

 PDF
PDF Citation
Citation Print
Print



We live in an epoch in which the twin crises of public health and the environment are merging. Climate change, particularly global warming, is exacerbating ill health across the world. Paradoxically, health care facilities are associated with environmental problems, as they represent a significant source of pollution around the world.
Most of the waste generated by healthcare facilities, which have many employees, is not very different from that generated by households. However, it is treated as regulated medical waste (RMW) that requires special waste treatment, such as incineration.
RMW, which has come into contact with the body fluids, blood, or tissues of patients, requires additional handling and processing for disposal. This waste poses a potential health risk as it includes infectious, sharp, pharmaceutical, or radioactive materials [1]. Non-regulated medical waste (non-RMW) is by definition not hazardous or contaminated and does not require additional handling and processing for disposal [2].
Most of the time, all hospital waste is considered to be infectious waste. If the waste is mixed, then all of the hospital waste is presumed to be infectious waste [3].
The majority of hospital RMW is produced in the operating room (OR), and it considerably consists of disposable packaging and wrapping materials for the sterilization of surgical instruments [4]. After examining the composition of this kind of waste, we found that a number of items had a recycling mark indicating that they were recyclable.
The objective of this study was to seek ways to reduce medical waste, and particulally the weight and volume of RMW.
We put the RMW and non-RMW from a number of surgeries in different bags, and asked the following questions:
(1) What is the weight and volume of RMW in the red bag?
(2) What is the weight and volume of non-RMW in the general bag?
Case Report
A waste audit provides both a qualitative and quantitative assessment. We performed a waste audit of 4 total knee replacement arthroplasties (TKRAs) and 1 total hip replacement arthroplasty (THRA), conducted at our hospital. The Hospital Research Ethics Board stated that this study did not require their approval. The five operations were performed in June 2015 by a team led by two orthopedic surgeons. Although the operating room personnel varied between the operations, they had all been informed of the procedure's inclusion in the waste audit in order to ensure that all waste would be disposed of in the OR for complete collection and analysis.
We classified the surgical waste into 3 types:
(Linen and liquids from suction containers were excluded from the study.)
1. Non-RMW: plastics, papers/cardboards, various wrapping materials
2. Blue wrap (used to hold sterilized instruments)
3. RMW
The data collection started as soon as the OR personnel began to prepare for the operation, and it ended when they disposed of their surgical attire and personal protective devices.
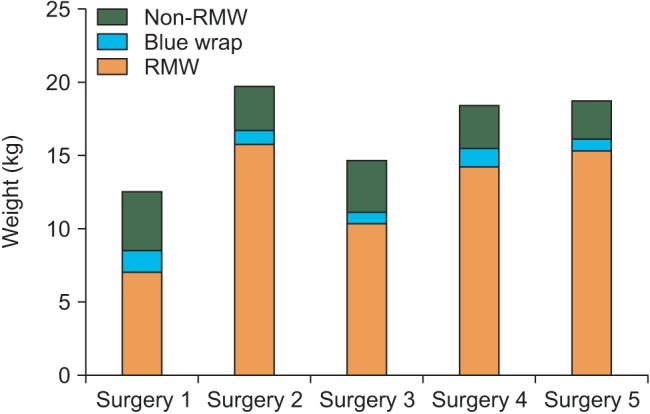
After the operation was completed and the patient left the OR, we weighed each type of waste and measured the volumes of the bags. The waste was weighed on a digital scale with an accuracy of 0.1 kg, and the volume was estimated using 30 and 90 L plastic bags. The weight of the surgical waste from the 5 operations totaled 84.4 kg, including 16.4 kg (19.4%) of non-RMW, 62.8 kg (74.4%) of RMW, and 5.2 kg (6.2%) of blue wrap (Fig. 1). The total weight of the non-RMW and blue wrap amounted to 21.6 kg (25.6%).
In the course of the audit, we noticed that much of the non-RMW was made up of recyclables, including papers, plastics, cardboards, and various wrapping materials. Originally, we only categorized the surgical waste into 2 types: non-RMW and RMW. However, we found that blue wrap was a major contributor to surgical waste. Therefore, we calculated the blue wrap's mass and volume separately from the rest of the non-RMW.
The volumes of the non-RMW, RMW, and blue wrap from the 5 operations were estimated roughly (Table 1).
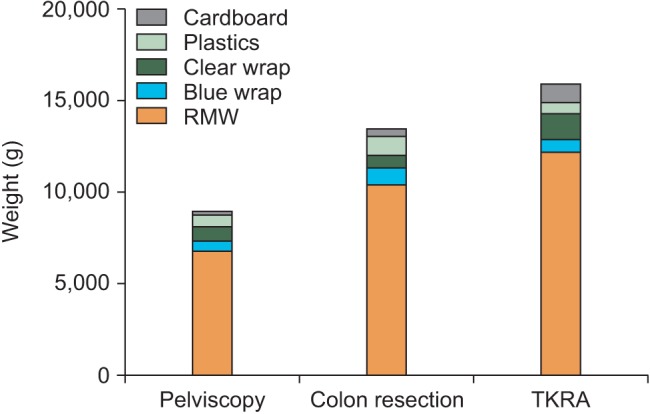
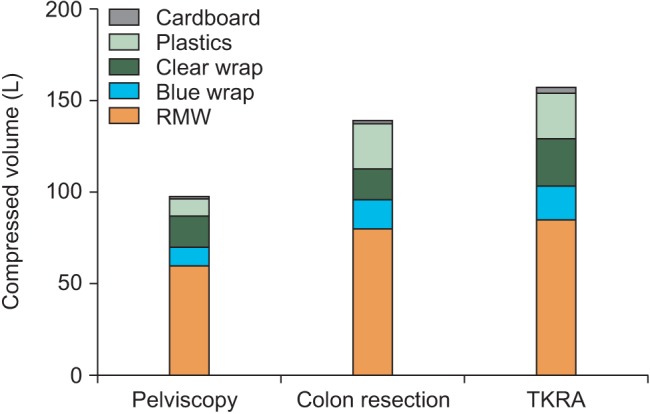
We performed 3 extra waste segregations of 1 TKRA, 1 laparoscopic anterior resection of the colon, and 1 pelviscopy (with radical vaginal hysterectomy) conducted at our OR in July 2016.
Discussion
One-third of all hospital RMW comes from the OR [5]. As the OR is a disproportionate contributor to hospital waste, it represents a high-yield target for segregation.
In 2010, the University of Pittsburgh Medical Center reduced 47% of the RMW generated in the OR, and was able to save around $89,000 [5]. The Carolinas Medical Center reported that it had saved an average of $158,000 USD (including $60,000 through the reduction of RMW, $2,000 from waterless scrubbing, and $33,000 through power down) by forming an internal Green Operating Room Committee [4]. Our study could not lay down the above figures. Research on the disposal of waste matter in Korean hospitals has been limited to the cost of RMW containers and disposal expenses (e.g., a 90 L RMW container costs 1,480 Korean won per box, disposal expenses come to 340 won per kg, and electron tag RFIDs cost 80 won each). Although the specific savings cannot be determined exactly, we may conclude that a considerable amount of environmental gain can be achieved by segregating non- RMW from RMW. According to the Johns Hopkins Hospital's go green initiative, only 24% of OR waste contains RMW, while the rest consists of non-RMW (59%) and recycled waste (17%) [6].
Financial and environmental concerns have been sparking an interest in hospital waste management and recycling programs [7]. The generation of medical waste from the healthcare industry has rapidly increased over the past decade. According to 2015 statistics from the Ministry of the Environment, around 147,600 tons of RMW were produced by Korean hospitals in 2012, and this amount has increased by about 10% every year since then. Seventy-nine thousand tons of RMW are generated around cities where incineration facilities can only dispose of 49,000 tons of RMW. Therefore, the remaining 30,000 tons of waste are subjected to long-distance travel. The segregation of medical waste and recycling in healthcare facilities may enable RMW treatment without expanding incineration facilities, which will help to cull environmental hazards.
Eight months have passed since the hospital at which this audit was conducted started to adopt waste segregation in the OR. In the past, the non-RMW was routinely thrown into the RMW stream, creating contaminated waste that generated extra costs for disposal. The most difficult part of our audit lay in the number of staffs required to carry it out. Most of the doctors and nurses felt that waste segregation was unnecessary as part of the OR flow and patient care.
Our research sample was limited by the lack of directing guidelines for waste segregation. We started the waste audit with operations in which a lot of recyclable materials were produced, with a view to extending the application of waste segregation to the entire OR. We believe that this small initiative is the first step toward the improvement of waste management in our hospital.
Due to the use of various prosthetics, implants, and their packages, large joint arthroplasty is a major contributor to OR waste production [8]. Moreover, total joint arthroplasty is one of the most frequent surgical procedures, and its frequency will continue to grow as the population ages. We advisedly selected the OR in which TKRAs and THRAs were performed to encourage waste segregation in staff members who were indifferent to it.
This waste audit drew results from the qualitative and quantitative analysis of 4 TKRAs and 1 THRA. We examined the proportion of non-RMW and blue wrap relative to the total waste.
These two waste streams totaled 21.6 kg, representing 25.6% of the total waste (84.4 kg).
In 2014, 105 TKRAs and 97 THRAs were completed by a team led by 2 orthopedic surgeons at our hospital. We estimated the possible weight reduction of RMW on that basis. We found that a RMW reduction of 872.6 kg was possible (as obtained with this calculation: 202 cases/5 cases x 21.6 kg) (Table 2).
Almost 20 years ago, Tieszen and Gruenberg [7] found that about 20% of hospital waste came from operating suites, and that 75% of non-infectious waste from operating suite packs could be recycled.
In comparison, the recyclable portion of our audit was very small.
The best medical waste management practice for medical facilities is to minimize the generation of waste. However, the potential for waste prevention and reduction at the point of generation is known to be somewhat limited due to the nature of the waste stream and the increased use of single-use disposable items [8].
Recycling is an effective way to reduce hospital waste.
One recyclable item that is frequently used in hospitals is sterilization wrapping (i.e., blue wrap), which is made of 100% polypropylene, a #5 plastic [9].
Finding appropriate recycling companies, particularly in regional areas where they are lacking, can be very challenging [10]. One solution may be to encourage medical device manufacturers interested in environmental issues to reduce the amount of packaging used or to change the materials used in order to reduce medical waste in a systemic way.
According to the present study, these changes and waste segregation, could help to achieve our goal to reduce RMW generation through non-RMW segregation.
Our audit presented some limitations: it only involved 8 sample operations, and the application of waste segregation to all operations raises challenges.
Furthermore, there is no recycling program and cooperative company at our hospital.
We performed our OR waste audit before implementing a recycling plan. It is necessary to start a broad audit with the goal to involve all staff before launching a recycling program.
Our waste audit showed that it is possible to reduce the amount of RMW through the segregation of waste in the OR. This gives us the opportunity to deliberately plan way to balance the importance of patient care with our impact on the environment.

 XML Download
XML Download