

 PDF
PDF Citation
Citation Print
Print



Introduction
Postoperative nausea and vomiting (PONV) are the most common and distressing side-effects following laparoscopic cholecystectomy (LC) [12]. Various factors contribute to the occurrence of PONV including patient factors, anesthetic techniques, and type and duration of surgical procedures [3]. Patients undergoing LC have a higher PONV risk, which can reach 72% [4]. PONV is one of the leading causes of postoperative patient dissatisfaction, and is also a major reason for readmission and prolonged hospital stay and increases health care costs [5]. In addition, preoperative fasting and severe PONV can result in complications such as wound dehiscence, dehydration, and electrolyte imbalances [6].
Perioperative administration of an adequate volume of intravenous (IV) fluid could correct the intravascular volume deficits that may reduce PONV and pain, without the side effects of pharmacological therapy [78]. Dexamethasone was found to reduce PONV due to its anti-emetic and anti-inflammatory properties, without significant complications [9].
Multimodal approaches of prophylactic therapy have been shown to improve PONV and pain management, as well as to reduce adverse events in high risk patients undergoing LC [10]. We hypothesized that a combination of dexamethasone and large volumes of fluid (super-hydration) would be more effective for the prophylaxis of PONV, and for reducing postoperative pain, than dexamethasone alone.
The effects of combined therapy of dexamethasone and intraoperative fluids have not been compared to those of dexamethasone alone in our study population. Thus, this study explored the efficacy and tolerability of IV dexamethasone plus super-hydration versus dexamethasone alone for PONV prophylaxis in female patients undergoing LC. The primary outcome was the incidence of PONV during the first 24 hours following surgery. Secondary outcomes included ondansetron consumption, visual analogue scale (VAS) pain scores, total consumption of rescue analgesic during the first postoperative 24 h, and the incidence of delayed complications that may accompany dexamethasone and super-hydration usage.
Go to : 
Materials and Methods
This prospective, randomized, double-blind, parallel assignment clinical trial was performed after receiving approval from the local ethics committee of the Faculty of Medicine, Assiut University (Assiut, Egypt), and was registered at ClinicalTrials. gov (ref: NCT02726308). Written informed consent was obtained from all participants. A total of 100 female patients with American Society of Anesthesiologists (ASA) physical status I or II, and aged between 20 and 50 years and who underwent elective LC from May 2015 to December 2015, were included. Exclusion criteria included use of steroids, antiemetics, or opioids during the last 3 days before surgery. Patients with liver, cardiac or renal diseases, pregnancy, or a body mass index (BMI) > 30 kg/m2 were also excluded.
Patients were randomly allocated to two groups (50 patients in each group). Randomization was based on computer-generated codes maintained in sequentially numbered opaque envelopes. Group DF received IV 5 mg dexamethasone just before induction of anesthesia plus 30 ml/kg Ringer's lactate solution (intraoperative), while group D received IV 5 mg dexamethasone just before induction plus 10 ml/kg Ringer's lactate solution (intraoperative). The fluids were prepared and infused by anesthesia assistants who were not involved in the study. To maintain blinding, the fluids were infused using a pump with the screen and solution bag covered. In the preoperative holding area, 2 mg IV midazolam was administered to all patients after insertion of the venous line. In the operating room, standard monitoring included electrocardiogram, noninvasive arterial blood pressure, arterial oxygen saturation, and end-tidal carbon dioxide.
The anesthetic technique was standardized for all patients, with anesthesia being induced with fentanyl 1.0 µg/kg and propofol 2–2.5 mg/kg. Then, 0.6 mg/kg rocuronium was administered to facilitate endotracheal intubation. Anesthesia was maintained with 2–3% sevoflurane in 50% oxygen/air. Volume-controlled ventilation was instituted and both tidal volume and respiratory rates were adjusted to maintain end-tidal CO2 at around 35 mmHg. If the heart rate or mean arterial pressure increased by > 20%, IV fentanyl 0.5 µg/kg was administered. The total intraoperative fentanyl requirement was recorded. Additional rocuronium (5–10 mg) was administered if clinically required to maintain an intraoperative train-of-four count of 2–3. If the surgical plan was changed to open cholecystectomy or the case became complicated due to severe hypotension or bleeding, the patient was excluded from the study.
After surgery, gastric contents were suctioned via an orogastric tube before extubation. Intravenous atropine 1 mg and neostigmine 2.5 mg were administered slowly IV to antagonize the residual effects of rocuronium and the trachea was extubated. In all patients, fluid administration was started in the operating theatre and completed by the end of surgery. The anesthesiologists who managed the patients were blinded to the group assignment.
Patients were then shifted to the post-anesthesia care unit (PACU) in a stable condition. Recovery was evaluated by modified Aldrete post-anesthesia recovery score, and the time required to achieve a score of 10 was recorded (time to PACU discharge). Patients were allowed to drink liquids as soon as requested.
Study measurements
A nurse blinded to the patient groups evaluated patients at 0, 6, and 24 h after surgery for symptoms of nausea, retching, or vomiting. PONV was classified as early if it occurred up to 6 h after surgery, and as late if it occurred between 6 and 24 h postoperatively. A verbal descriptive scale (VDS) was used to assess the severity of PONV as no PONV (grade 0), mild PONV (grade 1), moderate PONV (grade 2), or severe PONV (grade 3) [11]. The definitions of nausea, retching, and vomiting have been provided previously [12].
During the first 24 h postoperatively, the total number of patients who had nausea, vomiting, or retching was recorded. If patients were of grade 2 or 3, or requested an antiemetic, ondansetron (4 mg IV) was given slowly as a rescue antiemetic. Ondansetron consumption during the first 24 h postoperatively was calculated.
VAS pain scores (no pain = 0, worst possible pain = 10) used to assess postoperative pain. A nurse blinded to the patient allocation group evaluated the pain scores on arrival in the PACU and at 1, 4, 8, 12, and 24 h postoperatively. The 24 h aggregate pain scores were calculated. Intramuscular meperidine (1 mg/kg) was administered upon patient request or when the VAS score was > 3. The total consumption of rescue analgesic during the first 24 h postoperatively was recorded.
During the study period, patients were monitored closely for adverse events. They were followed-up at 1 week postoperatively by a surgeon who was not aware of the group to which the patients belonged. The surgeon recorded any delayed complications that may accompany dexamethasone usage, such as wound infection, delayed wound healing, and inflammation or discharge from the wound.
Statistical analysis
The primary outcome of this study was the incidence of PONV during the 24 h period following surgery. Based on a previous study, the incidence of PONV during the first 24 h was 55% following the use of pre-induction dexamethasone [13]. We expected a 20% reduction in PONV with the combined use of dexamethasone and fluids. A total of 42 patients per group were required to test for a difference in the proportion of patients with PONV, with a power of 80% and an α level of 0.05. We enrolled 50 patients per arm to allow for possible dropouts. Data were analyzed using SPSS software (ver. 17.0; SPSS Inc., Chicago, IL, USA). The normality of the data distribution was evaluated by the Kolmogorov Smirnov test. Outcome variables are presented as means (SD) and CI of the difference, or as numbers (%). For the statistical analysis, independent sample t-tests (for continuous variables) and chi-square and Fisher's exact tests (for categorical variables) were used. The significance level was set at P < 0.05.
Go to :
Results
A total of 100 female patients were enrolled in this study. Fig. 1 shows the CONSORT flow diagram. Table 1 shows that age, weight, ASA status, history of PONV or motion sickness, smoking, durations of surgery and anesthesia, intraoperative fentanyl requirement, and time to PACU discharge were not significantly different between groups.
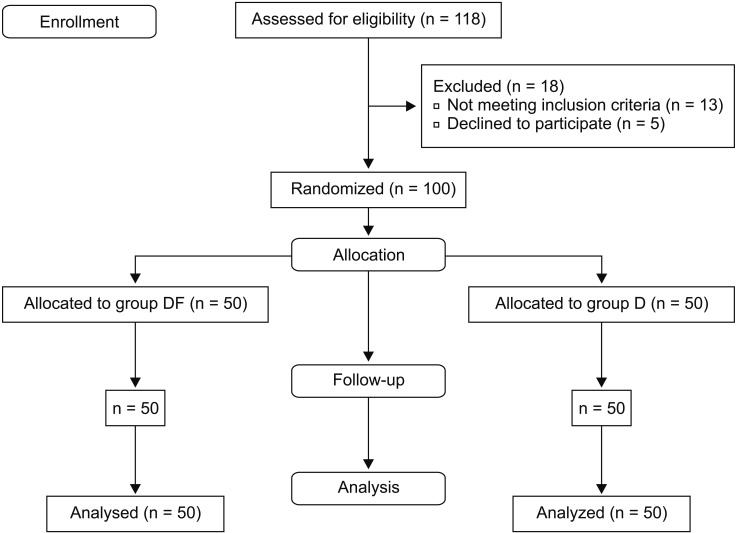
Table 1
Patients Demographic and Clinical Data
Data are represented as mean (SD) or numbers. Group DF: Dexamethasone plus hyper-hydration group, Group D: Dexamethasone group. ASA: American Society of Anesthesiologists, PONV: postoperative nausea and vomiting, PACU: post-anesthesia care unit. No significant difference between groups (P > 0.05) was observed for any variable.
![]()
The overall incidence of PONV during the first 24 h postoperatively was significantly decreased in group DF (22%) compared to group D (44%), with a P value of 0.03 (Table 2). However, there were no statistically significant differences between groups for the incidence of nausea, retching, or vomiting during the early (0–6 h) or late (6–24 h) postoperative periods (Figs. 2 and 3). Group DF had a lower odds ratio (0.359) of PONV, showing a CI of 0.150 to 0.858. Considering the severity of PONV during the first 24 h postoperatively, the number of patients having no nausea, retching, or vomiting (VDS score for PONV of 0) was increased significantly in group DF compared to group D (P = 0.03). However, there were no statistical differences in the number of patients in the other VDS scores for PONV, as shown in Table 2.
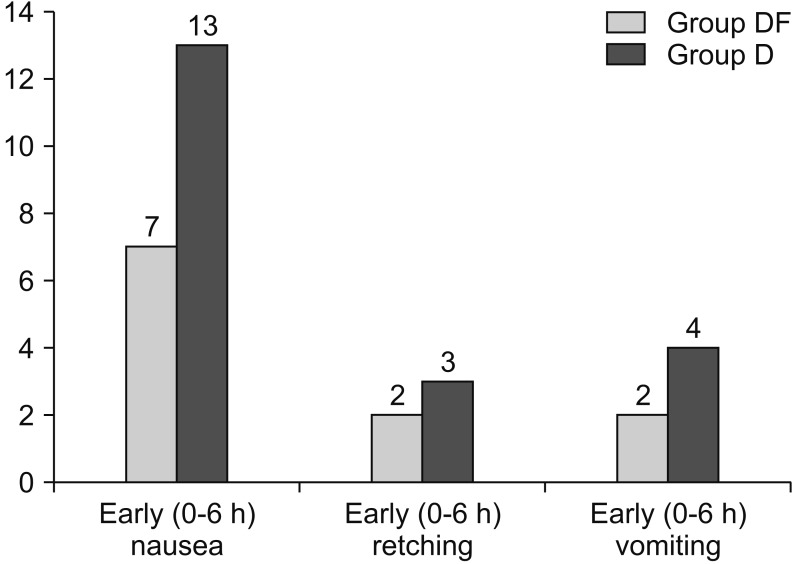 | Fig. 2Frequency of early (0–6 h) postoperative nausea, retching, and vomiting in both groups. Group DF: Dexamethasone plus hyperhydration group, Group D: Dexamethasone group. No statistical differences between groups were seen for the incidence of nausea, retching, or vomiting during the early postoperative period.
|
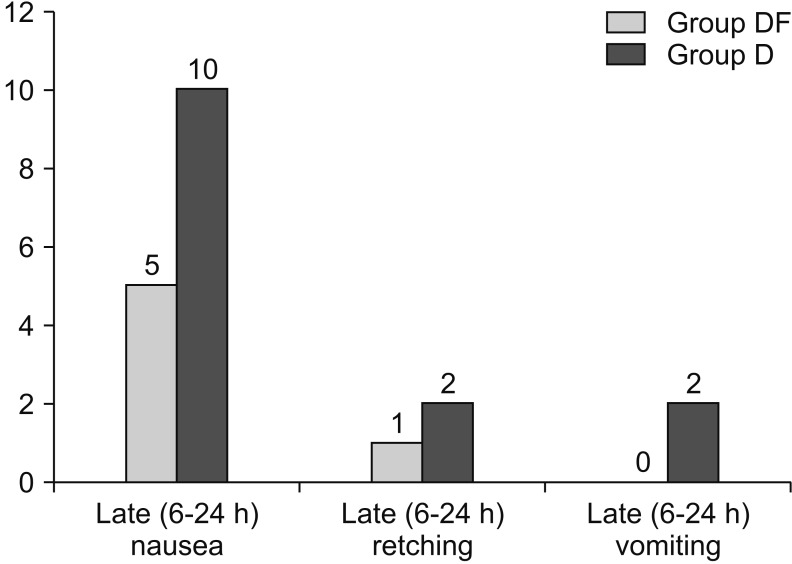 | Fig. 3Frequency of late (6–24 h) postoperative nausea, retching, and vomiting in both groups. Group DF: Dexamethasone plus hyperhydration group, Group D: Dexamethasone group. No significant differences between groups were seen for the occurrence of nausea, retching, or vomiting during the late postoperative period.
|
Table 2
Incidence and Severity of PONV and Antiemetics Use in the Dexamethasone Plus Hyper-hydration Group (Group DF) and Dexamethasone Group (Group D)
![]()
There was no significant difference between the groups regarding the number of patients requesting an antiemetic (6 patients in group DF vs. 14 patients in group D; P = 0.79). However, the mean ondansetron consumption was significantly lower in group DF (P < 0.001). The mean VAS pain score for the first 24 h postoperatively was significantly lower in group DF compared to group D (P < 0.001).
The time to the first meperidine request was significantly longer in group DF than group D (P < 0.001). In addition, total meperidine consumption during the first 24 h postoperatively was significantly lower in group DF compared to group D (P = 0.002) (Table 3). No patient was eliminated from the study due to conversion to open surgery or hemodynamic instability and no patient in either group experienced wound infection or any other wound complications at 1-week follow-up. No other adverse events were reported.
Table 3
Post-operative Pain Profile of the Dexamethasone Plus Hyper-hydration Group (Group DF) and Dexamethasone Group (Group D)
![]()
Go to :
Discussion
This study showed that the combined therapy of 5 mg dexamethasone and 30 ml/kg fluid reduced the incidence and severity of PONV and pain during the first 24 h after LC in female patients. In addition, it decreased the need for antiemetics and analgesics compared to the use of dexamethasone alone.
The incidence of PONV following laparoscopic surgery without prophylactic treatment can reach 88% [7]. This may be due to carbon dioxide insufflations during LC and intracranial pressure increases due to cerebral vasodilatation [14]. Our patients were at an increased risk for the development of PONV based on the risk score of Apfel [3]. This study attempted to eliminate the potential confounding factors that may contribute to the development of PONV, such as gender, history of PONV or motion sickness, nonsmoking status, postoperative opioid use, and the type and duration of anesthesia and surgery.
Prophylactic IV dexamethasone was reported to reduce the incidence of PONV and pain and decrease rescue antiemetic and analgesic requirements [14151617]. Furthermore, dexamethasone has been shown to decrease pain and fatigue, increase appetite, and improve mood and the overall quality of recovery during the first 24 h postoperatively [18]. Timing of dexamethasone is critical because it has a delayed onset. Prophylactic pre-induction administration of dexamethasone was more effective than administration at the conclusion of surgery [19]. In addition, it was more effective at decreasing late PONV due to its long half-life of 36–72 h [20]. A meta-analysis has provided good evidence that the use of 5 mg dexamethasone is clinically effective for prophylactic control of PONV when used alone or as combined therapy, as recommended by the Society of Ambulatory Anesthesia [9].
Several theories have been proposed to explain the antiemetic properties of dexamethasone such as endorphin release and antagonism of prostaglandin [4]. Moreover, dexamethasone has an anti-inflammatory action that may prevent the release of serotonin in the gut and tissue (and thus relieve pain), which is considered to be among the etiological factors of PONV [21]. Furthermore, dexamethasone is believed to reduce tissue damage and postoperative pain by suppressing fibrin deposition, capillary dilation, edema formation, and leukocyte migration [22].
Our findings support the superiority of combined use of super-hydration and dexamethasone for reducing PONV and pain compared to dexamethasone alone. Several studies have examined the effect of super-hydration on PONV in LC [7232425]. Some reports showed that perioperative super-hydration with 30 ml/kg crystalloid solution reduced the incidence of PONV and pain following laparoscopic surgery [2324]. Other studies showed that pre-operative fluid correction of intravascular volume deficits effectively reduced PONV during laparoscopic surgery [725]. Recently, Sayed et al. [26] provided support for the superiority of combined dexamethasone and super-hydration compared to each therapy alone for reducing PONV in children undergoing strabismus surgery. However, the study population and the type of surgery differ between our study and their work.
The mechanism underlying the reduction of PONV seen with supplemental fluid therapy remains unclear. During elective surgery, the combination of overnight fasting plus intraoperative fluid loss results in hypovolemia and a subsequent reduction in blood flow to the gut. If gut ischemia is not corrected, it will lead to the excessive release of serotonin, which can trigger PONV. Hence, fluids may reduce the incidence of PONV by improving mesenteric perfusion, preventing gut ischemia, and decreasing serotonin release. Indeed, large volumes of IV fluids have been found to decrease postoperative pain and analgesic requirements in high risk patients [5].
In contrast, other authors were unable to show a decrease in PONV after the administration of compound sodium lactate 1.5 ml/kg/h fasting time, with and without dextrose 0.5 g/kg, in patients undergoing diagnostic gynecologic laparoscopy [27]. Administration of other fluids, such as colloid or 0.9% saline, had a minimal effect on the incidence of PONV [28]. In addition, IV administration of crystalloid infusion (compound sodium lactate) 30 ml/kg to patients undergoing thyroidectomy did not decrease the incidence of PONV or antiemetic use compared with a 10 ml/kg dose [29]. However, our study differs from previous reports with respect to the dose and type of fluids used, as well as the surgical procedure.
Apfel et al. [5] suggested that supplementing with IV crystalloids is an inexpensive and simple non-pharmacological therapy to reduce the incidence of PONV, without any observable side effects of the fluids. Multimodal approaches for the management of PONV and pain using pharmacological and non-pharmacological interventions have been proposed to improve outcomes, provide synergistic effects, and decrease side effects of medications [10].
There are some limitaions of this study. We have no historical data on PONV incidence among untreated patients at our institution. Furthermore, we did not include a placebo control group in this study because this would be unethical, given that our study population were at an increased risk for PONV. In addition, we did not include a super-hydration treatment-only group due to the lack of evidence supporting its efficacy against PONV.
Based on our findings, we recommend the use of 5 mg dexamethasone (pre-induction) combined with 30 ml/kg Ringer's lactate (intraoperative) to achieve a reduction in PONV, VAS pain scores, and the requirement for antiemetics and analgesics during the first 24 h postoperatively. Furthermore, there were no reported adverse events using this regimen.
Go to :
 XML Download
XML Download