

 PDF
PDF Citation
Citation Print
Print


The loss of resistance (LOR) technique is the most commonly used technique for identifying the epidural space, which is based on different densities of tissues encountered as the needle tip passes through the thick ligamentum flavum into the loose epidural space. Air or liquid such as saline or local anesthetics are generally used for this technique. One of the causes of neurologic deficit after epidural injection is related to nerve root or spinal cord compression by the air used for LOR at the site adjacent to the epidural procedure [123]. However, there is no report of neurologic deficit in the distant region sparing the epidural procedure site, caused by the air used for LOR. We report a case of paraplegia without neurologic symptoms in the upper extremities following cervical epidural catheterization using the LOR to air technique.
Case Report
A 41-year-old woman was diagnosed with complex regional pain syndrome (CRPS) using the "Budapest" criteria [4] due to lower extremity pain after thigh contusion caused by dropping a heavy box on her thigh at work 28 months ago. She was admitted for a trial spinal cord stimulation (SCS) for treating her lower extremity pain that was resistant to multimodal pain treatments for 28 months after pain onset. Results of her blood tests including coagulation study were within normal ranges at the preoperative evaluation.
During her first visit to our clinic, she complained of lower extremity pain with pain sites gradually extending to her upper extremities. She underwent surgery for a trial SCS at the lower thoracic vertebral segment to alleviate her lower extremity pain, and her lower extremity pain score decreased moderately from 9 to 5 on the visual analog scale (VAS). However, on the 3rd day of the trial SCS she was still suffering from upper extremity pain and her upper extremity pain score was increased from 7 to 9 on the VAS despite oral analgesics and intermittent intravenous opioid rescue medication. Cervical epidural catheterization was planned for continuous administration of analgesics to manage her upper extremity pain.
The patient underwent cervical epidural catheterization with a 20-gauge catheter through an 18-gauge Tuohy needle at C7-T1 with LOR using air under fluoroscopic guidance. Total amount of air instilled into the epidural space was uncertain; however, the practitioner (4th grade of anesthesiology residency) recalled administering about 7 ml of air.
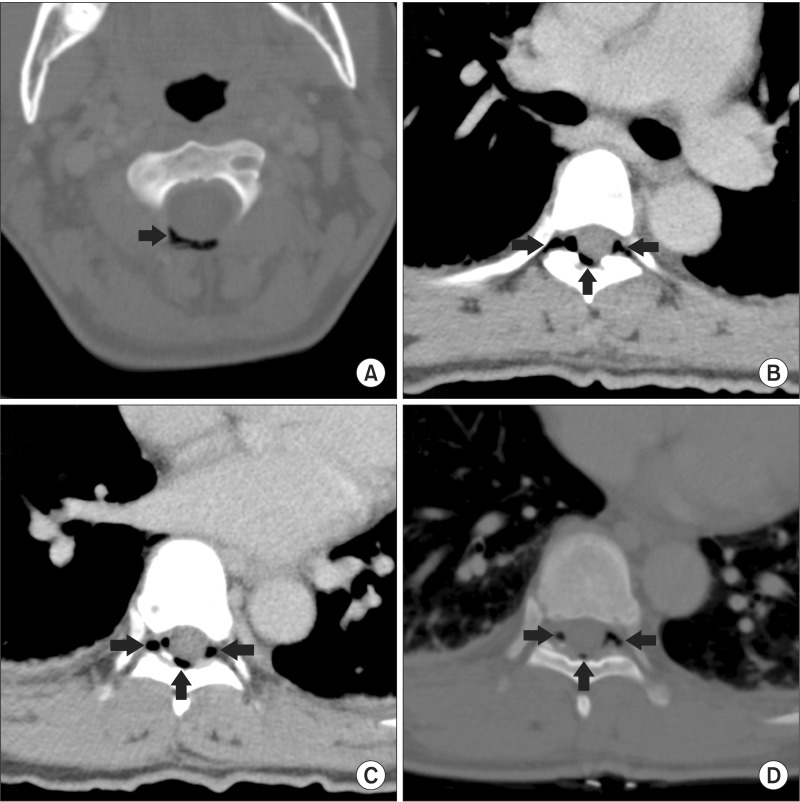
She was comfortable and able to ambulate in the in-patient ward after cervical epidural catheterization. Six hours after insertion of the cervical epidural catheter, she suddenly complained of hypoesthesia and motor weakness of both lower extremities. Neurologic assessment revealed markedly decreased sensation to pinprick, cold, and touch below the T10 dermatome and slight contraction of the leg and foot muscles without movement (grade 1/5). The authors suspected an epidural hematoma around the thoracic spine possibly related to the previous epidural procedures and considered whole spine magnetic resonance imaging (MRI) although she did not have typical pain accompanying an epidural hematoma. However, she had received a trial SCS lead and underwent whole spine CT. Definitive findings of whole spine CT scan were multifocal air densities in the epidural space, intervertebral foramen, and paraspinal muscles between C1 and T9 and no obvious spinal cord compression (Fig. 1). While evaluating the patient and performing CT scan within 1 hour, the sensation below the T10 dermatome was totally absent and muscle power of both lower extremities was zero with no contraction (0/5).
We consulted a neurosurgeon for emergent decompressive surgery although there was no obvious spinal cord compression due to a mass-like lesion such as epidural hematoma or abscess. Within 3 hours after the paraplegia developed, decompressive operation was started by targeting the insertion site of the trial SCS electrode at the lower thoracic spine first because the neurologic deficit developed below the T10 level. However, there was no hematoma or abnormal findings in the epidural space where the trial SCS electrode was placed at T9–12. The radiologist and the authors thought that multifocal air collection in the epidural space and intervertebral foramen could be the cause of paraplegia, and a decompressive operation in the cervical spine was performed immediately after the closure of the thoracic spine. As soon as the cervical epidural space was opened, the neurosurgeon noticed escape of air bubbles with the naked eye and there was no hematoma or any other lesion.
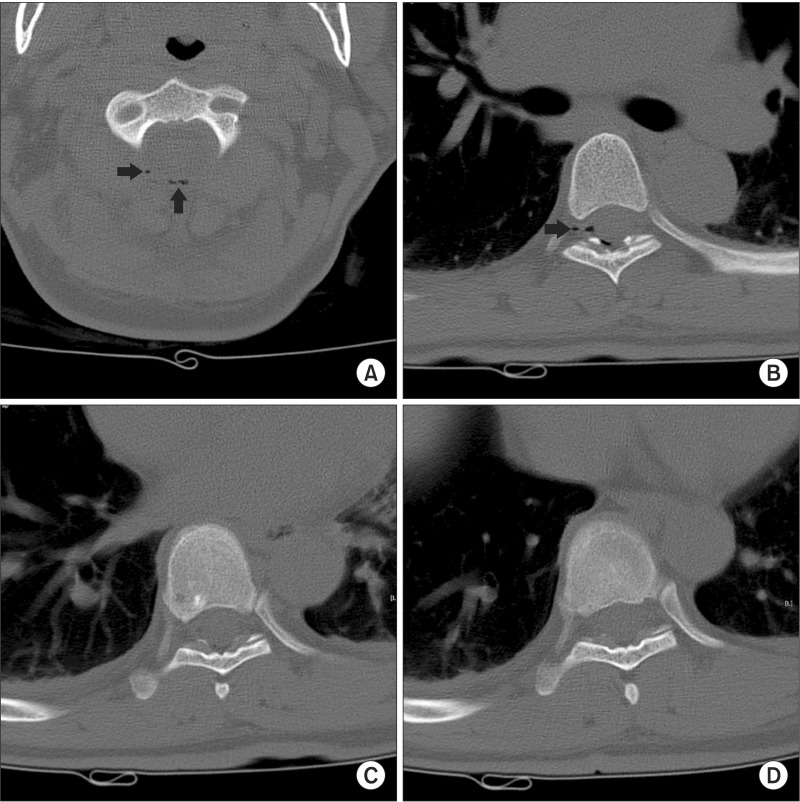
Immediately after the decompressive surgery, the patient underwent whole spine MRI for evaluation of the spinal cord and epidural space. There were no findings of spinal cord ischemia on the whole spine MRI. Her sensation and motor function recovered to normal immediately after she awoke in the post-anesthesia care unit. The following day, whole spine CT was performed and it revealed nearly complete disappearance of epidural and paravertebral air (Fig. 2). One month after this incident, she underwent SCS for the management of pain in the lower extremities.
Discussion
The causes of paraplegia following an epidural procedure include; first, mechanical compression of the spinal cord from outside due to an epidural hematoma or abscess, second, spinal cord ischemia due to vascular insufficiency due to a thrombus, embolus, or spasm of medullary arteries, and third, direct spinal cord trauma or neurotoxicity [56]. In this case, the cause of paraplegia was presumed to be delayed epidural hematoma or abscess that developed three days after the placement of the thoracic epidural lead for a trial SCS, or epidural hematoma or spinal cord ischemia related to cervical epidural catheterization six hours before the paraplegia developed, when the authors examined the patient immediately after she developed paraplegia.
Although the etiology often remains ambiguous, MRI would be the best tool for assessing the epidural space and spinal cord condition [7]. However, a CT scan was performed urgently to preserve the thoracic epidural lead for trial SCS in our case. The radiologist opined that there was no obvious compressive lesion around the spinal cord such as a hematoma or abscess in the whole spine, and found multifocal air collection in the epidural space, intervertebral foramen, and paraspinal regions between C1 and T9. The neurosurgeon and the authors decided to promptly perform decompressive operation in the thoracic spine although there was no clear evidence of causes of spinal cord compression on the CT scan because the patient's neurological deficit progressed rapidly below the T10 dermatome in the final hour before the surgery.
In our case, there was no obvious hematoma or other compressive pathology in the cervical and thoracic epidural space under the operative field and the only thing observed by the neurosurgeon with the naked eye was escape of air bubbles through the opening site of the cervical epidural space. On comparing the pre- and post-operative CT, multifocal distribution of air especially in the intervertebral foramen of the thoracic spine without obvious mechanical compression of the spinal cord noted in the pre-operative CT had almost disappeared in the postoperative CT. Heo et al. [8] demonstrated that most spinal segmental arteries from T8 to L4 passed the middle portion of the vertebral body and about 2/3 of the segmental arteries between T8 and T11 were located in the upper portion of the intervertebral foramen. In judgment based on the distribution of air in the intervertebral foramen and no mechanical compression of the thecal sac, we presumed that transient interruption of the blood supply to the spinal cord possibly occurred through compression of segmental radiculomedullary arteries by epidural air at the thoracic level of the intervertebral foramen or possibly increased epidural compartment pressure due to obstruction of lateral transforaminal outlet flow with air entrapment [9].
The critical factors for neurological outcome in case of mechanical compression of the spinal cord by an epidural hematoma are known to be the level of the preoperative neurological deficit and the time interval between onset of symptoms and surgical decompression [10]. Generally, neurologic outcome would be more favorable when the decompressive operation is performed as early as possible. Bitar et al. [11] found that a maximum three-hour period of ischemia would be the limit for recovery of the spinal cord, which they called "critical ischemia time" using a dog model of vascular clamping of the spinal anterior artery. In our case, the decompressive operation was performed within three hours, which resulted in an immediate and complete recovery of the neurological deficit.
All reported complications of paresis or paraplegia caused by epidural air are related with lumbar epidural block or catheterization using a large volume of air for LOR [123]. Among the reported adverse symptoms resulting from an epidural block using air for LOR, only 2 ml of air for LOR would produce inadequate analgesia or bilateral limited leg mobility with pain at the lumbar epidural injection site [1213]. Although there is still no consensus on whether air or saline would be superior for LOR, it is generally accepted that a small amount of air should be used for the procedure. Based on previous reports, we can consider that the amount of air for LOR should be as small as possible with a volume of less than 2 ml. Furthermore, contrast flows of 5 ml volume at the C7-T1 cervical epidural injection site have been reported to spread to an average of 11.0 ± 3.7 vertebral levels [14]. The spreading of instilled air into the cervical epidural space is not known but air may spread further, as in this case.
In conclusion, it should be remembered that the cervical epidural procedure can cause paraplegia without neurologic deficit of upper extremities. To prevent neurologic complications related with the use of air for LOR for epidural procedures, use of the smallest dose of air and frequent check up with contrast media under fluoroscopy to confirm the correct epidural space are necessary.
 XML Download
XML Download