

 PDF
PDF Citation
Citation Print
Print



Introduction
The number of elderly patients undergoing cardiac surgery has been increasing in the last years. Some of these patients have a good clinical course, whereas others develop severe postoperative complications, with prolonged stay in the intensive care unit, and their postoperative quality of life often remains below expectations.
The functional reserves of various organs decrease with age and vulnerability to stress increases. This decline with age is called “frailty syndrome,” and does not begin at the same age in everybody. A number of medical, psychological and social factors can affect the body's physiology, such as unhealthy diet, vitamin and trace element deficiencies, lifestyle, lack of physical activity, and harmful job effects [1]. This syndrome has no objective diagnostic criteria, so it is difficult to assess and quantify its severity objectively.
The severity of frailty varies and is less pronounced in those with physically and intellectually active lives [1], and denying major surgery simply based on chronological age would be unfair to those in good physical condition. On the other hand, elderly subjects with increased vulnerability will probably suffer increased morbidity and mortality after surgery, with a decrease in quality of life, so the indication for surgery should always be weighed between postoperative gain and complications, and may be wise to offer less invasive alternatives or conservative treatment to these patients.
Risk scales, used to assess patients for cardiac anesthesia and surgery, often underestimate poor outcomes of the elderly, probably because the scores mainly consider comorbidities with less consideration of disabilities and functional reserves [23].
Many studies have tested the efficacy of frailty scales in older patients [23456] undergoing major surgery, but only a few have compared these scores with common risk stratification scores. Therefore, we conducted a prospective clinical study to compare two frailty scales with risk scales used in cardiac surgery and anesthesia to study which of these scores has better prognostic value regarding postoperative complications, length of stay in the intensive care unit (ICU) and hospital, length of mechanical ventilation and in-hospital postoperative mortality in patients scheduled for open heart surgery.
Materials and Methods
After approval of the Ethical Committee of the Cardiovascular Surgery Clinic, we conducted a prospective clinical trial, including patients ≥ 65 years who agreed to cooperate and who were scheduled for open heart surgery.
The anesthetist in charge calculated the Cardiac Anesthesia Risk Evaluation (CARE) score [7] and EuroScore II [8] at the preanesthetic assessment, and another researcher who was unaware of anesthetic and surgical risk scores, calculated the frailty scores using the Edmonton Frail Scale (Table 1) and the Clinical Frailty Scale (Table 2), which contain questions on lifestyle and the physical condition of patients.
We recorded patient age, body mass index, comorbidities, type and duration of surgery, postoperative complications, length of mechanical ventilation and hospitalization in the ICU and in the hospital, and in-hospital mortality rate (postoperative death occurring before hospital discharge).
Patients were mechanically ventilated until they were fully awake, hemodynamically stable, normothermic, and met extubation criteria (no residual neuromuscular blockade and stable gas exchange). Patients were discharged from the ICU when they had no organ dysfunction requiring technical support.
Statistical analysis was performed using MedCalc ver. 12.5.0.0 (http://www.medcalc.org/download.php), and GraphPad Prism ver. 6.0 software (GraphPad, Software Inc., La Jolla, CA, USA). Discrete variables are expressed as percentages and continuous variables are expressed as mean ± SD. The correlation between quantitative variables was assessed using Spearman's rho. To compare the predictive value of the severity scores, receiver-operating characteristic (ROC) curves were constructed and the area under the curve (AUC) was determined. A two-tailed P value < 0.05 was considered significant.
Results
We analyzed 57 patients, 19 (33.3%) women and 38 (66.7%) men; mean age 70.2 ± 4.3 years, range 65–81 years. Comorbidities, and type and length of surgical interventions are shown in Table 3. Only one patient was free of any associated disease.
The CARE and EuroScore II scores are calculated routinely during pre-anesthetic visits, but we faced some difficulties assessing frailty scores, as 6 of the 57 patients did not understand the questions asked and required repetition or exemplification, and 21 were undecided and gave different answers to the same repeated question.
Postoperative complications occurred in 25 patients (43.9%); renal dysfunction was the most frequent (n = 13), followed by liver (n = 8) and neurological (n = 6) dysfunction, and low cardiac output syndrome (n = 4). Four patients died due to multiple organ failure (mortality: 7%).
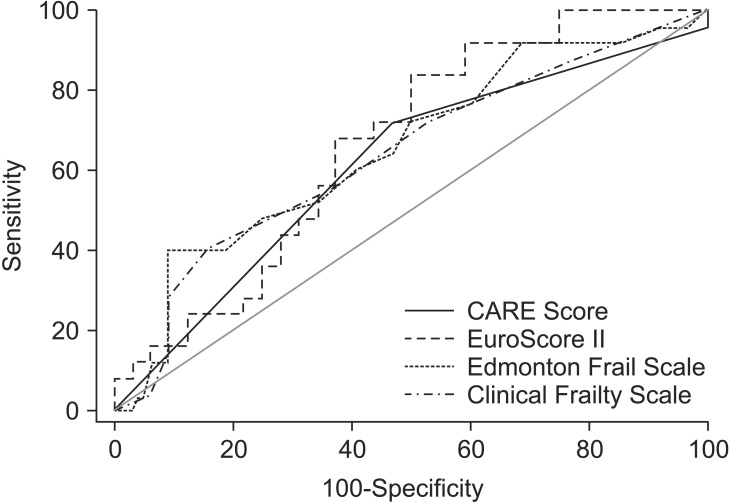
Therefore, We analyzed the prognostic value of the four scores predicting postoperative complications, and constructed ROC curves (Fig. 1, Table 4).
The AUC was higher for the EuroScore II and the Edmonton Frailty Scale (but < 0.7 for all risk scales, meaning low predictability), and the pairwise comparison of the ROC curves showed no significant differences.
We performed a univariate Spearman's correlation test to analyze the relationships between the different scores regarding length of mechanical ventilation and length of stay in the ICU and in the hospital, because the data did not follow a Gaussian distribution (Table 5). In the results, there were significant positive correlations between EuroScore II and length of mechanical ventilation and length of stay in the ICU. Significant correlations were detected between Edmonton Frail Scale, Clinical Frailty Scale and the length of mechanical ventilation.
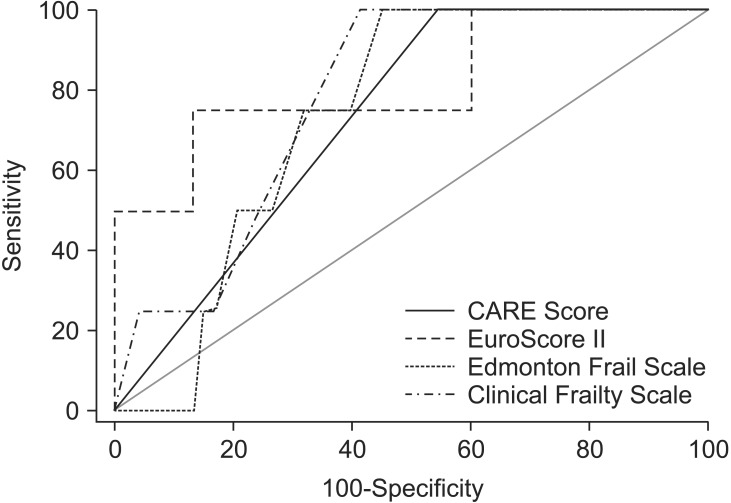
We analyzed the ROC curve and AUC for postoperative deaths, and found higher sensitivity for the EuroScore II (AUC 0.816), followed by the Clinical Frailty Scale (AUC 0.778) and the Edmonton Frail Scale (AUC 0.738). The pairwise comparison of the ROC curves showed no significant differences (Fig. 2, Table 6).
Discussion
More and more anesthetists and surgeons consider that the currently used risk scores underestimate postoperative risks in elderly patients with a high degree of frailty [39]. Consequently, many studies have attempted to find associations between frailty scores and postoperative morbidity and mortality in older patients undergoing major surgery. Most of these studies analyzed different frailty scales, whereas we compared two widely used scores in cardiac anesthesia (CARE and EuroScore II) and two frailty scales (Edmonton Frail Scale and Clinical Frailty Scale) that can be easily calculated.
In our study, the CARE score had the lowest sensitivity to predict postoperative complications, length of mechanical ventilation, lengths of stay in the ICU and the hospital, and in-hospital death. The CARE score is used frequently because of its simplicity, but no exact pathologies or surgical interventions are included; some uncontrolled medical problems or types of complex surgery are exemplified, but this leaves room for clinical judgement, which means different interpretations depending on the anesthetists' or surgeons' experience.
The EuroScore II is more complex and objective than the CARE score. Nonetheless, some studies have reported that a EuroScore II ≤ 6 overestimates mortality, and that one ≥ 13 underestimates it [26]. In our study, the EuroScore II had the highest predictability regarding postoperative outcome (postoperative complications and deaths) of the elderly patients, length of mechanical ventilation, and length of stay in the ICU. In addition to the severity of comorbidities and the type of surgery, the EuroScore II also evaluates musculoskeletal mobility and neurocognitive dysfunction, which reflect somewhat frail patients. This is probably why the prognostic value was better for the EuroScore II than for the CARE score, and was as efficient as the frailty scales for predicting length of mechanical ventilation.
The Clinical Frailty Scale and Edmonton Frail Scale are generally considered effective and have been studied by several authors [1310], but some of the questions on the scales can be interpreted differently by patients from different social or cultural backgrounds, so the calculated score may over- or underestimate the actual physical and cognitive condition of the patient. In addition, the Edmonton Frail Scale is more complex and more time-consuming to perform and it contains a series of questions (such as social support or medication) that are less relevant to the immediate postoperative course of patients. The overall condition of a patient who is depressed or anxious will likely be overestimated by the Edmonton Frail Scale. However, both frailty scales showed good predictability for length of mechanical ventilation, which depends on the patients' muscular strength. Age-related sarcopenia and sarcopenic obesity, as well as unintentional weight loss in the elderly, lead to progressive loss of muscle mass and strength, making weaning from mechanical ventilation more difficult [11121314]. Most of the frailty scores assess the patient's fitness and muscular strength, so they are a better predictor of length of mechanical ventilation than anesthetic scores.
The Edmonton Frail Scale has been studied in elderly patients undergoing orthopedic surgery, and the score is positively correlated with the occurrence of postoperative complications and length of hospital stay [15]. We found positive correlations only with the length of mechanical ventilation and in-hospital death in patients undergoing open heart surgery.
In a study involving 400 patients ≥ 75 years, Sündermann et al. [2] reported that patients with higher frailty scores had significantly higher mortality after major surgery. Other studies have shown that the number of complications, and lengths of stay in the ICU and in the hospital increase with increasing frailty, and that quality of life decreases in these patients during the late postoperative period [1]. Comparing the four scores, the EuroScore II (AUC 0.816) had the highest predictability for postoperative death, followed by the Clinical Frailty Scale (AUC 0.778) and the Edmonton Frail Scale (AUC 0.738), although the differences were not significant.
It is important to realize that the postoperative outcome of patients undergoing major surgery depends not only on frailty but also on the severity of any disabilities and comorbidities, which may be the reason why the EuroScore II had higher predictability than the frailty scores. Patients with high vulnerability have more comorbidities, which, in turn, can be predictors for adverse postoperative outcomes [3].
In conclusion, despite the use of different scores, it is difficult to predict postoperative complications and their severity in elderly patients, in which frailty is relatively common. The EuroScore II had higher predictability regarding the postoperative outcome of patients, length of mechanical ventilation, length of stay in the ICU and in-hospital death than the other scales, whereas the frailty scores correlated only with in-hospital death and length of mechanical ventilation, which depends on muscular strength.
A new risk stratification scoring system should be developed for elderly patients undergoing surgery, that include criteria for organ dysfunction, complexity of the surgical intervention, and an assessment of the patient's frailty and unintentional weight loss.
 XML Download
XML Download