

 PDF
PDF Citation
Citation Print
Print


Introduction
Postoperative nausea and vomiting (PONV) is a distressing adverse effect that may result in postoperative complications including bleeding, wound dehiscence, aspiration pneumonitis, and fluid and electrolyte imbalances [1]. The incidence of PONV ranges from 22%–52% despite advance in anesthetics and anesthesia techniques [234]. The etiology of PONV remains unclear, but the contributing factors are complex including gender, smoking, a history of motion sickness or previous PONV, anesthetic technique, type of surgery, and the use of opioids [5]. Among the risk factors of PONV, the use of postoperative opioids is one of the four major risk factors in the simplified risk scoring system devised by Apfel et al. [6]. The use of postoperative opioids strongly affects the incidence of PONV in a doserelated manner [7]. In the Society for Ambulatory Anesthesia Consensus Guidelines for the management of PONV, one of the strategies for reducing the baseline risk factors of PONV is the minimization of intraoperative and postoperative opioid use [5].
In addition to postoperative analgesia, opioids have often been used to reduce the hemodynamic response to laryngoscopy and tracheal intubation or to blunt surgical stimulation during anesthesia management. Most anesthesiologists prefer shortacting opioids such as remifentanil or fentanyl rather than longacting opioids for this purpose because long-acting opioids may cause postoperative adverse effects including respiratory depression, PONV, urinary retention, and pruritus. Therefore, smalldose fentanyl or remifentanil infusion is commonly employed to reduce the hemodynamic response to tracheal intubation during anesthesia induction or to ablate responsiveness to noxious intraoperative stimuli as a balanced anesthesia concept [891011].
Although a number of clinical reports have identified the use of postoperative opioids as one of the major risk factors of PONV, few studies have been performed that focus on the effects of intraoperative opioid use on the incidence and severity of PONV [121314]. Furthermore, studies regarding the effects of a single bolus administration of fentanyl during anesthesia induction or the intraoperative infusion of remifentanil on PONV are rare. We conducted a prospective, randomized, double-blinded study to compare the incidence and severity of PONV in female patients undergoing thyroidectomy who received a single bolus intravenous administration of fentanyl during anesthesia induction or infusion of remifentanil during the operation.
Materials and Methods
This study was approved by the Institutional Review Board of author's institution and registered with the WHO International Clinical Trials Registry Platform (KCT0001126). After obtaining written informed consent, 250 female patients, aged 20–65 years and American Society of Anesthesiologists physical status I or II, undergoing thyroidectomy were enrolled in this prospective study. Patients with a history of motion sickness or PONV, diabetes mellitus or gastrointestinal disease, and those who were smokers, menstruating, or who had taken antiemetics or steroids within 72 h prior to surgery were excluded from the study. Because the four major risk factors are female gender, non-smoking, use of postoperative opioids, and prior history of motion sickness or PONV according to Apfel's simplified risk scoring system [6], the enrolled patients in this study had two risk factors of PONV. Patients were allocated randomly to one of three groups: the control group (Group C), 2 µg/kg of a single bolus administration of fentanyl during anesthesia induction (Group F), or 2 ng/ml of effect-site concentration of remifentanil with a target-controlled infusion (Group R) using computergenerated random numbers.
The anesthetic regimen was standardized for all patients. No patient received preanesthetic medication. All patients were monitored by electrocardiography, noninvasive blood pressure, temperature, pulse oximetry, and capnography. Anesthesia was induced with thiopental sodium 4–6 mg/kg and rocuronium 1.0 mg/kg. Anesthesia was maintained with sevoflurane and 50% nitrous oxide in oxygen. End-tidal carbon dioxide partial pressure was maintained at 30–35 mmHg. The arterial blood pressure was kept within 20% of the preanesthetic values. Sevoflurane was administered to maintain an end-tidal sevoflurane concentration of 0.5%–3.0% according to blood pressure. Endtidal sevoflurane concentration was recorded every 5 min. A balanced salt solution was infused at a rate of 4 to 6 ml/kg/h during surgery except in cases of overt intraoperative blood loss. At the completion of surgery, inhalational anesthetics and remifentanil infusion were stopped. Residual neuromuscular blockade was antagonized with glycopyrrolate and pyridostigmine, and the trachea was extubated. Patients were administered 30 mg of ketorolac intravenously upon closure of the skin. Although the anesthesiologists in the operating room were not blinded to the group assignment, the data-collecting anesthesiologists in the postanesthesia care unit (PACU) and the ward, who did not perform the anesthetic management in the operating room, were blinded to the group allocations.
To assess nausea and vomiting, patients were monitored for 2 h in the PACU and interviewed in the ward at postoperative 6 and 24 h. PONV during periods 0 to 2 h, 2 to 6 h, and 6 to 24 h after anesthesia was evaluated by an anesthesiologist blinded to the study groups or by the spontaneous complaints of the patients. Nausea was defined as a subjectively unpleasant sensation associated with an awareness of the urge to vomit, and vomiting was defined as the forceful expulsion of gastric contents from the mouth. Rescue antiemetics were given immediately when the patients showed vomiting or required rescue medications. The first-line rescue antiemetic was ondansetron 4 mg, which was followed by metoclopramide 10 mg as a second-line treatment.
Any episode of nausea or vomiting during the 24 h period following surgery was considered an occurrence of PONV. Nausea severity was recorded using a Visual Analog Scale (nausea-VAS; where 0 cm = no nausea and 10 cm = worst possible nausea) at postoperative 2, 6, and 24 h. Vomiting was assessed by the number of vomiting occurrences. The incidence and severity of PONV and administration of rescue antiemetics were recorded. In addition to 2, 6, and 24 h, PONV was noted any time a patient complained of nausea or vomiting in the PACU or ward. The amount and time of administration of rescue antiemetics were recorded. Postoperative pain was evaluated using a VAS (pain-VAS; where 0 cm = no pain and 10 cm = worst possible pain), simultaneously. Patients received intravenous ketorolac as a rescue analgesic when required.
Statistics
The sample size was predetermined by the Proportions Sample Size using SigmaPlot 12.0 (Systat Software Inc. San Jose, USA) based on the assumption that the incidence of PONV, which was regarded as the primary endpoint, would be 35% in Group C and 60% in Groups F and R. It was ascertained that 70 patients were required in each group with a significance level of 0.05 (α = 0.05) and a power of 80% (β = 0.20). To allow for attrition, the total sample size was enlarged to 250.
Statistical analysis was performed with SigmaPlot 12.0. Continuous variables were analyzed with one-way analysis of variance. The incidence of PONV and use of rescue antiemetics were analyzed using the Chi-square test. The Holm-Sidak method and the Bonferroni correction were used for multiple comparisons after the ANOVA test and the Chi-square test, respectively. All data are expressed as mean ± standard deviation, or patient number and percentage. A P value of less than 0.05 was considered statistically significant.
Results
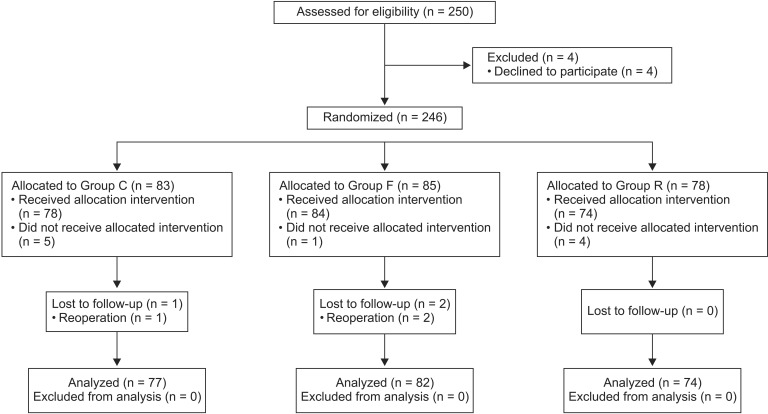
Two hundred and thirty-three patients completed the study, and the subject flow diagram is shown in Fig. 1. The three groups were comparable for patient characteristics, anesthesia time, and volume of fluids administered (Table 1). The doses of intraoperative opioids were fentanyl 120 ± 17 µg and remifentanil 283 ± 98 µg in patient Groups F and R, respectively.
The incidence of PONV and use of rescue antiemetics are listed in Table 2. Patients who received fentanyl during anesthesia induction (Group F) showed higher incidences of nausea (adjusted P = 0.013) and use of rescue antiemetics (adjusted P = 0.003) compared with Group C at 0–2 h. However, there were no significant differences in the incidences of PONV and use of rescue antiemetics between Groups C and R during the first postoperative 24 h. The overall incidences of PONV were 55, 73, and 59% in Groups C, F, and R, respectively (P = 0.008). There was a significant difference between Groups C and F (adjusted P = 0.003), but no difference between groups C and R (adjusted P = 0.279) for 24 h. No significant differences were shown in the PONV-VAS for those patients who had PONV (Table 3). There were no differences in the pain-VAS among the three groups in each time period (Table 4). The end-tidal sevoflurane concentrations during the operation were lowest in Group R (Fig. 2). No patients showed opioid-related complications, such as respiratory depression, urinary retention, or pruritus in Groups F and R.
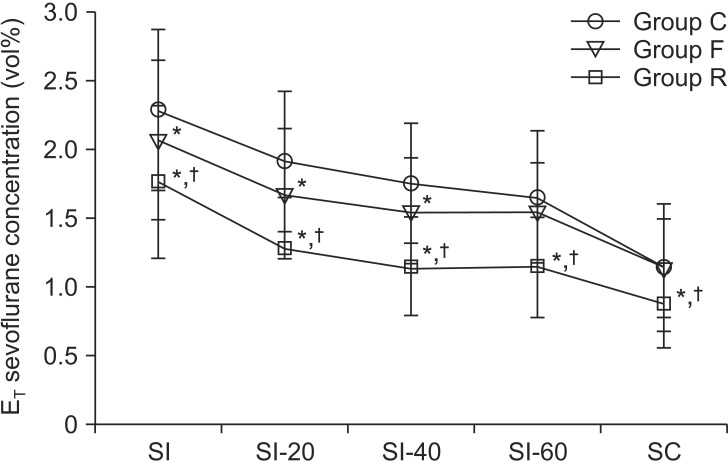
Fig. 2
The end-tidal (ET) sevoflurane concentrations were lower in Groups F and R compared with Group C from skin incision to 40 min after skin incision. In Group R, end-tidal sevoflurane concentrations were lower throughout the operation compared with Groups C and F. *P < 0.05 compared with Group C. †P < 0.05 compared with Group F. SI: Skin incision, SI-20: 20 min after skin incision, SI-40: 40 min after skin incision. SC: Skin closure.
![]()
Discussion
This study examined the emetic effects of a single bolus fentanyl administration during anesthesia induction and intraoperative continuous infusion of remifentanil on PONV. In the current study, there were no significant differences in the incidence and severity of PONV and requirement of rescue antiemetics in patients who received intraoperative remifentanil infusion compared with control patients. The overall incidences of PONV were 55% in the control group and 59% in the remifentanil group. These incidences were similar to those of previous studies of PONV after thyroidectomy [15]. However, patients who received 2 µg/kg of fentanyl during anesthesia induction showed higher incidences of PONV compared with control patients.
Because opioids commonly cause nausea and vomiting, the use of opioids is one of the major risk factors of PONV. Therefore, anesthesia strategies to avoid or reduce administration of opioids are effective means of reducing the risk for PONV. In fact, consensus guidelines for the management of PONV recommend the minimization of intraoperative and postoperative opioid use for the management of PONV [5]. Although a few studies have reported the effects of intraoperative opioid use on the incidence of PONV, the results were controversial [161718]. These previous studies had small numbers of subjects, and the opioids were used for postoperative analgesia. These may affect the interpretation of the results. Therefore, large prospective study that excludes the effect of postoperative opioids is required to demonstrate the effect of intraoperative opioids on PONV.
A single bolus administration of small-dose fentanyl has been used to reduce the hemodynamic response to tracheal intubation 3–5 min before intubation [9]. Fentanyl concentration at the effect site peaks 3.6 min after the bolus injection, which is 17% of the initial plasma concentration [919]. At 120 min after the bolus injection, the mean anesthesia time of the current study, the relative effect-site fentanyl concentration is approximately 10% of the peak effect-site concentration [19]. Because remifentanil is hydrolyzed by nonspecific esterase and has a very short context-sensitive half-time, the time required for a 50% reduction in the effect-site concentration of remifentanil was very short (3.65 min) regardless infusion duration [20]. Although the effect-site concentrations of fentanyl and remifentanil were not compared at the early postoperative period, the differences of PONV incidence between Groups F and R may have been influenced by effect-site concentrations. Although there were no differences in PONV among the volatile anesthetics isoflurane, sevoflurane, and desflurane, volatile anesthetics are known to have emetogenic effects [2122]. The vomiting incidence of volatile anesthetics was different from propofol in the early postoperative period and the difference is dose-related [23]. Sevoflurane consumption was less in Group R than Group F during operation. The lower use of sevoflurane in Group R may have influenced the incidence of PONV compared with Group F. However, the PONV incidence was higher in Group F than Group C, although the sevoflurane consumption was less in Group F. This result demonstrates that the residual effect of fentanyl influenced PONV more than emetogenic effect of sevoflurane. Intraoperative hypotension can affect the incidence of PONV. Because blood pressure was kept within 20% of the preanesthetic values by adjusting the sevoflurane administration, intraoperative blood pressure may not have affected the incidence of PONV in this study.
In this study, the contributing factors of PONV were controlled among the groups including patient demographic characteristics, surgical procedure, history of motion sickness and/or previous PONV, smoking, inhalational anesthetics, and postoperative use of analgesics. By eliminating the factors that affect PONV, the results of this study could therefore be attributed to the study setting. To exclude the effect of postoperative opioid use on PONV, intravenous ketorolac without opioids was administered for postoperative analgesia. Although inadequate analgesia was concerned, the pain score was maintained at less than 4.
Patients undergoing thyroidectomy have a remarkably high incidence of PONV when no prophylactic antiemetic is given [15]. The cause of the high PONV incidence after thyroidectomy is not known, but it may be related to several factors, including the age and sex of patients and vagal stimulation through surgical handling of the neck. Several studies have demonstrated the preventive effects of propofol on PONV compared with inhalational anesthetics [4,232425]. In patients undergoing thyroidectomy, avoiding volatile anesthetics and nitrous oxide and using propofol for the induction and maintenance of anesthesia can considered for anesthesia management to reduce PONV.
There is a limitation of the current study. The subjects were not administered prophylactic antiemetics, which could be considered unethical. However, the patients were under close observation and received antiemetic rescue medications immediately when the patients showed vomiting or required rescue medications.
In conclusion, the current study demonstrated that a single bolus administration of 2 µg/kg of fentanyl during anesthesia induction increased the incidence of PONV, but intraoperative remifentanil infusion with 2 ng/ml of effect-site concentration did not affect the incidence and severity of PONV.
 XML Download
XML Download