopnea was defined as a decrease in airflow of at least 50% or a decrease in SpO2 of at least 4%, compared to the baseline. The apnea-hypopnea index (AHI), apnea index (AI), lowest saturation, and the percentage of time spent at a SpO2 below 90% (sleep time at SpO2 below 90%/total sleep time ×100) were obtained.
Statistical analyses were performed using SPSS ver. 11.5 (SPSS Inc., Chicago, IL, USA). The Student t test was used to determine the relationship between the plasma ESR level and the demographic data, such as gender, or a history of smoking, alcohol, diabetes mellitus, and hypertension. Simple and multiple linear regression analyses were used to statistically determine the relationship between the plasma ESR level and the other polysomnographic variables. The parameters included age, BMI, AHI, AI, lowest saturation, and the percentage of the time spent at a SpO2 below 90%. The significance level was set at P<0.05 in all analyses.
RESULTS
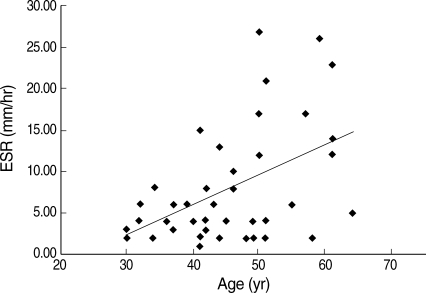
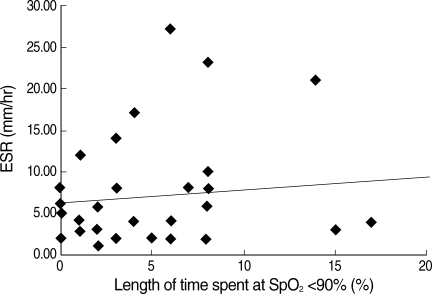
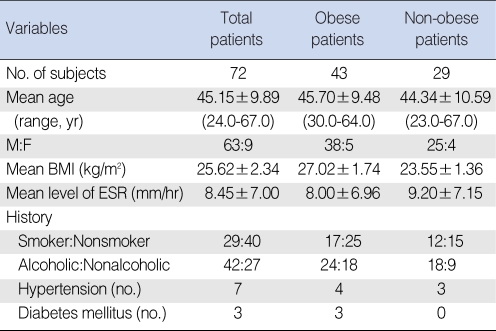
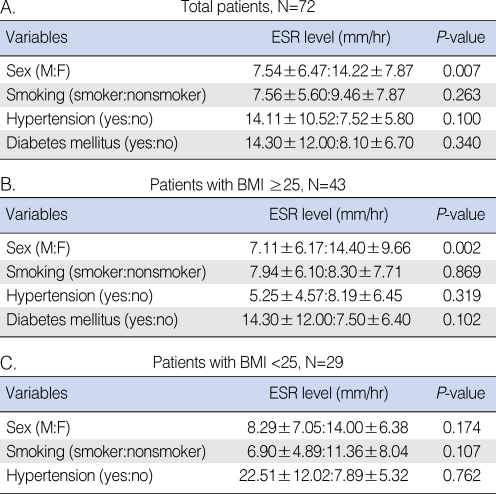
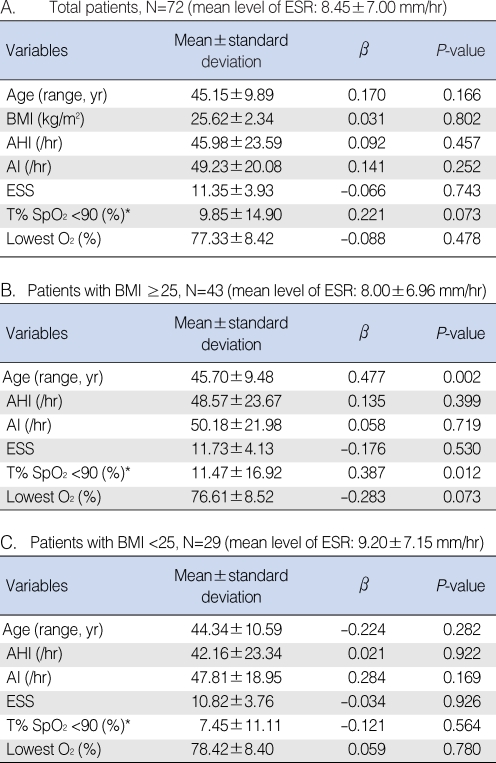
The clinical characteristics of the study population are summarized in Table 1. The mean ESR level was 8.45±7.00 for all patients. The plasma ESR level was significantly higher in female patients than in male patients (median, 14.22 ver. 7.54; P=0.007). For all patients, there was no significant correlation between the plasma ESR level and the polysomnographic variables or the demographic data except for gender (Tables 2, 3). However in the obese group, there was a significant correlation between the plasma ESR levels and the percentage of time spent at a SpO2 below 90% (BMI ≥25, n=43, P=0.012; correlation coefficient, R2=0.148, β=0.387; 95% confidence interval, 0.036-0.276) (Fig. 1). The mean ESR level was 8.00±6.96, and the mean percentage of time spent at a SpO2 below 90% was 11.47±16.92% in the obese group. Other polysomnographic variables such as AHI, AI, and the lowest O2 saturation revealed no significant correlation with the plasma ESR levels. In addition, the mean age of the obese group was 45.70±9.48 yr which was positively correlated with the plasma ESR level (P=0.002; R2=0.205, correlation coefficient, β=0.477; 95% confidence interval, 0.150-0.577) (Fig. 2). To investigate the independent factors associated with increased ESR levels, we performed a multivariate analysis for age, gender, and all other studied variables. In our multivariate analysis, the plasma ESR level was associated only with the percentage of time spent at a SpO2 below 90% (P=0.007; correlation coefficient, β=0.369; 95% confidence interval, 0.043-0.254) and age (P=0.001; correlation coefficient, β=0.463; 95% confidence interval, 0.153-0.552) in the obese group. In the non-obese group, there was no significant correlation between the plasma ESR level and the demographic data or the polysomnographic variables.
DISCUSSION
Silvestrini et al. (12) first demonstrated that male patients with severe OSAS have an increased risk for carotid atherosclerosis independent of any other concurrent, confirmed, vascular risk factors. There is increasing evidence for the existence of a causal relationship between OSAS and cerebrovascular disease (6, 13). Many studies have documented that the functional outcome of OSA patients is poorer if they had a recent stroke or transient ischemic attack, and the mortality rate at 1-yr follow-up was higher than in stroke patients without OSAS (14-18). Although the explanations for these findings are incomplete, it has been suggested that a combination of sleep deprivation and hypoxemia may aggravate the disease process. In addition, a recent polysomnographic study reported that patients with the OSAS have more severe plaque formation than patients who do not have OSAS (19).
A recent hospital-based study with a large population of patients showed that inflammatory markers such as CRP, WBC count and fibrinogen tend to correlate with obesity, central distribution of body fat, higher blood pressure, hyperglycemia, lower HDL-cholesterol, and hyperinsulinemia which are all risk factors for cardiovascular disease such as atherosclerosis (20). In addition, CRP has been suggested to be a risk factor for a myocardial infarction (21). To date, a few prospective population-based studies have shown the long-term predictive value of ESR in relation to the development of cardiovascular disease (10). The Stockholm Prospective Study Group demonstrated that ESR was an independent risk factor for myocardial infarction (22); in addition, another study suggested that ESR predicts events associated with the development of ischemic heart disease (23).
A correlation between inflammatory markers, especially CRP, and the severity of OSAS has been reported. Shamsuzzaman et al. (6) found that in 22 newly diagnosed patients with OSAS, there was a significant increase in CRP levels compared with 20 normal subjects, and they concluded that the magnitude of the CRP elevation was significantly associated to the severity of OSAS. However, there have been few reports on the correlation between the severity of OSAS and plasma ESR levels which is an important inflammatory marker. ESR, which is an indicator of red cell aggregation and thus blood viscosity, is a routine laboratory test widely used to screen for the presence of inflammation and for the initial diagnosis and follow-up of chronic diseases (7). Physiologically, ESR relates to both the underlying blood rheology and the inflammatory responses (24). A few studies have proposed that ESR is an independent predictor of coronary heart disease (24).
We found a positive correlation between the plasma ESR level and the severity of OSAS which was assessed by the percentage of time spent at a SpO2 below 90% in obese patients, independent of the smoking status, alcohol consumption and the presence of hypertension or diabetes mellitus. Since there is a tendency for the plasma ESR level to increase with adiposity, we divided the patients into obese and non-obese groups to eliminate this confounding factor. There were no positive correlations with ESR in the non-obese group.
In this study, we evaluated the correlation between the percentage of the time spent at a SpO2 below 90% and the plasma ESR level by pulse oxymetry. The advantage of pulse oxymetry is that it reflects only significant desaturation which is an objective test, whereas there is a large variation in other polysomnographic measurements such as AHI between readers. Based on the results that there is a significant correlation between the ESR level and the time spent at a SpO2 below 90% and whereas there was no significant correlation between the ESR level and other polysomnographic variables, it is conceivable that the desaturation time may be related to the risk for cardiovascular disease. In addition, Nieto et al. (25) reported that after controlling for the main potential confounders, high levels of AHI or time at sleep with below 90% oxygen saturation was associated to greater odds ratios for hypertension. Furthermore, Hoffstein et al found significantly increased hematocrit levels when contrasting patients in the lowest and highest quartiles for percent of total sleep time spent at oxygen saturation <85% (26). Moreover, our multivariate analysis showed that the ESR levels were higher in women compared to men and increased with advancing age. Recent studies have shown that gender may affect the upper limit of the normal ESR level and that the ESR level is slightly higher in women (0-15 mm/hr) than in men (0-10 mm/hr) (7).
One limitation of this study is its small sample size and lack of female subjects. Thus, further studies with a larger sample size of female subjects are needed to confirm the correlation between the ESR levels and the female gender. The results of this study suggest that there may be a positive association between the plasma ESR level and nocturnal oxygen desaturation in obese patients. The duration of deoxygenation in OSAS patients may be associated with the ESR level which is an independent predictor of cardiovascular disease.
 XML Download
XML Download