

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Many studies have emphasized the importance of early cochlear implantation for children with profound hearing loss (1-7). These studies have proven that children who are implanted during younger ages achieve higher scores on several auditory performance and language tests after a given time of implant use. Cheng et al. (3) performed a meta-analysis on the effects of age at the time of implantation and the causes of profound hearing loss on the performance of post operative speech perception. They concluded that the age at the time of implantation has a significant effect, while the cause of the profound hearing loss does not. In addition, they found that the receptive benefit in spoken language continues to improve even after 3 yr with no plateau.
As a result of the prior studies, it appears that there is a period of time when the brain has the plasticity to adapt the auditory information associated with meaningful auditory performance and language (8, 9). However, there is debate concerning the exact limits of this period for auditory performance and language development. This is particularly relevant to the timing of cochlear implantation. Some researchers have advocated that cochlear implants should be provided earlier than 5-6 yr of age (10, 11), while others suggest 3 yr of age as the proper time for implantation (12, 13). The general consensus is that children have the best opportunity to learn language during the first 5 yr of life (5). However, whether earlier implantation, even within this critical period, has additional benefit requires further study. Actually, one study has reported that they have failed to find additional benefits for earlier implantation within the critical period for language development (4). But this point should be reevaluated since there were some shortcomings in that particular study. For example, the patients implanted under the age of 2 were not included.
Another notable point is that many prior studies have neglected to consider the influence of the maturation/development of the studied children. Kileny et al. (5) gave consideration to this point and they attempted to control for the effects of maturation/development by comparing the speech perception performance between the patients of the same age, but who received their cochlear implants at different ages. Although this was a fresh attempt to answer some questions about this issue, they failed to differentiate the effect of the length of implant use from the age at implantation. That is, although the children who were implanted earlier showed a better performance, Kileny et al. (5) could not differentiate whether the benefits were due to the early implantation or to a longer duration of implant use. Nonetheless, the differentiation of the benefits from maturation/development from those due to early cochlear implantation is important for determining the best age to provide the implants. Therefore, the objective of this study was to compare the long-term auditory performance and language skills according to the age of cochlear implantation in a Korean population. We especially tried to separate the effect of maturation/development from that of the age at the time of implantation.
MATERIALS AND METHODS
Subjects
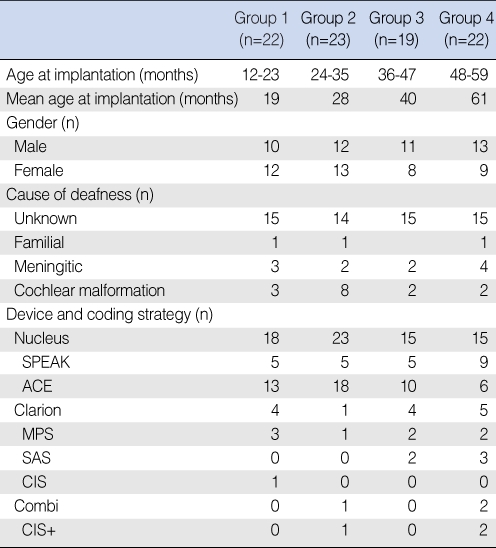
From 1995 through 2003, 86 pre-lingual deaf children with profound hearing loss and who underwent cochlear implantation before the age of 6 and who had been followed for more than 3 yr were enrolled in this study. Those children with mental retardation and severe cochlear malformations such as a common cavity or cochlear and vestibular aplasia were excluded from the study. The children were grouped by age at the time of implantation: group 1 included the children who were younger than 2 yr (n=22), group 2 included the children who were 2-3 yr of age (n=23); group 3 included the children who were 3-4 yr of age (n=19) and group 4 included the children who were 4-6 yr of age (n=22). Most of the children (n=55) had the diagnosis of profound hearing loss of an unknown etiology, although there were 11 patients who had a history of meningitis before the diagnosis of hearing loss. The demographic data is presented in Table 1. There were 15 children with minor inner ear anomalies such as Mondini dysplasia or an enlarged vestibular aqueduct. The distribution of these children was three in group 1, eight in group 2, two in group 3 and two in group 4. We did not exclude the patients with minor inner ear anomalies because there is no definite evidence that these anomalies are associated with the hearing prognosis (14).
Auditory performance and language assessment
Although a battery of tests, including the Categories of Auditory Performance (CAP), the Infant Toddler Meaningful Auditory Integration Scale, the Central Institute for the Deaf , the Phonemically Balanced words and the Korean Picture Vocabulary Test (K-PVT) were evaluated before and after cochlear implantation at our institute, only the CAP score and K-PVT were analyzed for this study. The CAP and K-PVT were selected because the CAP is a generally accepted tool for evaluating the auditory performance and the K-PVT reflects the speech perception abilities. These two tests can also be used from a very young age.
The CAP is a global outcome measure of auditory abilities (15, 16). It includes a nonlinear, hierarchical scale on which children's developing auditory abilities can be rated in eight categories of increasing difficulty. The categories are as follows:
-
0=no awareness of environmental sound
1=awareness of environmental sounds2=responds to speech sounds3=recognizes environmental sounds4=discriminates at least two speech sounds5=understands common phrases without lip reading6=understands conversation without lip reading with a familiar talker7=can use the telephone with a familiar talker
The K-PVT is a test that evaluates the receptive vocabulary as compared with the child's chronological age in the normal hearing population (17). There are four pictures to a page, and each is numbered. The examiner states a word describing one of the pictures and he/she asks the child to point to or tell the examiner the picture that the word describes. A Korean language version was introduced by Kim et al. (17) in 1995; it is similar to the Peabody picture vocabulary test-revision (18), yet the vocabulary and pictures are different and optimized for the Korean language. It can be used from the age of 24 months through 8 yr and 11 months and the results are expressed in an absolute score and the developmental language age is expressed in years, as well as in a percentile score as compared with the child's chronological age in the normal hearing population. It is scored from 0 to 112. In order to emphasize the effect of the age at implantation and to diminish the maturation/development effects, the postoperative score improvement compared to the preoperative score was used as the primary outcome measure.
Operation and programming
All the children underwent the conventional facial recess approach for the implantation and all of the electrodes were successfully inserted. Among the 84 patients, 71 patients were implanted with a Nucleus device (Cochlear Ltd, Sydney, Australia) while 14 and 3 patients were implanted with a Clarion device (Advanced Bionics Corp, Valencia, CA, USA) and a Combi device (Med-El, Innsbruck, Austria) respectively. All of the children underwent programming 1 month after surgery. The ACE coding strategy was used in 47 patients and the SPEAK coding strategy was used in 24 patients. Various coding strategies were used for the Clarion amd Combi devices. The exact coding strategies are mentioned in Table 1.
Statistical analysis
The repeated measures analysis of variance (RM ANOVA) was used. A P-value<0.05 was considered statistically significant. The study protocol was approved by the ethical committee of Seoul National University Hospital and informed consent was obtained from all the participants or their guardians.
RESULTS
CAP score
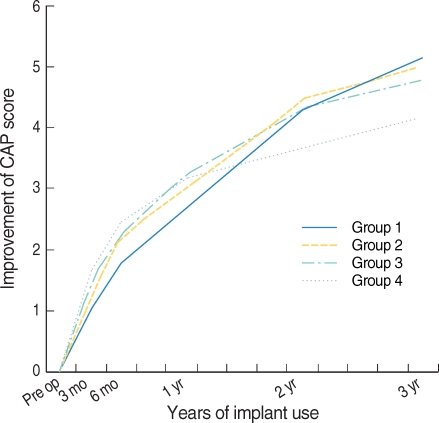
Fig. 1 illustrates that group 4 appeared to have poor improvement scores after 1-3 yr. However, the RM ANOVA for the CAP revealed a significant effect for time (P<0.001) and a non-significant effect for group (P=0.773). That is, the CAP score continued to improve with time, but the improvement of the CAP score was not significantly different among the groups. The group×time interaction was significant (P=0.002). That is, the younger age groups showed a more rapid improvement (steeper inclination).
K-PVT score
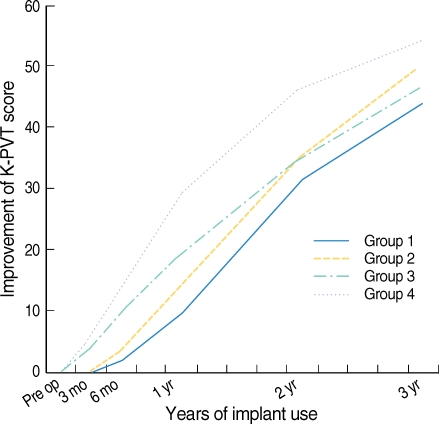
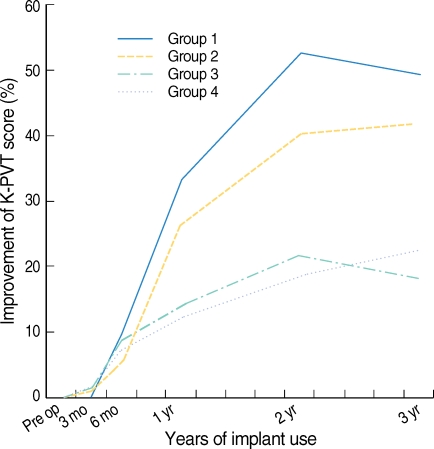
Group 4 appeared to have the best results when the improvement in the K-PVT scores was directly compared among the groups (Fig. 2). This is likely due to a maturation/development effect. In order to separate the effect of age at the time of implantation, the results were readjusted to percentile scores of their chronological age (Fig. 3). The RM ANOVA for the K-PVT percentile scores revealed a significant effect of time (P<0.001) and a significant effect for the group (P=0.037). That is, the improvement in the K-PVT percentile scores continued to increase over time and the improvement of the K-PVT percentile score was significantly higher for the group implanted at a younger age. The 50th percentile is the mean of the normal hearing population. Compared to the normal hearing population, the children implanted under 2 yr of age were able to catch up with the normal hearing population after 2-3 yr of implant use. By contrast, the children implanted after 3 yr of age only achieved a score at the 20th percentile of the normal hearing population, and this poor score was maintained. In addition, the group×time interaction was significant (P=0.004). That is, the younger age groups showed more rapid improvement (steeper inclination).
DISCUSSION
The CAP score has many advantages, and the inter-observer reliability of the CAP has been formally confirmed (16). Rather than evaluating specific speech perception abilities, this method evaluates the general and comprehensive functions of hearing in children (19). Differences in language competency are not critical for performing the tasks of this test and it can be used for children of any age (19). However, the outcome results are expressed in only seven ordinal scales. This may result in lower statistical power, which means that a large difference may be presented as a small difference due to the low resolution of the outcome measures. In addition, the CAP has no reference value for subjects with normal hearing. Consequently, it is difficult to separate the benefits that are due to the age at implantation from those associated with maturation/development. It seems that for this reason, we failed to show a significant difference for improvements in the CAP scores according to the age at implantation. It is likely that the demonstrated differences in auditory performance and language skill were diminished in our results by the factors we have mentioned above. It would be very helpful if we had a chronological reference value for the CAP scores based on the normal hearing population. Actually, one previous study tried to compare the post implantation CAP score with that of the normal hearing population (19). Based on 84 normal hearing subjects, the investigators developed a normal reference for the CAP score according to age. The mean CAP score for 12 months was a CAP of 2, and that for 18, 24, and 30 months was 5, 6, and 7, respectively. Although the number of subjects was not large enough to represent the entire normal hearing population, they were able to show that a larger proportion of patients with earlier cochlear implantation reached normal CAP scores for their age. If the investigators had directly compared the CAP score results among the study groups, as we did, they would have also had difficulty proving the benefit of early implantation. Therefore, establishing a reference value for the CAP scores, based on the normal hearing population, seems important for the ability to separate the effects of maturation/development from those of the age at implantation.
Cheng et al. (3) reported that speech perception performance continues to improve without a plateau even three years after cochlear implantation. However, according to the results of our study, the percentile of receptive language abilities reached a plateau after 2-3 yr. Although a definite plateau was not found in groups 2 and 4, the trends of the increments progressively diminished, which implied that the graph would soon reach a plateau. This does not mean that the auditory performance stops improving after 2-3 yr of implantation. It means that after 2-3 yr, the speech and language performance of the child reaches a certain stationary level, as compared to that of the children of the same age. For example, Fig. 2 shows that the performance keeps on improving even after 2 yr. However, it seems that after 2 yr, the natural maturation/development of the child becomes a more important factor for improvement since the relative percentile score was stationary. In other words, if the child received the cochlear implant at an early enough age, then the child's performance will be able to catch up with the maturation/developmental process of the normal hearing population after 2-3 yr. By contrast, the children implanted after 3 yr will only catch up to approximately the 20th percentile of normal even after 2-3 yr and they will probably maintain this level thereafter. It should also be noted that not every patient reached a plateau after 2-3 yr. There were 12 patients in this study who did not reach a plateau. But for the majority of children (74 patients), it seems true that the percentile of receptive language abilities reach a plateau after 2-3 yr.
The importance of the critical period of speech and language development has been emphasized in many reports, and recent studies have suggested that early implantation even within the critical period is recommended (20-22). Our results for a Korean population concur with this prior suggestion since the patients implanted under 2 yr of age showed a better performance compared to those implanted after 3 yr of age. On the contrary, Geers (4) reported that there is no additional benefit for early implantation within the critical period. According to their results, for children who received a cochlear implant between the ages of 2 and 4 yr, the age at implantation was not strongly associated with better speech perception, speech production, language or reading skills by the age of 8 yr. They suggested three reasons for their findings. 1) The age of 2 yr was not young enough to show the advantages of early implantation. 2) There may be an advantage to early implantation that is no longer apparent by the age of 8 yr. 3) The speech coding strategies that were available at the time of the study may not have had enough information for most children to achieve normal speech and language development no matter how young they were when they received the testing. Although we partially agree with their interpretations, the effect of age at implantation and that of maturation/development are likely to be more important considerations. By applying the percentile score instead of the absolute score, our results showed that there is a noticeable benefit associated with early cochlear implantation even within the critical period, which is consistent with the predictions of most audiologists and otolaryngologists.
Our current study has several limitations as well. We analyzed the CAP and K-PVT as our primary outcome measures, but these two methods alone cannot fully reflect the auditory and language performance of a child. Other testing batteries should have been included in the analysis. However, since the age of the children we tested in this study ranged from 12 months to 9 yr, several different auditory and language assessment methods were used according to the child's age. Only the two methods used in this study were available for the entire range of ages. Despite the limitations for reflecting the child's performance abilities, the measures we used allowed us to directly compare the results among the groups without converting the results into another scale. Second, there are additional factors that are known to be important for the development of post-implantation auditory and language performance such as the type of device implanted, the number of electrodes inserted, the speech processing strategy, the communication mode, and participation and support of the child's family during the rehabilitation (3, 7). Although we looked in to these factors for each group, we did not perform a multivariate analysis of these factors. However, we attempted to validate that these factors were not significantly different among the four groups.
In conclusion, many previous studies have evaluated the auditory and language performance according to the age at the time of cochlear implantation. However, some of their results according to the age at the time of implantation are confounded by the maturation/development effect. We attempted to overcome this problem by using the percentile score relative to the normal hearing population. The group implanted at a younger age showed significantly better receptive language abilities as compared to the group implanted at an older age. The percentile score reached a plateau 2-3 yr after implantation, although the score itself kept on improving. The patients implanted before 2 yr of age caught up with the normal hearing population after 2-3 yr. However, the children implanted after 3 yr caught up only to the 20th percentile of normal children even after 2-3 yr, and the children implanted after 3 yr are likely to maintain this level thereafter.
Therefore, our study showed that early implantation, within the critical period, was associated with better outcomes even in a Korean population. It seems that 2 yr of age is the critical time point to perform a cochlear implantation in a child.
 XML Download
XML Download